Intrahepatic cholangiocarcinoma (ICC) is a lethal malignant tumor, with an incidence rate ranking second among primary liver cancers. In the past decade, the incidence of this disease has increased by 140%. ICC accounts for 20% of all liver malignancies, and 3% of all gastrointestinal malignancies.
The disease typically develops against a background of chronic inflammation, which can lead to bile stasis and damage to cholangiocytes.
Identified risk factors for ICC include fibropolycystic liver disease (such as choledochal cysts), primary sclerosing cholangitis, liver stones, cirrhosis, viral hepatitis, parasitic infections (such as Opisthorchis viverrini, Clonorchis sinensis), obesity-related fatty liver disease, diabetes, and exposure to carcinogens (such as nitrosamines, thorium contrast agents, and iron overload) as well as at least four known genetic conditions, including Lynch syndrome, BRCA-associated protein-1 (BAP-1) tumor susceptibility syndrome, cystic fibrosis, and cholangiocarcinoma papillomatosis.
However, no obvious triggering factors are found in most patients diagnosed with cholangiocarcinoma.
The 5-year overall survival (OS) rate for ICC patients is only about 9%, with most patients being in advanced stages at the time of consultation; even when detected early, small tumors may limit the application of diagnostic methods due to their difficult-to-access locations within the liver or due to significant desmoplastic or hypovascular characteristics.
Surgical resection remains the only potentially curative method for ICC, but only 20%-30% of patients have the opportunity for surgical resection, with a postoperative 5-year OS rate of only 20%-35%, and postoperative local and distant recurrence becomes a survival barrier for ICC patients.
Relevant data indicate that postoperative adjuvant therapy with capecitabine yields a median survival of 53 months; in contrast, the median survival for unresectable ICC patients receiving palliative chemotherapy is only 11.7 months.
For advanced patients, the combination of gemcitabine (Gem) and cisplatin (Cis) is considered the most effective first-line regimen.
Recent use of triplet regimens and immunotherapy may change the current treatment landscape.
In terms of targeted therapy, patients with isocitrate dehydrogenase (IDH) and fibroblast growth factor receptor (FGFR) mutations exceeding 40% may receive targeted therapy, but will gradually develop resistance within months, and the survival rate remains low.
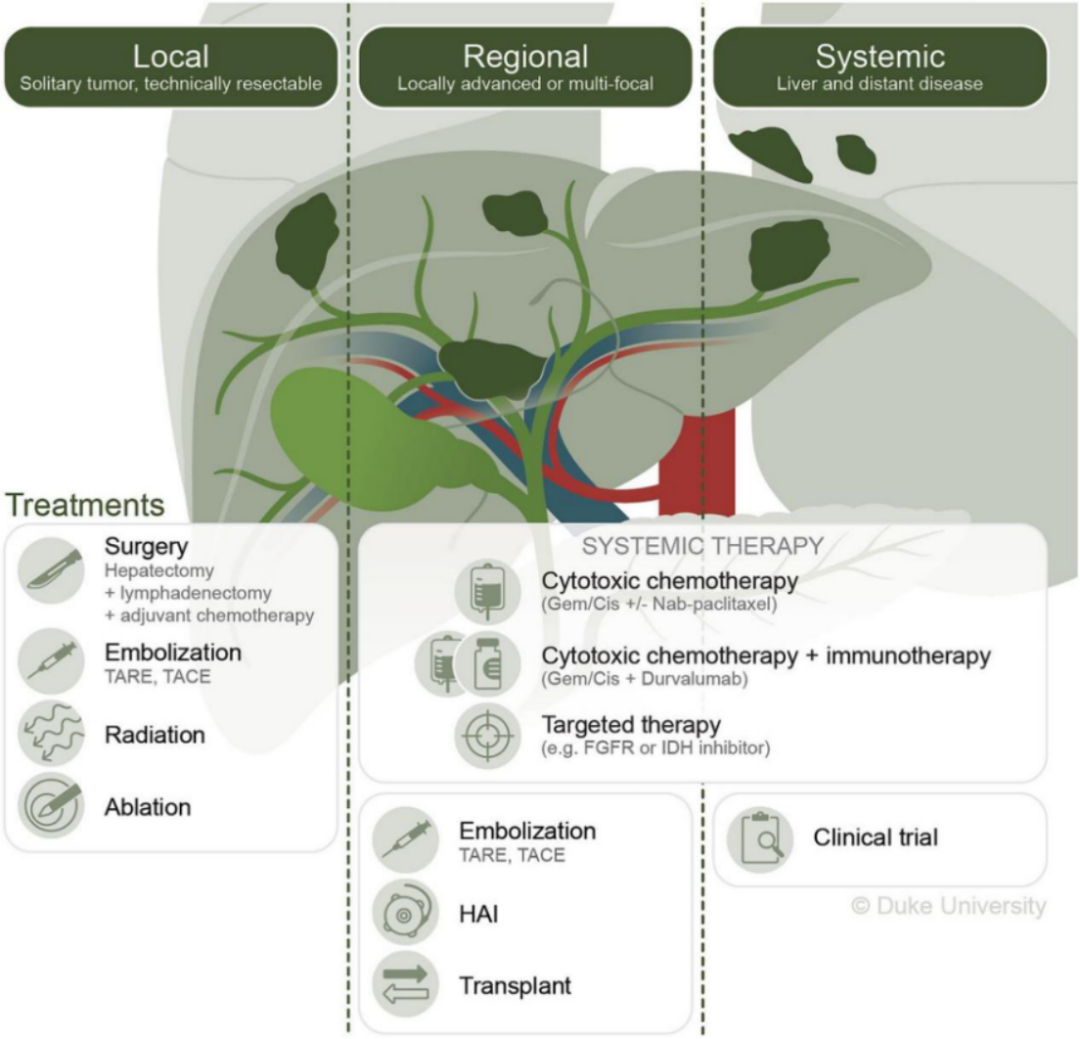
Holster et al. have also developed emerging strategies combining systemic and local treatments, such as transarterial radioembolization or hepatic arterial infusion (HAI) (Figure 1).
