
1. Research Background

Ulcerative colitis (UC) is a chronic intestinal disease that severely affects the quality of life of patients and significantly increases the risk of colorectal cancer (CAC) associated with colitis, posing a major threat to patient survival. Current treatment strategies for UC are limited by single therapeutic mechanisms, uncontrolled drug release, and non-specific distribution, leading to poor clinical efficacy and significant adverse reactions. Furthermore, the long-term lack of disease remission exacerbates the risk of malignant transformation, making the development of novel and effective treatment strategies an urgent need. Oral probiotics have gained widespread attention in recent years as a promising biotherapy strategy. Surface modification techniques, such as metal-phenolic networks (MPN), can enhance the activity, adhesion, and gut microbiota regulation of probiotics in the gastrointestinal tract. For example, the biocompatible coating formed by tannic acid (TA)-Fe3+ complexes can protect probiotics from external threats such as ultraviolet light, lysosomal enzymes, and antibiotics, while providing probiotics with strong tissue adhesion through multivalent non-covalent interactions with the intestinal mucosal surface via catechol groups. However, the selective colonization of MPN-modified probiotics at lesion sites still faces challenges, and the severe inflammatory infiltration at UC lesion sites can disrupt the intestinal mucosal barrier, leading to mucosal erosion and ulcers, which limits the efficacy of probiotic therapy. Currently, no strategy has been developed to combine the selective colonization of probiotics at lesion sites with on-demand activation of chemotherapeutic methods, highlighting the urgent need for more effective comprehensive treatment strategies to address the complex pathological mechanisms of UC.
2. Design Concept
We developed a triggerable probiotic-drug conjugate that integrates probiotic protection, site-specific colonization, and pathological responsive anti-inflammatory drug release functions. This strategy utilizes natural polyphenol tannic acid (TA) and Fe3+ to form a sticky inner coating in situ on the surface of probiotic Escherichia coli Nissle 1917 (EcN), enhancing its colonization ability in the gut, regulating gut microbiota, and competitively inhibiting pathogenic bacteria. The outer layer consists of a reactive oxygen species (ROS)-responsive thioether bridge phospholipid-tanshinone (PSL), forming a protective lipid coating. After oral administration, this conjugate can protect probiotics from harsh gastrointestinal conditions such as gastric acid, proteases, and bile salts, significantly improving the survival rate of EcN. Upon reaching the colonic lesion site, high levels of pathological ROS trigger the cleavage of the thioether bonds in PSL, releasing tanshinone and the coated probiotics. Tanshinone has anti-inflammatory and scavenging activity, effectively improving the inflammatory microenvironment at the lesion site and synergistically enhancing the therapeutic effect with probiotics. In mouse models of ulcerative colitis (UC) and severe colitis-associated colorectal cancer (CAC), this strategy demonstrated significant therapeutic effects, further validating its clinical value. This innovative approach provides a new idea for UC treatment, combining the advantages of probiotic therapy and drug release, promising more efficient and precise treatment options for patients.
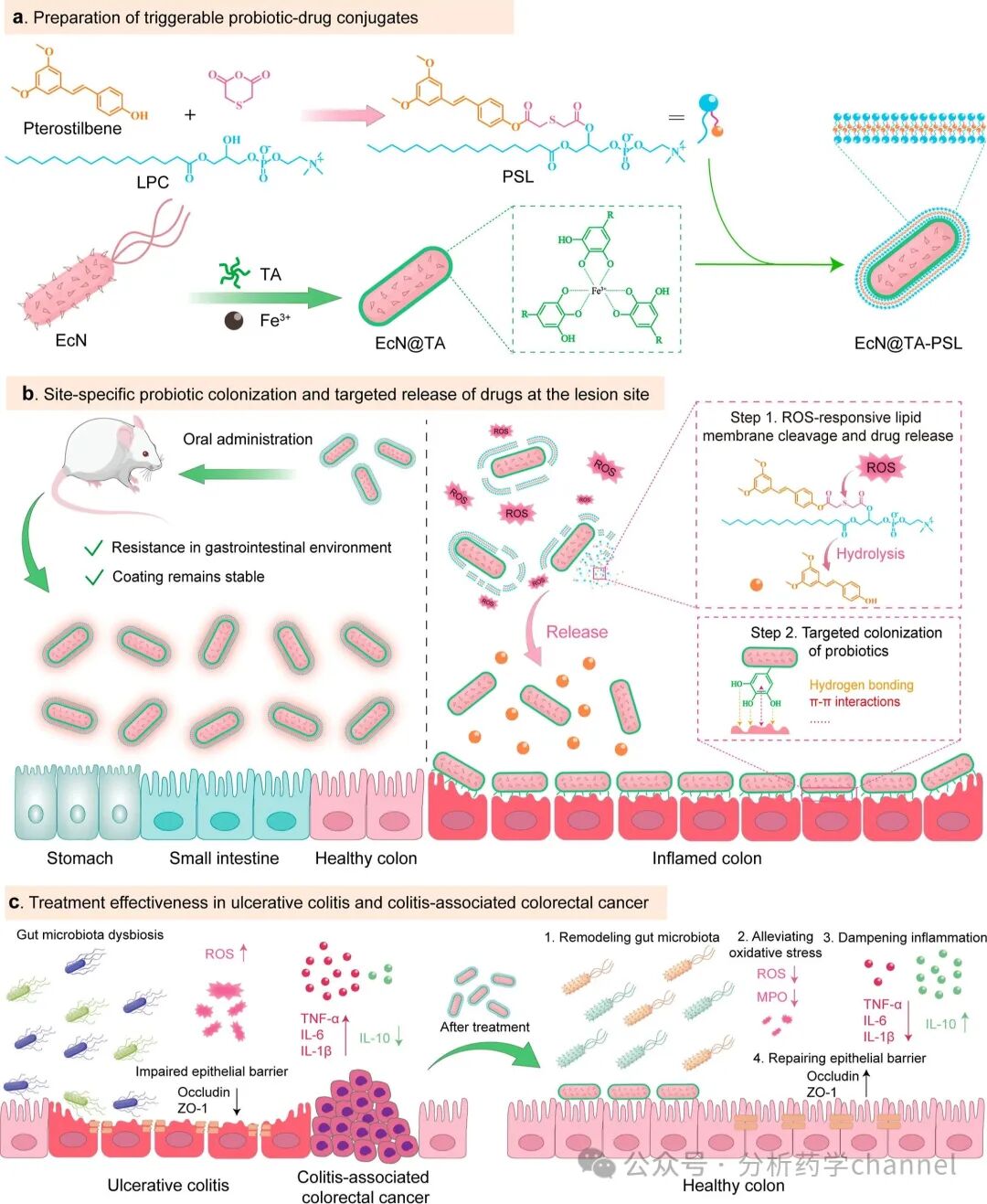
Figure 1. Schematic diagram of the triggerable probiotic-drug conjugate and its therapeutic mechanism for UC and CAC. (a) Synthesis schematic of ROS-responsive PSL and preparation process of EcN@TA-PSL. (b) Schematic diagram of EcN-specific colonization and targeted release of tanshinone at colonic lesion sites. (c) Therapeutic effects of EcN@TA-PSL in UC and CAC mouse models.
