Primary liver cancer is a common malignant tumor in China, including hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and mixed hepatocellular carcinoma-cholangiocarcinoma (cHCC-CCA), with HCC accounting for 75% to 85% and ICC for 10% to 15%[1, 2]. Although the incidence of cholangiocarcinoma is low, its malignancy is very high, with most patients diagnosed at an advanced stage and a 5-year survival rate of less than 20%. In recent years, systemic anti-tumor treatment for HCC has transitioned from traditional chemotherapy to targeted and immunotherapy combination treatment. So, as the second most common malignant tumor in the liver, what advancements have been made in systemic anti-tumor treatment for ICC? Can targeted and immunotherapy combination treatments also be used?
First-Line Systemic Treatment
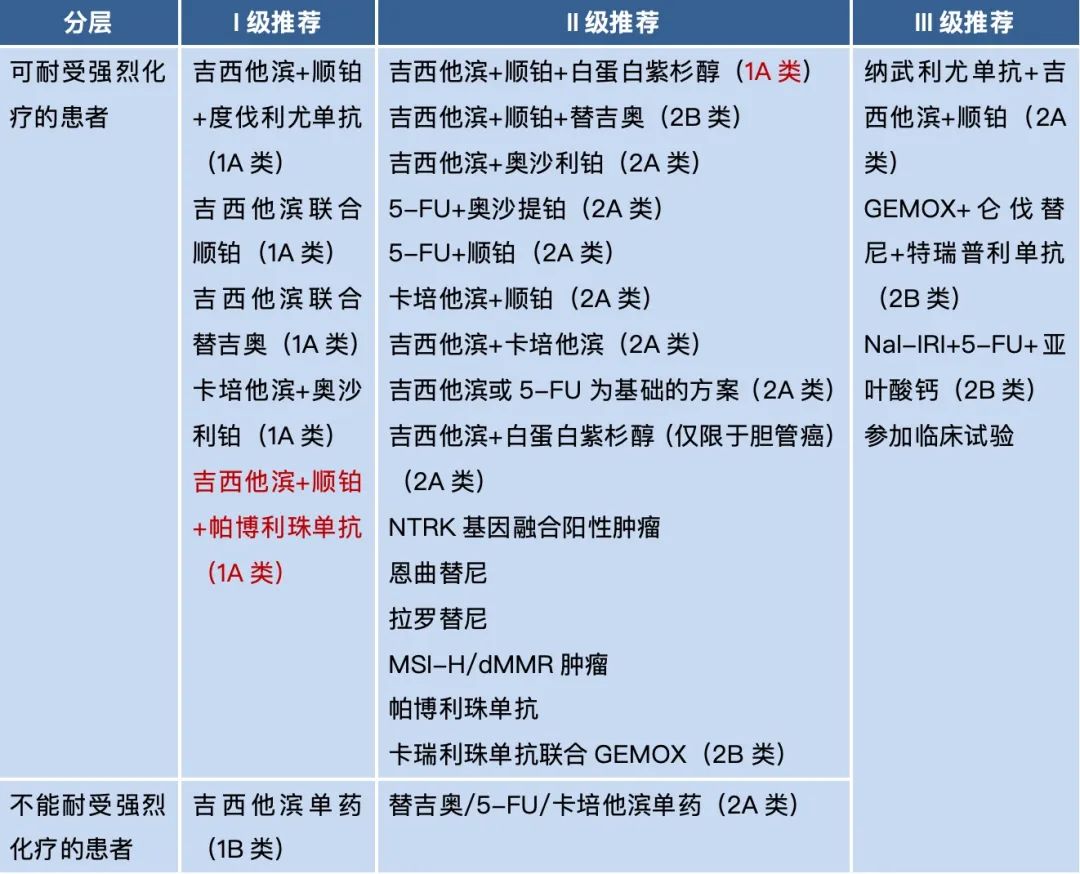
In the past decade, the first-line systemic anti-tumor treatment for ICC has primarily been gemcitabine combined with cisplatin chemotherapy. With the addition of immunotherapy in recent years, immunotherapy combined with chemotherapy has become a guideline-level I recommendation[3], such as durvalumab/pembrolizumab combined with gemcitabine and cisplatin (durvalumab received cholangiocarcinoma indication in China in November 2023). Of course, traditional double-drug chemotherapy remains the cornerstone of first-line treatment for ICC, including gemcitabine combined with cisplatin, gemcitabine combined with tegafur, and capecitabine combined with oxaliplatin.