This article focuses on current and future treatment strategies for ICC, ultimately guiding personalized and multidisciplinary treatment for ICC patients.
Management of ICC Treatment
The treatment of ICC typically depends on patient-specific and tumor-specific factors, including age, performance status, the underlying health of the patient’s liver, and the extent of the disease (isolated and locally resectable versus locally unresectable and metastatic).
Ideally, treatment decisions should be made by a multidisciplinary expert team, which assesses the patient for surgical resection, perioperative chemotherapy, liver-directed therapies, transplantation, and systemic treatments, including cytotoxic therapy, targeted therapy, and/or immunotherapy.
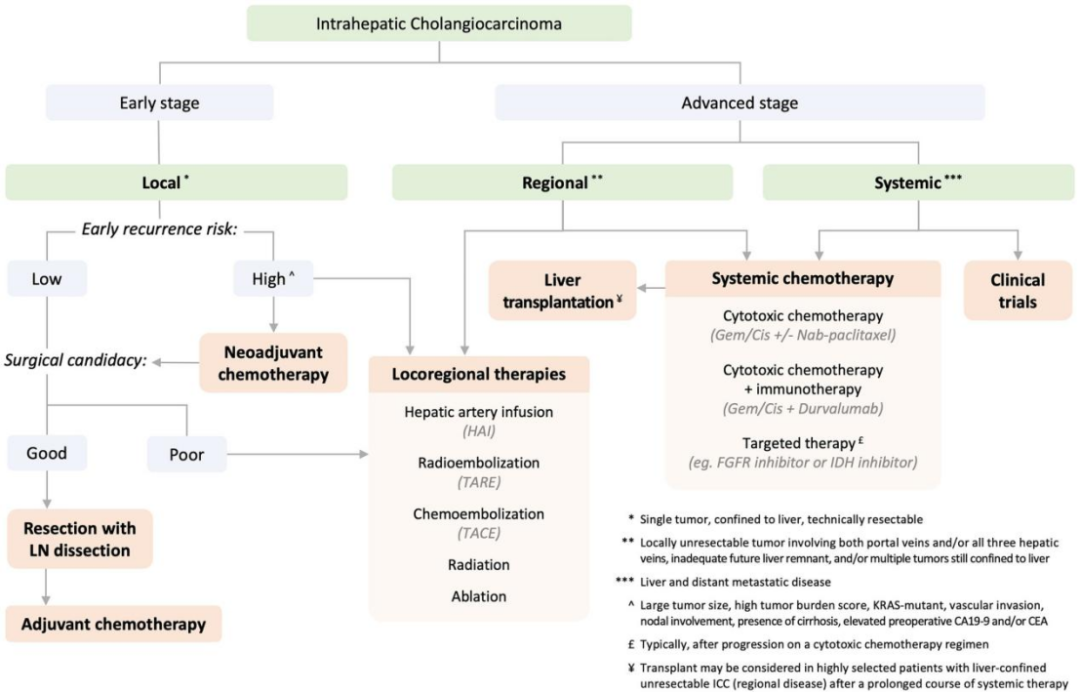
The following sections review the treatment considerations and data for each treatment modality in detail (Figure 2).
The Role of Surgical Resection and Lymph Node Dissection in Early ICC Patients
Surgical resection is the primary treatment for ICC. In a series of studies involving 238 ICC patients, 54% of patients were deemed unresectable at the time of consultation, with the most common reasons being multiple liver lesions (54%), locally unresectable tumors (29%), and distant metastasis (13%).