3. Results and Discussion
3.1 Design, Preparation, and Characterization of Probiotic-Drug Conjugates
To investigate the key pathogenic mechanisms of ulcerative colitis (UC), we performed bioinformatics analysis on multiple publicly available RNA-seq datasets (GSE87473, GSE92415, and GSE165512), comparing the gene expression profiles of inflamed tissues from UC patients and healthy controls. Through integrative analysis, we identified common differentially expressed genes (DEGs) and found that these genes were significantly enriched in biological processes such as “response to bacteria,” indicating that dysbiosis plays a key role in the pathogenesis of UC. Additionally, KEGG pathway analysis showed that DEGs were mainly involved in inflammation-related pathways, such as cytokine-cytokine receptor interaction, chemokine signaling pathway, IL-17 signaling pathway, and TNF signaling pathway, which are closely related to the severity of inflammation in the colonic tissues of UC patients. Based on these findings, we developed a triggerable probiotic-drug conjugate for the co-delivery of probiotics and the anti-inflammatory drug tanshinone to the intestinal lesion sites. This conjugate consists of an inner TA-Fe3+ coating and an outer ROS-responsive PSL (thioether bridge phospholipid-tanshinone). The TA-Fe3+ coating enhances the colonization ability of probiotics EcN through coordination interactions, while PSL cleaves under high ROS levels at lesion sites, releasing tanshinone and probiotics. Through a layer-by-layer coating procedure, we successfully prepared the conjugate EcN@TA-PSL and verified its structure and function. Transmission electron microscopy (TEM) and dynamic light scattering (DLS) results showed that the coating significantly increased the particle size and zeta potential of EcN. Confocal laser scanning microscopy (CLSM) and flow cytometry (FCM) further confirmed the successful encapsulation of the coating. High-performance liquid chromatography (HPLC) analysis indicated that the loading efficiency of tanshinone was 1.98 mg/1×10^9 CFU EcN. Bacterial viability staining and growth curve experiments showed that the coating had no significant effect on the viability and proliferation of EcN. In summary, this conjugate combines the advantages of probiotic therapy and drug release, providing an efficient and precise new strategy for UC treatment.
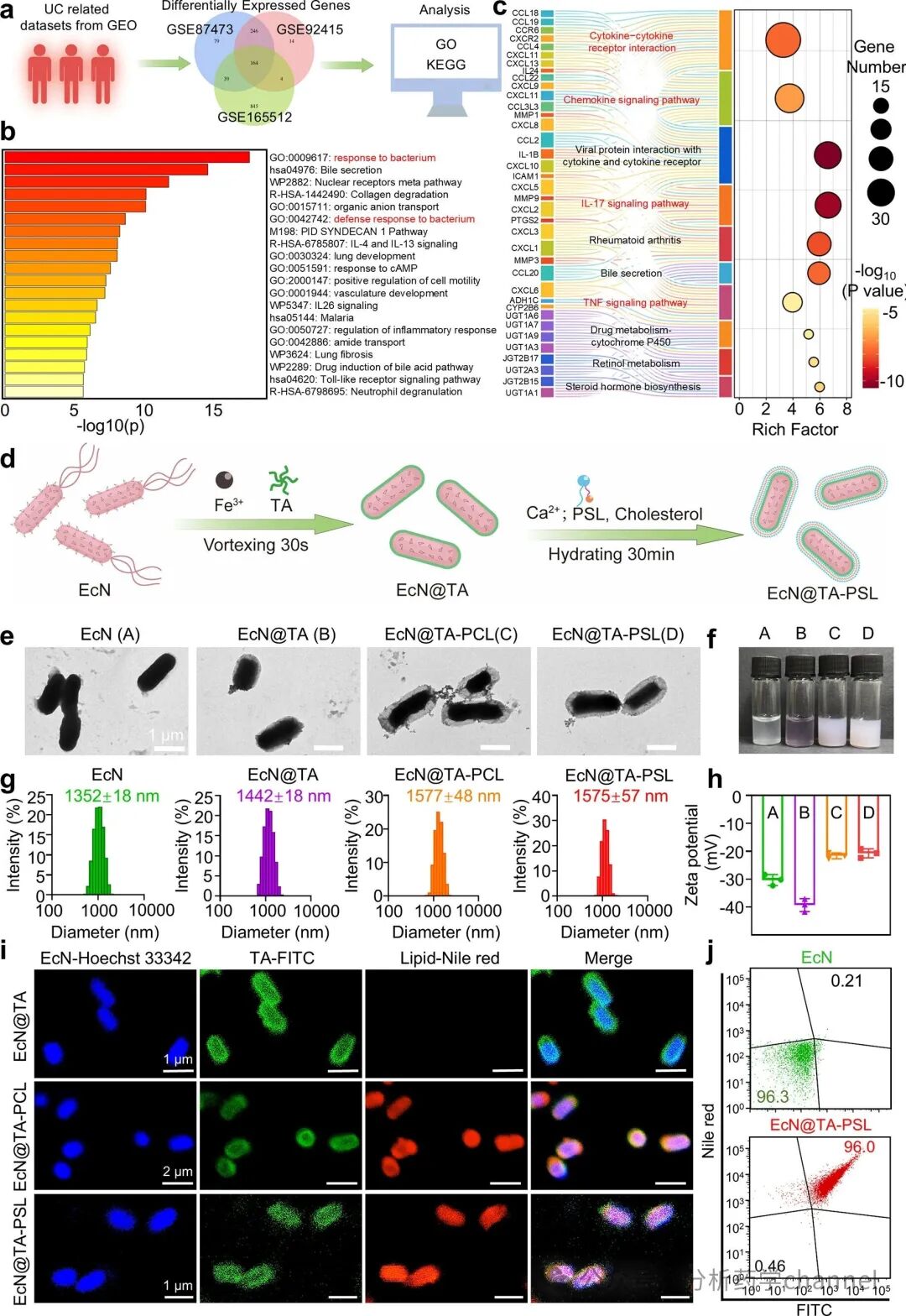
Figure 2. Design, preparation, and characterization of the conjugate. (a) Schematic diagram of bioinformatics analysis of publicly sequenced datasets related to UC. (b) GO and KEGG analysis of common differentially expressed genes in UC patients and healthy controls across three datasets (GSE87473, GSE92415, and GSE165512). (c) Preparation process of EcN@TA-PSL. (d) Representative TEM images of natural EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL. (e) Visual appearance of EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL (n = 3). (f) Size distribution (g) and zeta potential (h) of EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL. (i) Representative CLSM images of EcN@TA, EcN@TA-PCL, and EcN@TA-PSL. Blue: EcN labeled with Hoechst 33342. Green: TA coating labeled with FITC. Red: lipid coating labeled with Nile Red. (j) FCM histograms of EcN@TA-PSL prepared using FITC-labeled TA coating and Nile Red-labeled lipid coating, using natural EcN as a control. Data are presented as mean ± standard deviation.
3.2 In Vitro Protection and Stability
To evaluate the protective effect of the probiotic-drug conjugate in simulated harsh gastrointestinal environments, we compared the survival rates of natural EcN and the conjugate under simulated gastric fluid (SGF), simulated intestinal fluid (SIF), and bile salt treatment. The results showed that the survival rate of natural EcN was only 6.2% after 0.5 hours of incubation in SGF, while the survival rates of EcN@TA and the conjugate increased to 23.9% and 40.8%, respectively. As the incubation time was extended to 2 hours, natural EcN was almost completely inactivated, while the conjugate maintained significant viability, with a survival rate 3.5 times higher than that of EcN@TA. TEM images showed severe cell shrinkage and lysis of natural EcN after SGF treatment, while the conjugate maintained intact bacterial morphology. Under SIF and bile salt treatment, the conjugate also exhibited significant protective effects, with survival rates 5.5 times and 5 times higher than natural EcN, respectively. Furthermore, in simulated gastrointestinal continuous exposure experiments, the survival rate of the conjugate was approximately 5 times higher than that of EcN@TA, further confirming its superior protective ability.
