
Source: Abdominal Medical Imaging Forum
Cholangiocarcinoma
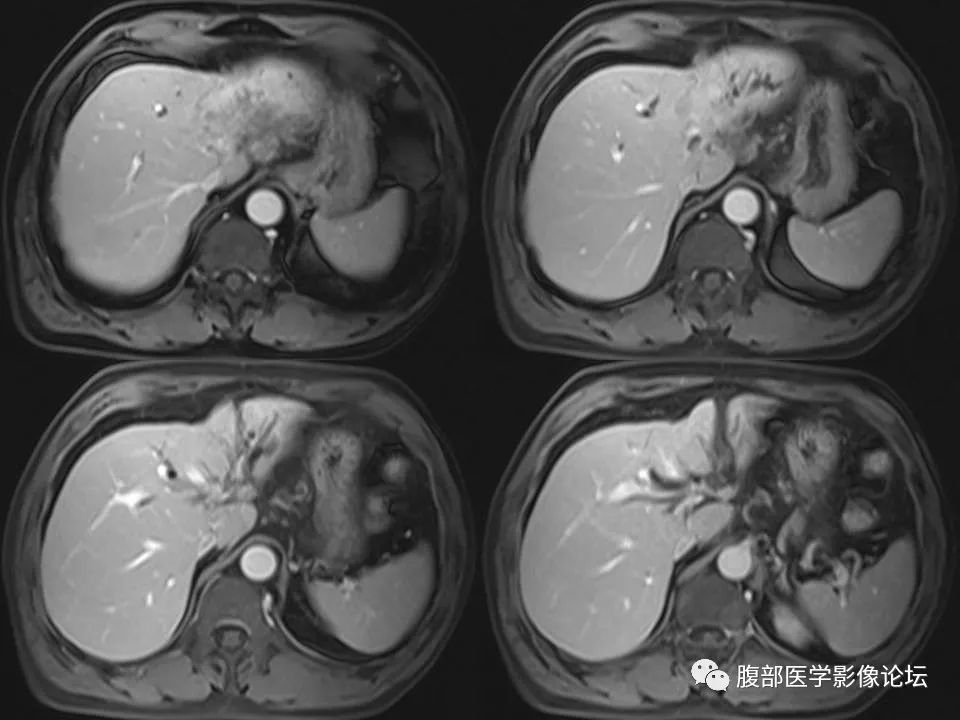
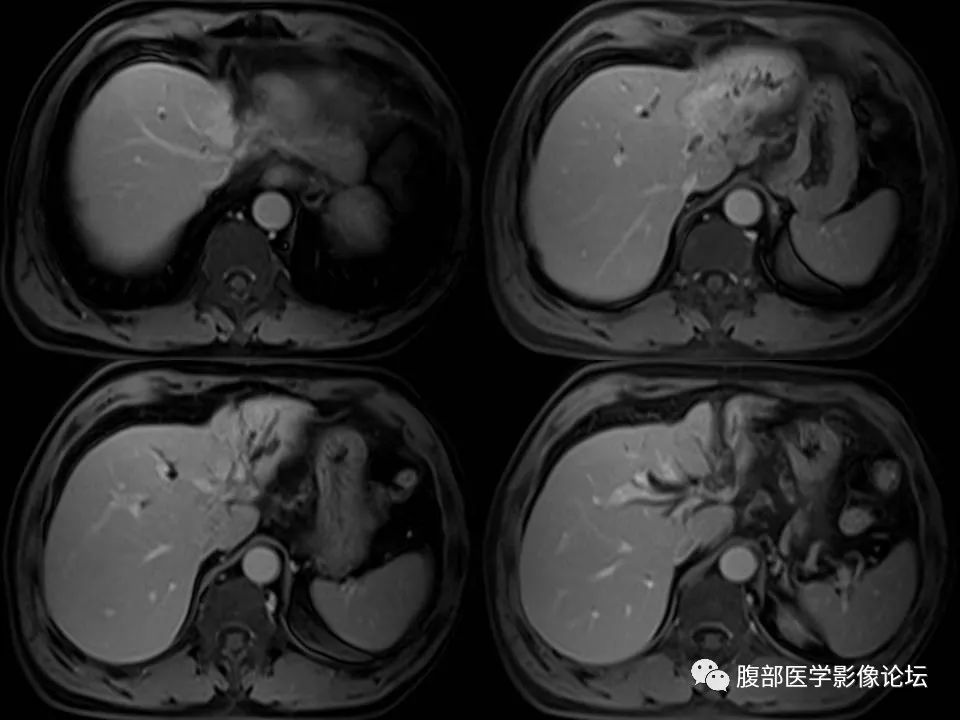
Intrahepatic cholangiocarcinoma (ICC) is a type of malignant tumor composed of cells similar to bile ducts. Intrahepatic (or peripheral) cholangiocarcinoma (ICC) originates from any part of the intrahepatic bile duct epithelium, such as the large intrahepatic bile duct (segmental and regional ducts and their small branches), and the intrahepatic small bile ducts. It refers to adenocarcinoma originating from the epithelium of secondary bile ducts and their branches. ICC accounts for about 10%-15% of primary malignant tumors of the liver, making it the second most common primary liver malignancy after hepatocellular carcinoma, with an increasing incidence in recent years.