Regarding first-line immunotherapy and targeted monotherapy, two NTRK inhibitors (entrectinib, larotrectinib) and pembrolizumab have all been early trials without tumor type distinction, and all are post-first-line treatments, but due to favorable clinical data, they are recommended as level II for first-line treatment[3].
Table 1. First-line Treatment for Advanced Biliary Malignancies[3]
Second-Line Systemic Treatment
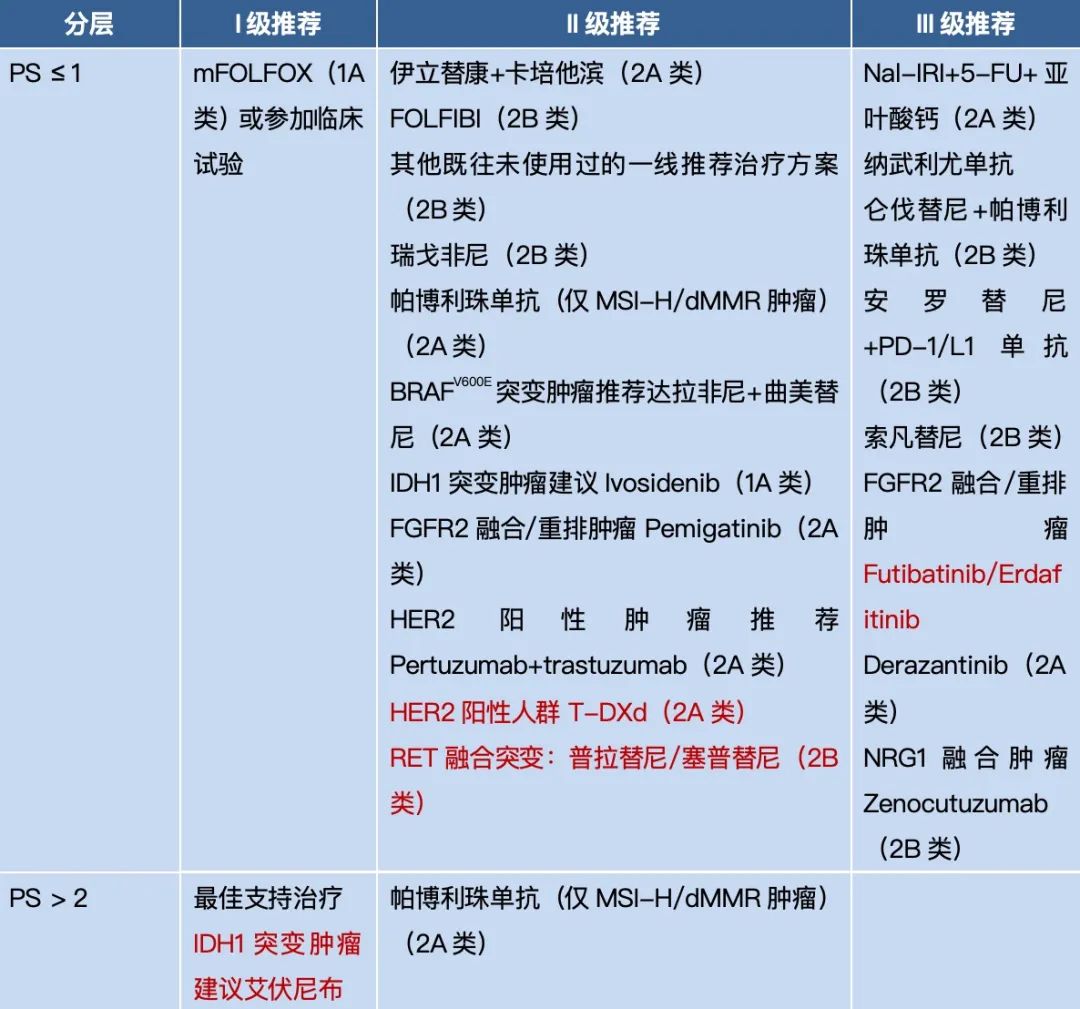
In the second-line and subsequent treatments for ICC, it is recommended to use the mFOLFOX regimen as the second-line treatment plan under active symptom control; other available chemotherapy options include irinotecan combined with capecitabine, irinotecan combined with 5-fluorouracil, etc.[3].