The stability of the coating is a key factor in protecting probiotics. TEM and CLSM analyses indicated that EcN@TA gradually thinned and completely degraded after 2 hours of exposure in SGF, while the conjugate maintained structural integrity throughout the treatment period due to the protective outer lipid coating. FCM analysis further confirmed that the fluorescence intensity of the coating after SGF, SIF, and bile salt treatment remained significantly higher than that of EcN@TA, with no significant difference from the pre-treatment level. These results indicate that the conjugate not only significantly improved the survival rate of probiotics in harsh gastrointestinal environments but also achieved targeted delivery of probiotics and drugs through a stable coating structure.
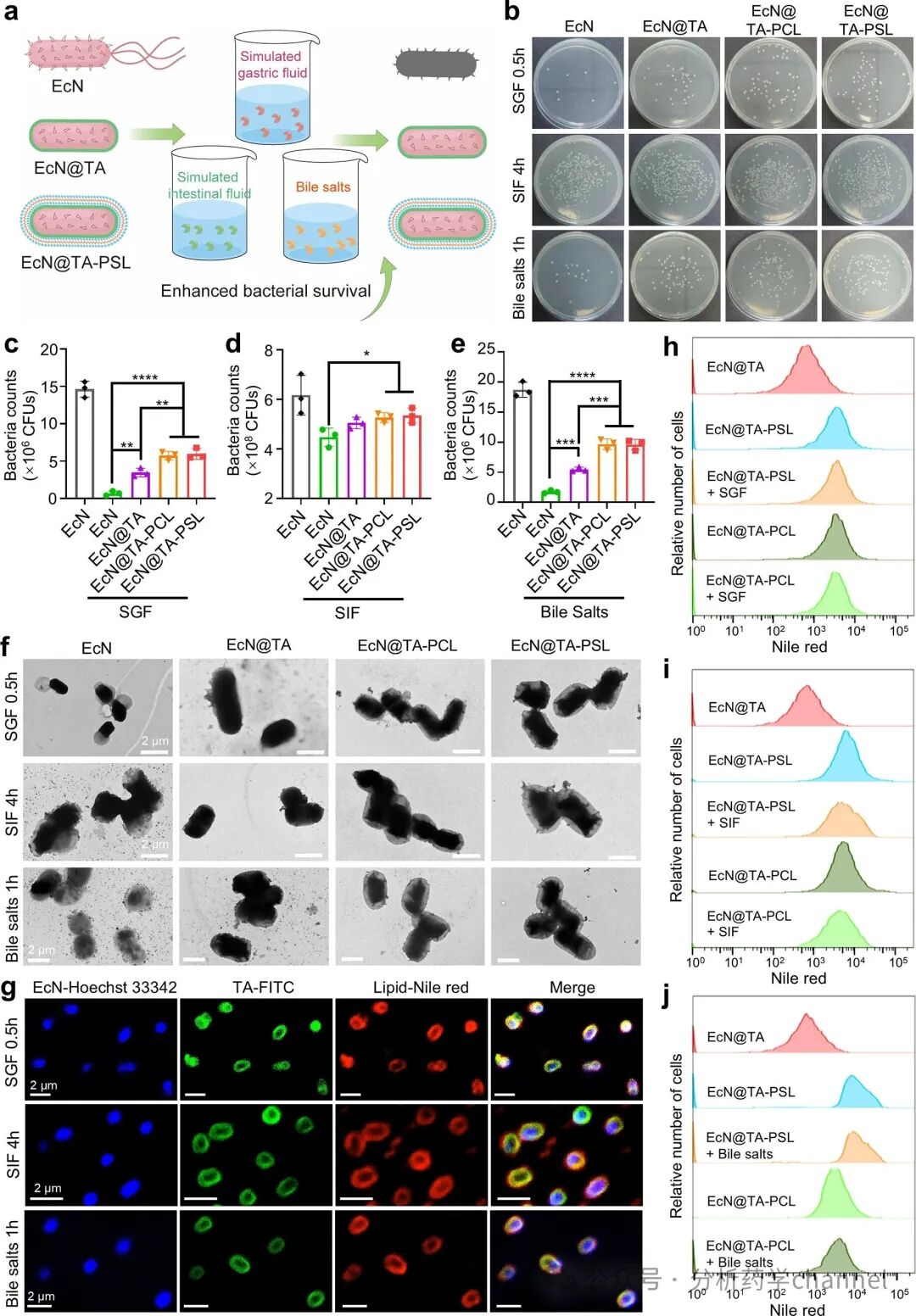
Figure 3. In vitro protection and stability of the conjugate. (a) Schematic diagram of the enhanced ability of the conjugate probiotics to withstand gastrointestinal conditions in vitro. (b) Photos of bacterial colonies formed on agar plates of natural EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL after incubation with SGF for 0.5 hours, SIF for 4 hours, or bile salts for 1 hour. Survival rates of natural EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL after treatment with SGF for 0.5 hours (c), SIF for 4 hours (d), or bile salts for 1 hour (e) (n = 3). (f) Representative TEM images of EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL after incubation with SGF for 0.5 hours, SIF for 4 hours, or bile salts for 1 hour. (g) Representative CLSM images of EcN@TA-PSL after incubation with SGF for 0.5 hours, SIF for 4 hours, or bile salts for 1 hour. Blue: EcN labeled with Hoechst 33342. Green: TA coating labeled with FITC. Red: lipid coating labeled with Nile Red. FCM histograms of EcN@TA-PCL and EcN@TA-PSL after incubation with SGF for 0.5 hours, SIF for 4 hours, or bile salts for 1 hour (j). Data are presented as mean ± standard deviation. Statistical analysis was assessed using one-way ANOVA and Tukey’s multiple comparison test (EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL).
3.3 In Vitro ROS Triggered Dissociation and Ex Vivo Reactive Adhesion
To utilize the significantly elevated levels of reactive oxygen species (ROS) at ulcerative colitis (UC) lesion sites, we developed an ROS-responsive conjugate EcN@TA-PSL, whose outer PSL (thioether bridge phospholipid-tanshinone) can be oxidized to hydrophilic sulfone in an ROS environment, thereby triggering drug release and probiotic colonization. In vitro experiments indicated that the release rate of tanshinone from EcN@TA-PSL significantly increased with the concentration of H₂O₂. Under 10 mM H₂O₂ stimulation, tanshinone was almost completely released within 8 hours, while the ROS non-responsive EcN@TA-PCL released only about 10% of the drug under the same conditions. Furthermore, even in the presence of 500 μM glutathione (GSH), the drug release from EcN@TA-PSL remained below 20%, indicating its ROS response specificity. TEM and CLSM analyses further confirmed that the PSL layer dissociated under H₂O₂ stimulation, exposing the TA coating, while the TA layer remained stable in the ROS environment, providing a basis for targeted colonization of probiotics.
To evaluate the in vivo adhesion capability of the conjugate, we co-cultured Dir-labeled EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL with mouse intestinal segments and human colonic tissues after incubation with 100 μM H₂O₂ for 12 hours. In vivo imaging system (IVIS) showed that the fluorescence intensity of the H₂O₂-treated EcN@TA-PSL group on the intestinal mucosa was significantly higher than that of the other groups, indicating its excellent tissue adhesion capability. Plate counting experiments further confirmed that the viability of EcN@TA-PSL after H₂O₂ treatment was 1.4 times higher than that of the EcN@TA group. Frozen section analysis showed that the H₂O₂-treated EcN@TA-PSL group exhibited the highest bacterial adhesion on the mucosal surface, attributed to the abundant catechol groups in the TA coating.