Pathology
The gross types of ICC can be classified into three types: mass-forming, periductal infiltrating, and intraductal growth. The most common type is mass-forming, accounting for 60%-80% of ICC; periductal infiltrating type accounts for 15%-35%, which can infiltrate along the bile duct system and portal vein system, leading to bile duct narrowing and surrounding bile duct dilation; intraductal growth type accounts for 8%-29%, often presenting as papillary, polypoid, or granular growths that spread superficially along the bile duct.
Histological Types
The histopathological types of ICC include various types such as adenocarcinoma, adenosquamous carcinoma, squamous cell carcinoma, mucinous carcinoma, and signet-ring cell carcinoma. Most ICCs are adenocarcinomas of varying degrees of differentiation, which can be classified as well, moderately, or poorly differentiated. Those occurring in larger bile ducts may form papillary structures. Tumors often exhibit rich stromal responses, and even local calcification may occur. Most tumors may show varying amounts of mucus. Cancer cells often invade the portal areas, portal area blood vessels, or nerves, which can lead to intrahepatic metastasis via lymphatic drainage pathways or metastasis to local lymph nodes.
Clinical Manifestations
ICC often has no obvious symptoms in the early stages and is frequently discovered incidentally through imaging examinations when liver function abnormalities are detected. Even when the tumor size reaches 5-7 cm, about one-third of patients may have no clinical symptoms. When symptoms do appear, they include abdominal discomfort, vomiting, night sweats, and fatigue. Only about 10%-15% of patients may experience jaundice due to tumor thrombus obstructing the bile duct or metastasizing lymph nodes, or due to the tumor itself compressing the bile duct; fever and elevated white blood cell counts are rare. A mass may occasionally be palpable in the right upper abdomen.