It is important to note that targeted therapy plays a crucial role in second-line treatment for advanced ICC, with common targets including FGFR2 fusions, NTRK fusions, IDH1/2 mutations, BRAF mutations, HER2 overexpression, RET fusions, and NRG1 fusions. For FGFR2 fusion or rearrangement, pemigatinib is recommended; for NTRK fusion-positive patients, entrectinib or larotrectinib is recommended; for IDH1 mutation patients, avapritinib is recommended; for BRAFV600E mutation patients, dabrafenib combined with trametinib is recommended; for HER2 overexpression, options include trastuzumab + pertuzumab or trastuzumab deruxtecan; for RET fusion tumors, pralsetinib/saracatinib is recommended; for NRG1 fusion tumors, zymewisumab is recommended; for ICC patients with unknown driver genes, after systemic chemotherapy, targeted combination immunotherapy, such as pembrolizumab combined with lenvatinib, can be chosen, but the objective response rate (ORR) is only 10%.
Currently, immunotherapy lacks high-quality evidence in second-line treatment for advanced ICC; pembrolizumab is limited to MSI-H/dMMR tumors, and further clinical research is recommended to explore new immunotherapy regimens.
Table 2. Second-Line Treatment for Advanced Biliary Malignancies[3]
Local Combined Systemic Treatment
As most ICC patients are diagnosed at an advanced stage and cannot undergo surgical resection; local treatment has a definite effect in ICC, the most common being liver artery-based local treatments, such as transarterial chemoembolization (TACE), hepatic arterial infusion chemotherapy (HAIC), and Y-90 radioembolization[4]. Ablation therapy can also be used to control local lesions of ICC, including radiofrequency ablation (RFA) and microwave ablation (MWA), especially suitable for tumors <3 cm[5]. Additionally, more studies are exploring the efficacy of durvalumab combined with HAIC and TKIs for advanced ICC patients[6].
ICC has a high degree of malignancy, and treatment is a long way to go. Currently, immunotherapy combined with chemotherapy has become the preferred first-line treatment for advanced ICC, but due to the high heterogeneity of ICC and the complex immune microenvironment, the overall efficacy of targeted combined immunotherapy is limited; in the future, more immunotherapy combinations need to be explored, such as dual immunotherapy combined with TACE/HAIC, etc.
[1] ZHOU M G, WANG H D, ZENG X Y, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 [J]. Lancet, 2019, 394(10204): 1145-1158.
[2] BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries [J]. CA Cancer J Clin, 2018, 68(6): 394-424.
[3] Chinese Society of Clinical Oncology (CSCO). Guidelines for Diagnosis and Treatment of Biliary Malignancies, 2024.
[4] SHEN Y T, ZHU H D, CHEN L, et al. Progress in the Diagnosis and Treatment of Intrahepatic Cholangiocarcinoma [J]. Journal of Interventional Radiology, 2018, 27(03): 285-289.
[5] ZHAO X J, YANG N. Comprehensive Treatment of Intrahepatic Cholangiocarcinoma [J]. Liver, 2023, 28(09): 1020-1023.
[6] Junying Wang, et al. Durvalumab Plus HAIC and TKIs in Combination for Advanced Biliary Tract Cancers. 2024 APASL Abstract Submission No. 200225.
Author: Huang Yuting; Editor: lsh
Cover Image: Image from Tuchong Creative