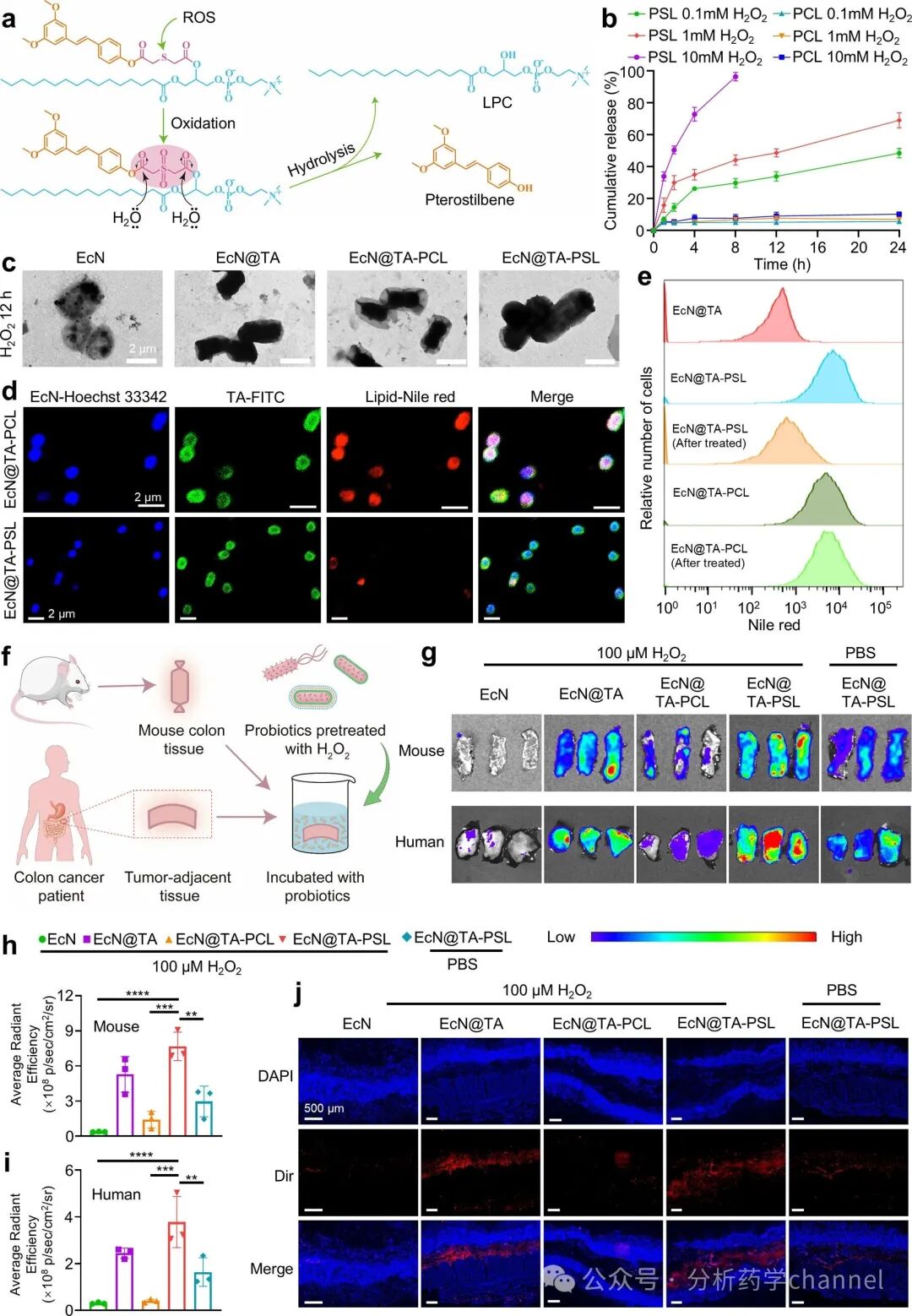
Figure 4. Dissociation, drug release, and ex vivo tissue adhesion of the ROS-triggered conjugate. (a) ROS response mechanism of PSL. (b) Cumulative release curves of tanshinone from EcN@TA-PCL and EcN@TA-PSL under 100 μM, 1 mM, and 10 mM H₂O₂ treatment (n = 3). (c) Typical TEM images of EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL after 12 hours of treatment with 100 μM H₂O₂. (d) CLSM images of EcN@TA-PCL and EcN@TA-PSL after 12 hours of treatment with 100 μM H₂O₂. (e) FCM histograms of EcN@TA-PCL and EcN@TA-PSL after 12 hours of treatment with 100 μM H₂O₂. (f) Schematic diagram of the responsive adhesion of probiotics to mouse and human ex vivo colonic tissues. (g) After 24 hours of incubation with 100 μM H₂O₂, EcN@TA and EcN@TA-PSL were co-cultured with fresh mouse intestine or ex vivo human colonic tissues for 1 hour, with EcN@TA-PSL without H₂O₂ treatment as a control. The average fluorescence intensity of Dir-labeled probiotics retained on mouse (h) or human (i) colonic tissues (n = 3). (j) CLSM images of Dir-labeled probiotics penetrating into human colonic tissues. Blue: intestinal villus nuclei stained with DAPI, red: Dir-labeled probiotics. Scale bar: 500 μm. Data are presented as mean ± standard deviation. Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with H₂O₂ treatment as control).
3.4 In Vivo Targeted Colonization of the Conjugate
To evaluate the targeted adhesion and colonization ability of the conjugate in ulcerative colitis (UC) models, we induced UC in mice using 3% DSS and orally administered Dir-labeled EcN, EcN@TA, EcN@TA-PCL, or EcN@TA-PSL. IVIS results showed that the fluorescence intensity of the uncoated EcN group was significantly lower than that of the other groups after 2 hours, indicating the protective effect of the coating on EcN. At 6 and 12 hours, the EcN@TA group exhibited the highest fluorescence intensity, highlighting the strong adhesion capability of the TA layer. After 24 and 48 hours, the fluorescence signals of the EcN@TA-PCL and healthy control group (EcN@TA-PSL-Con) significantly weakened, while the EcN@TA and EcN@TA-PSL groups maintained strong fluorescence signals, indicating their excellent colonic targeting and stability.
Ex vivo colonic imaging further confirmed that at 6 hours, the fluorescence intensity of the EcN@TA-PSL group was 1.9 times higher than that of the EcN@TA group, indicating that the ROS-responsive conjugate could achieve colonic-specific adhesion. After 48 hours, the fluorescence intensity of the EcN@TA-PSL group was 9.7 times, 1.9 times, 6.4 times, and 3.4 times higher than that of the EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL-Con groups, respectively, indicating its significantly enhanced colonization ability at colonic lesion sites. Moreover, no fluorescence signals were detected in major organs, confirming the high safety of the conjugate.
Through plate counting with ampicillin and CLSM analysis, we further verified the targeted colonization ability of EcN@TA-PSL at colonic lesion sites. The results showed that the EcN@TA-PSL group had the highest bacterial count in the colon, being 7.3 times, 1.7 times, 3.4 times, and 2.8 times higher than the EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL-Con groups, respectively. CLSM images showed that the EcN@TA-PSL group exhibited the strongest fluorescence intensity in the inflamed areas, while the EcN@TA-PCL group showed no significant fluorescence in the inflamed areas, and the fluorescence intensity of the EcN@TA group was similar in both inflamed and non-inflamed areas.