Differential Diagnosis
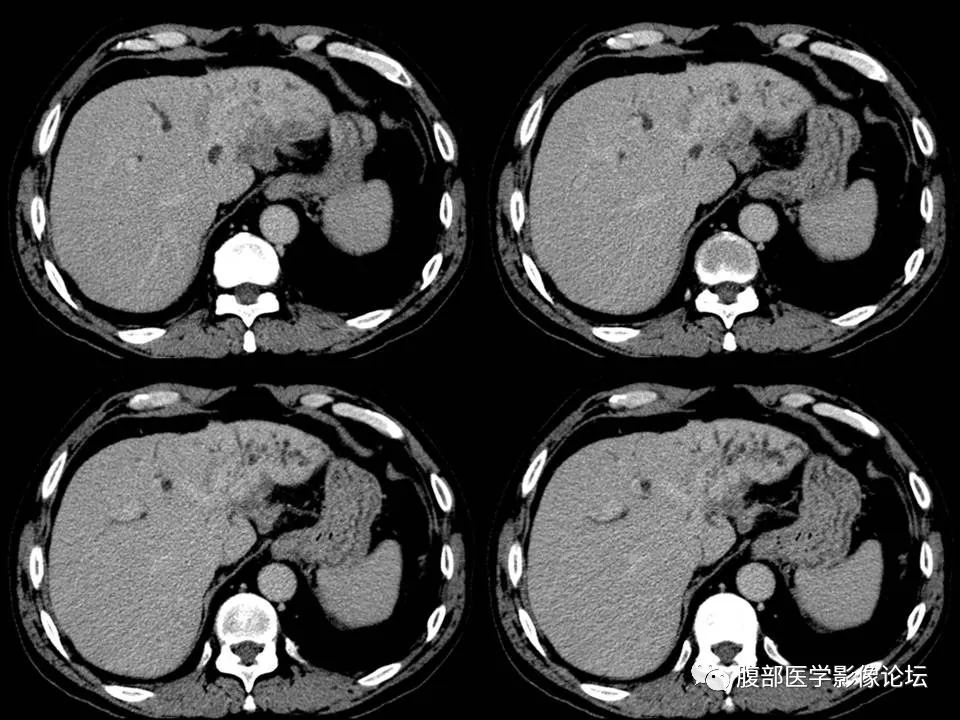
1. Hepatocellular carcinoma: Primary hepatocellular carcinoma is much more common than ICC, with the vast majority of hepatocellular carcinoma cases showing evidence of hepatitis B/C (about 90%) and liver cirrhosis (about 80%), with most having elevated AFP. On CT scans, most lesions appear as low-density with clear boundaries, and calcification within the lesions is extremely rare; enhanced scans, especially spiral CT dual-phase scans, show characteristic findings, with high density in the arterial phase and low density in the portal phase, and the enhancement curve shows a “fast in, fast out” pattern. Additionally, larger hepatocellular carcinomas often have portal vein tumor thrombus formation involving branches and trunks, while ICC usually has no history of hepatitis and cirrhosis, is AFP negative, and lesions are often located in the left lobe of the liver, usually larger with unclear boundaries, and some lesions may show irregular calcification.
2. Liver abscess
Clinically, there are often symptoms and signs of infection; CT may show “cluster signs” or “target signs,” but sometimes differentiation between the two requires ultrasound or CT-guided puncture diagnosis.
3. Metastatic liver tumors
Patients with metastatic tumors often have a history of primary tumors, especially gastrointestinal tumors, and are often multiple. CT shows smooth low-density masses with central low-density necrotic areas, and thickened peripheral enhancement shows a “target sign.” A few liver metastatic cancer lesions may show calcification, characterized