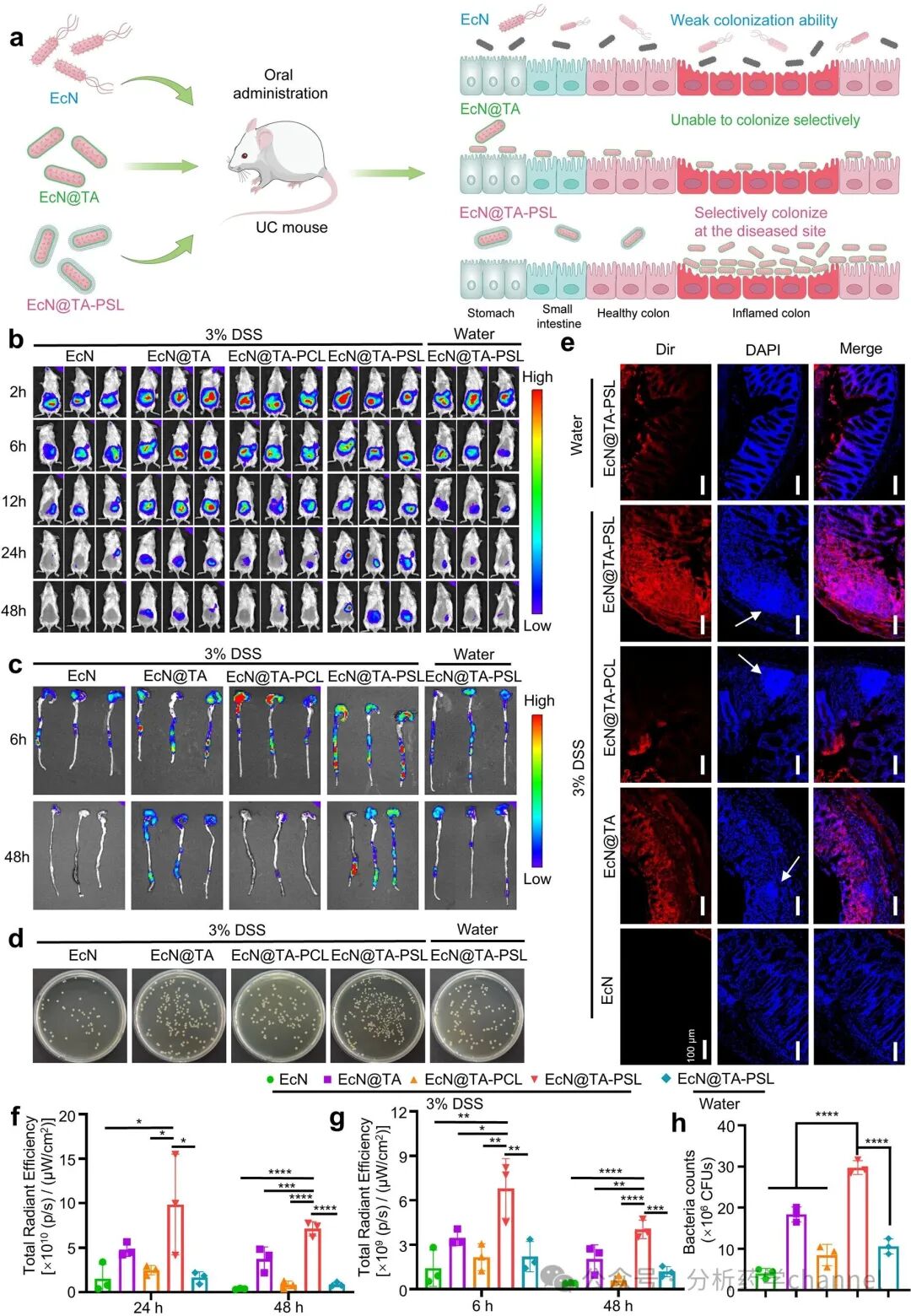
Figure 5. In vivo specific colonization of the conjugate. (a) Schematic diagram of selective colonization of EcN@TA-PSL at colonic lesion sites. (b) IVIS images of IBD mice at 2, 6, 12, 24, and 48 hours after oral administration of natural EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL. Healthy mice were orally gavaged, with EcN@TA-PSL as control. Each mouse was orally gavaged with 1 × 10^8 viable Dir-labeled natural or coated EcN (ampicillin-resistant) CFU. (c) IVIS images of colons harvested from each group at 6 hours and 48 hours. (d) Representative images of agar plates containing EcN collected from colonic homogenates after 48 hours of oral gavage (n = 3). (e) CLSM images of colonic tissues from each group at 48 hours. Blue: intestinal villus nuclei stained with DAPI, red: Dir-labeled probiotics. Scale bar: 100 μm. White arrows indicate areas of inflammatory infiltration. (f) Total radiative efficiency in the abdominal region of each group at 24 hours and 48 hours (n = 3). (g) Total radiative efficiency in colonic tissues of each group at 6 hours and 48 hours (n = 3). (h) Bacterial counts of EcN in colonic homogenates of each group at 48 hours (n = 3). Data are presented as mean ± standard deviation. Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with DSS disease as control).
3.5 Therapeutic Effects on DSS-Induced UC Mice
To evaluate the therapeutic potential of EcN@TA-PSL in DSS-induced ulcerative colitis (UC) mouse models, we compared it with EcN + tanshinone, EcN@TA, and EcN@TA-PCL. The results showed that EcN@TA-PSL significantly alleviated weight loss and disease activity index (DAI) scores, completely eliminating clinical symptoms (such as bloody stools and diarrhea) at the end of treatment. Additionally, EcN@TA-PSL significantly improved colonic shortening, indicating its effective reduction of inflammation. In contrast, other treatment groups failed to completely alleviate these symptoms, possibly due to low probiotic survival rates, poor drug bioavailability, or lack of ROS-responsive characteristics.
Further analysis revealed that EcN@TA-PSL significantly reduced myeloperoxidase (MPO) activity in colonic tissues, indicating reduced neutrophil infiltration. At the same time, it significantly decreased the levels of pro-inflammatory cytokines (TNF-α, IL-6, and IL-1β) and increased the expression of the anti-inflammatory cytokine IL-10. Histopathological analysis confirmed that EcN@TA-PSL restored epithelial integrity and crypt morphology, significantly reducing inflammatory infiltration. Immunofluorescence staining showed that EcN@TA-PSL significantly enhanced the expression of tight junction proteins (ZO-1 and occludin), indicating its effective repair of the intestinal mucosal barrier.
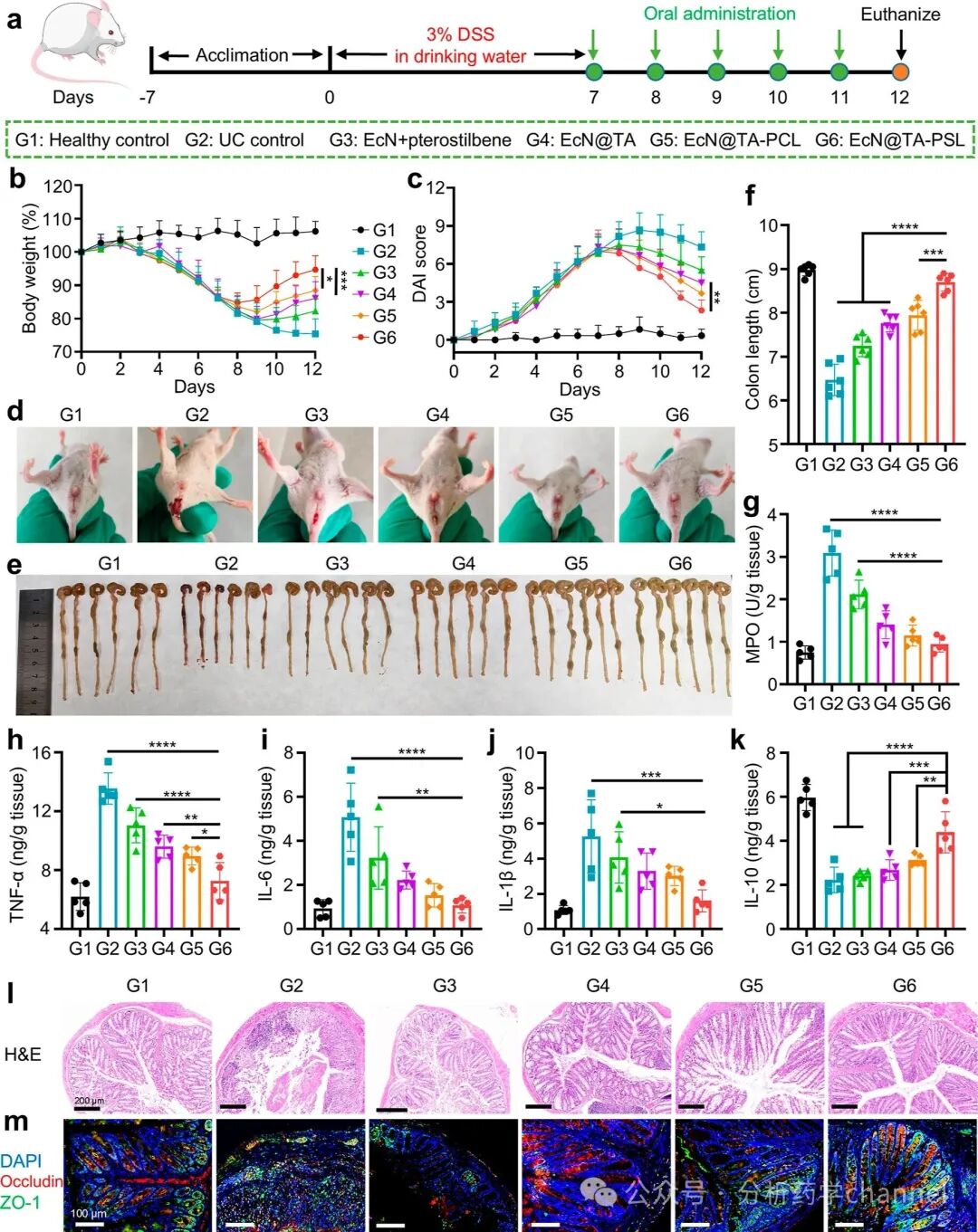
Figure 6. Therapeutic effects of the conjugate on DSS-induced UC mice. (a) Experimental design of DSS-induced UC model mice. After inducing with 3% DSS drinking water for one week, mice were orally gavaged with 2×10^8 CFU EcN + tanshinone, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL daily for 5 days (equal amounts of tanshinone). Mice not treated with DSS were used as healthy controls and given PBS. (b) Photos of rectal bleeding in different groups of mice during treatment. (c) Photos of cecum and colon isolated from different groups of mice (n = 6). (d) Colonic lengths of different groups of mice (n = 6). (e) Daily weight changes of mice in different groups over 12 days; data normalized to the weight percentage of day 0 (n = 6). (f) DAI scores between different groups of mice during treatment (n = 6). (G-K) Quantitative analysis of MPO, TNF-α, IL-6, IL-1β, and IL-10 in colonic tissues of different groups (n = 5). (l) H&E staining of representative colonic tissues from each group. (m) Immunofluorescence staining of ZO-1 (green) and occludin (red) proteins, with cell nuclei stained with DAPI (blue). Data are presented as mean ± standard deviation. Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with DSS disease as control).
To verify the key role of the TA layer, we compared the therapeutic effects of EcN@PSL and EcN@TA-PSL. The results showed that EcN@TA-PSL outperformed EcN@PSL in alleviating weight loss, DAI scores, and colonic shortening, and further inhibited TNF-α while upregulating IL-10. This enhanced efficacy is attributed to the long-term colonic retention of probiotics mediated by the TA layer, emphasizing the importance of intelligent drug release and the synergistic effect with probiotics.
Moreover, 16S rRNA gene sequencing analysis showed that EcN@TA-PSL significantly restored the dysbiosis induced by DSS, increasing the abundance of beneficial bacteria (such as Prevotellaceae, Lachnospiraceae, and Muribaculaceae) and reducing the proportion of pro-inflammatory bacteria (such as Escherichia-Shigella). Principal coordinate analysis (PCoA) and non-metric multidimensional scaling (NMDS) analysis indicated that the microbial composition of the EcN@TA-PSL group was highly similar to that of the healthy control group.
In summary, EcN@TA-PSL effectively treated DSS-induced colitis by alleviating symptoms, reducing inflammation, restoring the intestinal mucosal barrier, and reshaping the dysbiotic microbiota. Its excellent therapeutic effects are attributed to ROS-responsive drug release, TA layer-mediated targeted colonization of probiotics, and the synergistic action of probiotics and drugs, providing an efficient and precise strategy for UC treatment.
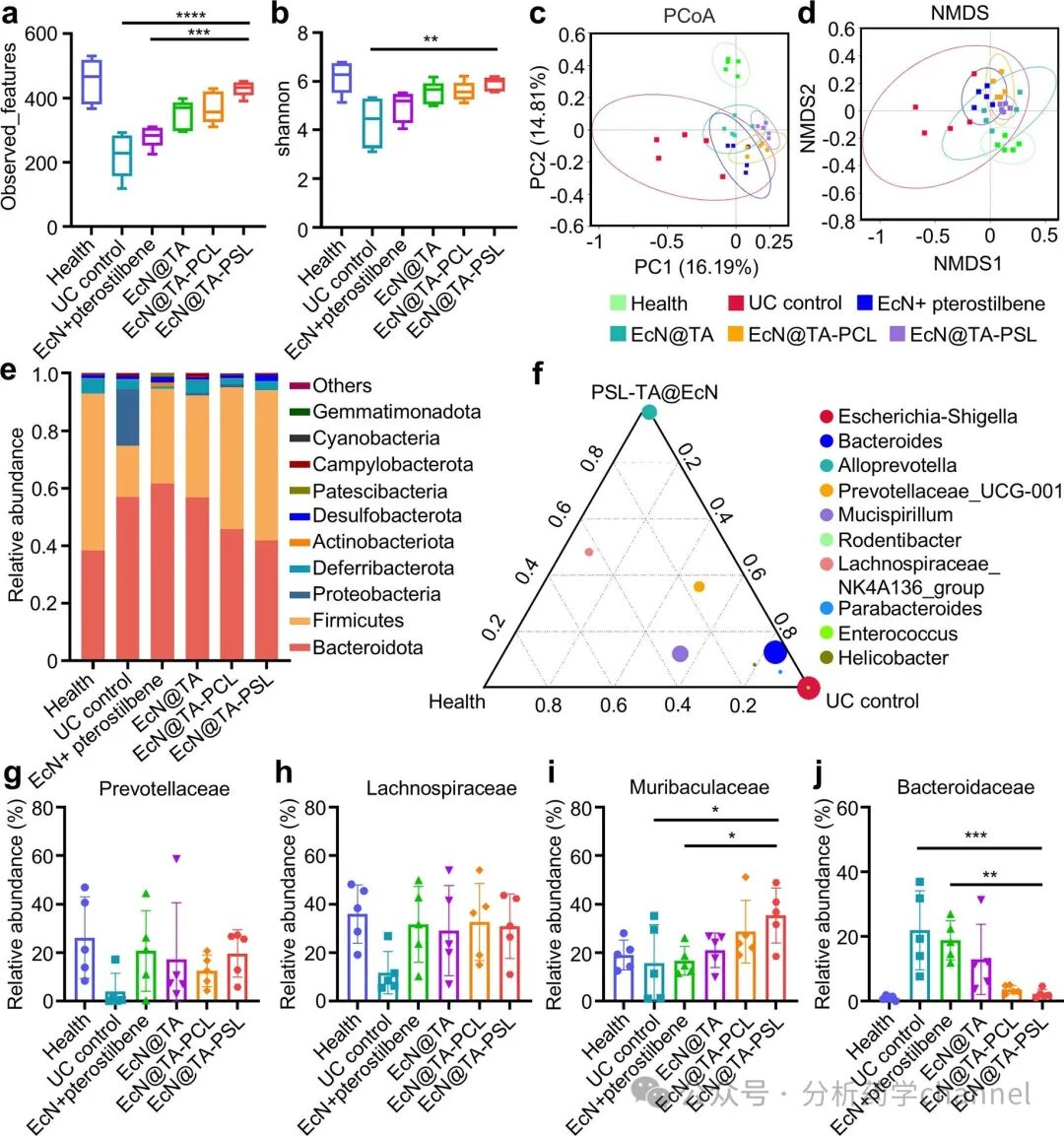
Figure 7. Regulation of the intestinal microbiota by the conjugate in DSS-induced UC mice. α-Diversity of the intestinal microbiota shown by observed features (a) and Shannon index (b). β-Diversity of the intestinal microbiota shown by PCoA (c) and NMDS (d). (e) Relative abundance of the intestinal microbiota at the phylum level. (f) Differences in dominant genera of the intestinal microbiota after EcN@TA-PSL treatment analyzed using ternary plots. (g-j) Relative abundance of selected taxa: Prevotellaceae, Lachnospiraceae, Muribaculaceae, and Bacteroidaceae. Data are presented as mean ± standard deviation (n = 5). Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with DSS disease as control).