by low-density calcification, extensive range, located in the central part of the lesion, with surrounding low-density tumor tissue separated from normal liver tissue, while multiple lesions may show high-density calcifications, forming a significant contrast to ICC’s multiple punctate high-density calcifications.
4. Liver hemangioma
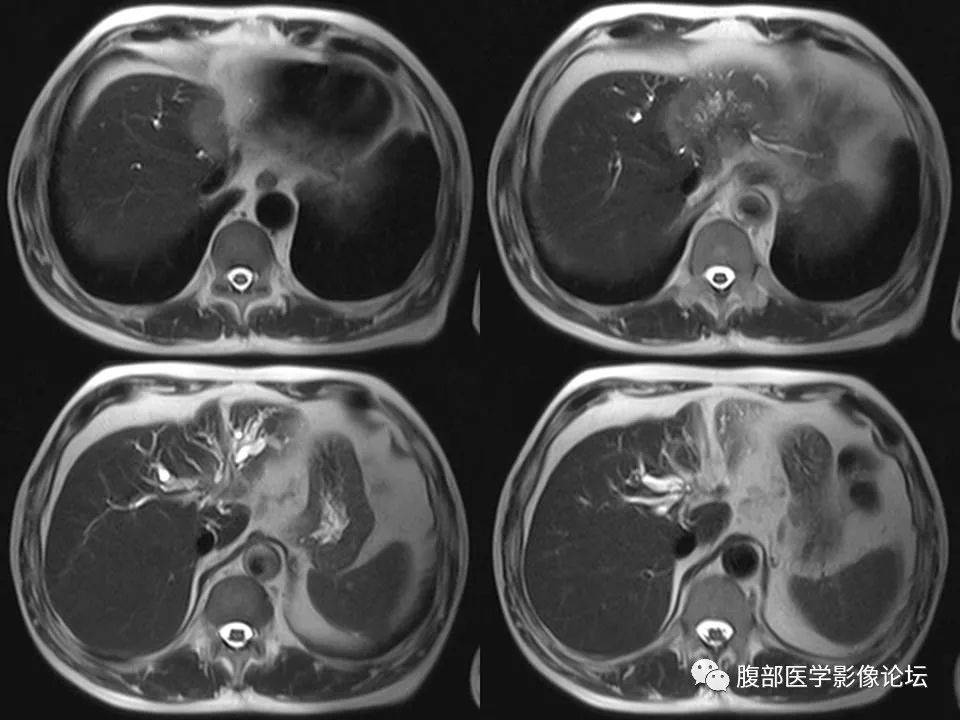
CT scans show well-defined low-density lesions, with enhancement curves showing an “early out, late return” pattern, with typical strip-like or spot-like significant enhancement around the early lesions, with enhancement density roughly equal to that of the abdominal aorta, and delayed scans showing isodense filling. In contrast, ICC shows unclear margins on plain scans, with early enhancement appearing as peripheral ring enhancement, and most lesions often remain unfilled after delayed scans. MR imaging is generally easier to differentiate hemangiomas from ICC compared to CT, as hemangioma lesions show very high signals on T2-weighted images, which can present as the “light bulb sign,” a typical manifestation of hemangiomas. Generally, no enhancement is needed for a clear diagnosis, while ICC rarely shows this imaging feature.
5. Primary sclerosing cholangitis
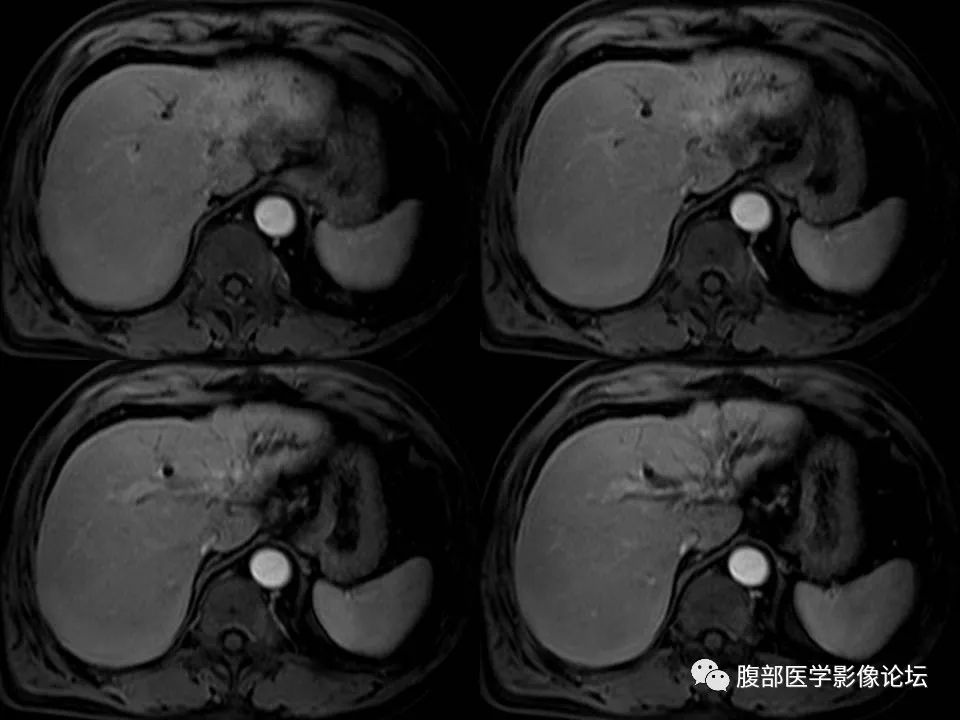
Intrahepatic wall-infiltrating ICC with wall thickening needs to be differentiated from primary sclerosing cholangitis, which shows imaging characteristics of alternating bead-like dilatation and narrowing of the bile ducts, and is often associated with ICC. Dilated bile ducts in the arterial and portal phases may also show peripheral ring enhancement, and delayed scans can differentiate between dilated bile ducts and ICC, with the latter showing delayed enhancement.


Imaging Garden, Editor WeChat: naoyis