3.6 Efficacy in Preventing CAC
To evaluate the potential of the conjugate in preventing and treating colitis-associated colorectal cancer (CAC), we established an AOM/DSS-induced CAC mouse model and compared the therapeutic effects of EcN, EcN@TA, EcN@TA-PCL, and EcN@TA-PSL. The results showed that EcN@TA-PSL significantly alleviated weight loss and disease activity index (DAI) scores, completely reversing clinical symptoms during the third DSS cycle. In contrast, the effects of other treatment groups were weaker, indicating that EcN@TA-PSL has a significant advantage in alleviating CAC progression.
At the experimental endpoint (10 weeks), EcN@TA-PSL treatment significantly improved colonic length and significantly inhibited tumor burden, reducing the average number of tumor nodules per mouse to 1.2±1.2, far lower than the model group’s 7.8±2.4. Additionally, EcN@TA-PSL significantly reduced MPO activity and levels of pro-inflammatory cytokines (TNF-α, IL-6, and IL-1β) in colonic tissues while increasing the expression of the anti-inflammatory cytokine IL-10, indicating its strong anti-inflammatory effects. Histological analysis further confirmed that the EcN@TA-PSL treatment group exhibited optimal recovery of crypt structures, minimal dysplasia, and the least inflammatory cell infiltration, while the model group showed severe pathological changes.
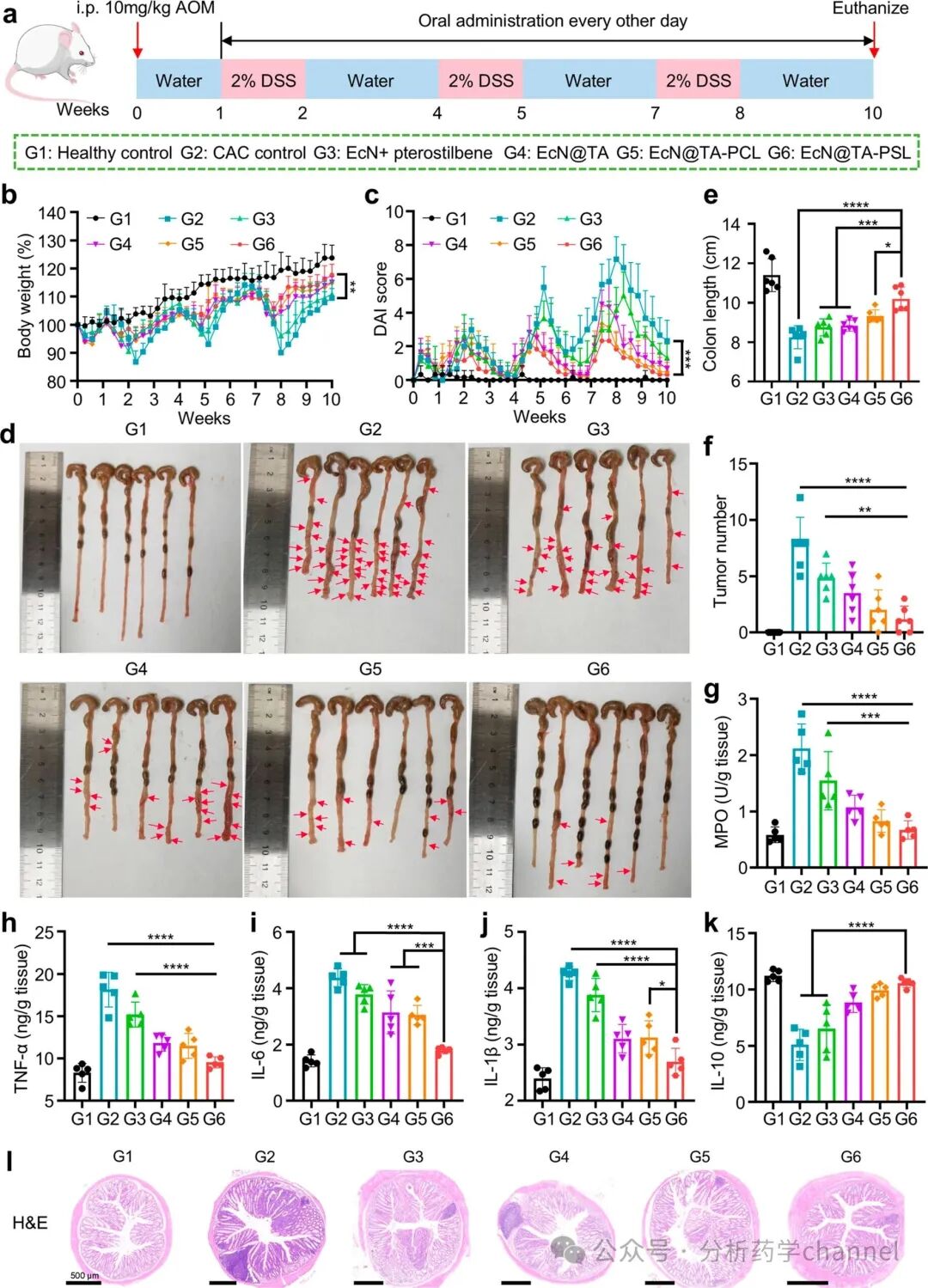
Figure 8. Preventive efficacy of the conjugate against CAC. (a) Experimental design of AOM/DSS-induced CAC model mice. (b) Weight changes of each group of mice during treatment, normalized to the weight percentage of day 0 (n = 6). (c) DAI scores between different groups of mice during treatment (n = 6). (d) Photos of cecum and colon isolated from different groups of mice (n = 6). Red arrows indicate tumors. (e) Colonic lengths of different groups of mice (n = 6). (f) Tumor counts of different groups of mice (n = 6). (G-K) Quantitative analysis of MPO, TNF-α, IL-6, IL-1β, and IL-10 in colonic tissues of different groups (n = 5). (l) H&E staining of representative colonic tissues from each group. Data are presented as mean ± standard deviation. Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with CAC disease as control).
To explore the regulatory effects of the conjugate on the intestinal microbiota, we conducted 16S rRNA gene sequencing analysis. The results showed that EcN@TA-PSL significantly restored the α-diversity indices (observed features, Shannon index, Chao 1 index, and Simpson diversity) in CAC mice and improved β-diversity, making its microbial community structure highly similar to that of the healthy control group. At the phylum level, EcN@TA-PSL significantly increased the relative abundance of Firmicutes, consistent with the results of the DSS-induced colitis model. Heatmap analysis at the family level indicated that EcN@TA-PSL increased the relative abundance of beneficial bacteria (such as Lachnospiraceae, Muribaculaceae, Rikenellaceae, and Oscillospiraceae) while decreasing the abundance of pro-inflammatory bacteria (such as Enterobacteriaceae). Linear discriminant analysis effect size (LEfSe) further identified the significant enrichment of short-chain fatty acid-producing bacteria Roseburia in the EcN@TA-PSL treatment group, suggesting its potential anti-CAC effects through anti-inflammatory and barrier-protective actions.
Furthermore, to assess the biosafety of the orally administered conjugate, we analyzed serum biochemical parameters and conducted histopathological examinations. No significant differences were observed in liver (aspartate aminotransferase, alanine aminotransferase) or kidney (creatinine, urea nitrogen) function markers between treated and control mice. Histological assessments of major organs (heart, liver, spleen, lung, and kidney) through H&E staining revealed no evidence of cellular damage or pathological changes, confirming the safety of the conjugate.
In summary, EcN@TA-PSL effectively prevented and alleviated the progression of CAC by significantly reducing inflammation, inhibiting tumor occurrence, and regulating the intestinal microbiota. Its excellent therapeutic effects are attributed to ROS-responsive drug release, TA layer-mediated targeted colonization of probiotics, and the synergistic action of probiotics and drugs, providing an efficient and precise strategy for CAC treatment.
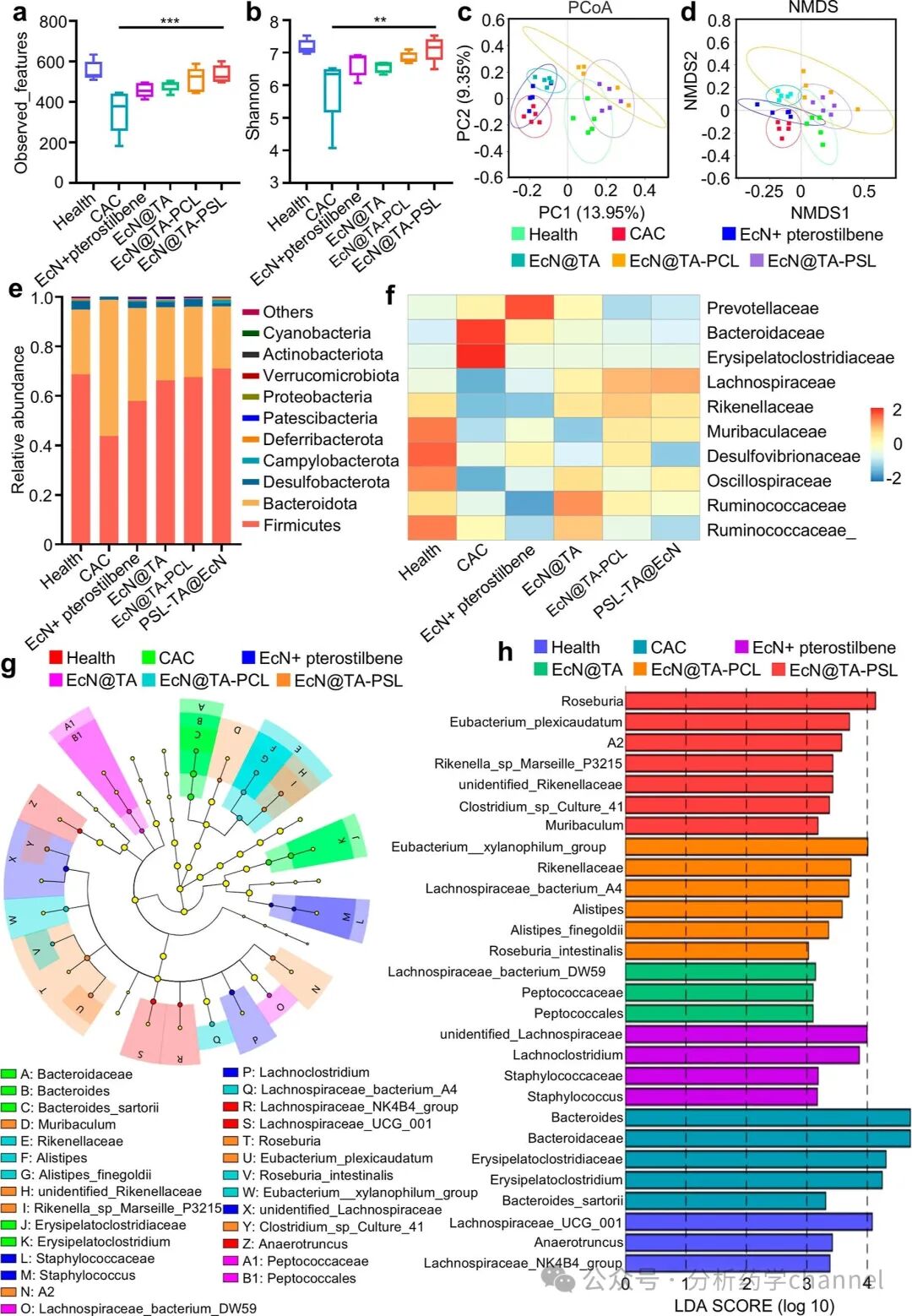
Figure 9. Regulation of the intestinal microbiota by the conjugate in CAC mice. α-Diversity of the intestinal microbiota shown by observed features (a) and Shannon index (b). β-Diversity of the intestinal microbiota shown by PCoA (c) and NMDS (d). (e) Relative abundance of the intestinal microbiota at the phylum level. (f) Heatmap analysis of relative abundance at the family level for each group. (g) Branch diagram based on LEfSe analysis showing the community composition of the intestinal microbiota in each group of mice. (h) Histogram of LDA score distribution for each group. LDA scores greater than 3 indicate that the relative abundance of the corresponding group is higher than that of other groups. Data are presented as mean ± standard deviation (n = 5). Statistical analysis was assessed using one-way ANOVA and Dunnett’s multiple comparison test (EcN@TA-PSL with CAC disease as control).
4. Conclusion
This study developed a triggerable probiotic-drug conjugate (EcN@TA-PSL) aimed at treating ulcerative colitis (UC) and its complications through synergistic probiotic colonization and intelligent drug release. The conjugate effectively protects probiotics from harsh gastrointestinal conditions and exerts therapeutic effects at colonic lesion sites through ROS-responsive drug release and targeted colonization. In mouse models of UC and colitis-associated colorectal cancer (CAC), EcN@TA-PSL demonstrated outstanding therapeutic effects by modulating the inflammatory microenvironment and reshaping the intestinal microbiota, significantly alleviating inflammation, tumor occurrence, and dysbiosis. However, despite achieving significant efficacy in mouse models, translating these findings to clinical applications remains challenging. The human gastrointestinal system is more complex than that of mice, particularly regarding microbial composition and ROS gradients. Therefore, future studies need to further validate these findings in humanized microbiota models. Additionally, achieving consistency in coating thickness and release stability during large-scale production still requires optimization, with strict quality control and quantitative monitoring being key to ensuring therapeutic efficacy.
This study established a novel conjugate system that integrates bio-reactivity, targeted colonization, and synergistic drug therapy by merging materials science and microbiome engineering, opening new avenues for the treatment of gastrointestinal diseases. This innovative strategy not only provides potential therapeutic options for UC and CAC but also offers important references for the precise treatment of other gastrointestinal diseases.

Welcome to follow
Analysis Pharmacy Channel
✦
Note
DOI:
https://doi.org/10.1021/jacs.5c08094
Author: Su
Editor: Xiaobao Liu