Among the remaining patients aimed for cure,30% were determined to be unresectable in the operating room, with the most common reasons being detection of multiple liver tumors (33%), lymph node or peritoneal metastasis (64%), or locally advanced disease (12 %).
Of these, 32% ultimately underwent resection, with a median overall survival (mOS) of 36 months, while unresectable patients had a median survival of only 9 months. Resection can yield a median disease-free survival of up to 34 months.
The goal of surgery is to achieve microscopic negative margins (R0), with 76%-92% of patients achieving this. The status of surgical margins correlates with long-term survival in patients and is consistent with resections for other cancers.
In patients with no lymph node metastasis (N0), microscopic positive (R1) resection is an independent predictor of poor survival ([OR] 9.6; 95% [CI], 4.5-20.4).
In lymph node-positive patients, survival after R0 and R1 resections is similar (median survival of 18 months and 13 months, respectively; p=0 .1).
Additionally, median survival correlates with the width of the surgical margin (≤1 mm, 15 months; 2-4 mm, 36 months; 5-9 mm, 57 months; ≥10 mm, 64 months; p <0 .001), and it is proven that margins >5 mm are independent predictors of survival (OR, 2.22; 95% CI, 1.59–3.09).
However, due to local anatomical factors, achieving an ideal wide margin is not always possible. The role of lymph node dissection in reducing local recurrence and improving survival in ICC patients remains controversial.
Although whether lymph nodes are involved is an important prognostic factor, lymph node dissection does not seem to provide therapeutic benefit, especially in patients with major vascular invasion, preoperative CEA levels >5.0 IU/ml, and lymph node metastasis outside the hepatoduodenal ligament.
A multicenter study indicates that lymph node metastasis correlates with poorer outcomes (median survival, N0 is 30 months, N1 is 24 months;p =0 .03 ).
The important role of lymph node dissection is to assist in accurately staging the patient, thereby improving risk stratification for disease recurrence and mortality.
AJCC and NCCN recommend lymph node dissection, including all fibrofatty and lymphatic tissue within the hepatoduodenal ligament between the hepatic hilum and the head of the pancreas, with at least 6 lymph nodes.
During hepatic resection for ICC, relevant procedures are consistent with all patients having biliary malignancies. Lymph node dissection should include group 8 (common hepatic artery) and group 12 (hepatoduodenal ligament) lymph nodes, as approximately 82% of lymph node metastases occur in these locations.
Research shows that only 50% of ICC patients routinely undergo lymph node dissection during hepatic resection. The 5-year OS rate after surgical resection ranges from 11% to 40%, with a 5-year survival rate of up to 63% for lymph node-negative and completely resected (R0) patients, but recurrence still occurs, and the pattern of recurrence is unpredictable.
Intrahepatic recurrence is most common (approximately 60%), especially in patients with lymph node involvement. Recent nomograms from multicenter studies have been used to improve prognostic stratification for ICC patients undergoing resection and may identify which patients are at higher risk of recurrence and may benefit from neoadjuvant and/or adjuvant therapy.
These nomograms combine clinical, pathological, and laboratory data, including tumor size, multifocality, tumor burden score, KRAS status, vascular invasion, lymph node involvement, presence of cirrhosis, and preoperative serum tumor marker levels.
Such nomograms are limited by small sample sizes, institutional practice differences, and selection bias, and they are not routinely used for clinical decision-making in ICC patients.
Adjuvant Chemotherapy After ICC Resection

Research on adjuvant therapy after resection in ICC patients is limited, typically including patients with gallbladder cancer and other biliary cancers.
The PRODIGE 12–ACCORD18 study (ClinicalTrials.gov identifier NCT01313377) is a multicenter, open-label, phase 3 randomized clinical trial involving 196 patients with biliary malignancies treated with R0 or R1 resection from multiple centers in France.
Patients were randomly assigned to receive gemcitabine and oxaliplatin adjuvant chemotherapy (GEMOX) or only monitoring. The median follow-up time for this trial was 46.5 months (95% CI, 42.6-49.3 months), but no statistically significant difference was shown in disease-free survival (median time in the GEMOX group was 30.4 months, while the monitoring group was 18.5 months;
HR, 0.88; 95% CI, 0.62-1.25; p= 0.48) or OS (median, GEMOX group 75.8 months, while monitoring group 50.8 months; HR, 1.08; 95% CI, 0.70-1.66; p= 0.74).
The BILCAP trial (NCT03779035) is a phase 3, randomized, multicenter trial from the UK involving 447 patients with biliary malignancies. In this study, patients were randomly assigned to receive capecitabine or no adjuvant therapy.
The median follow-up time for all patients was 60 months (IQR, 37-60 months). Although intention-to-treat analysis did not show any statistically significant difference, the sensitivity analysis adjusted for various factors (lymph node status, grade, and gender) did lead to an OS HR of 0.71, 95% CI, 0.55-0.92; p=0.01.
In the pre-specified per-protocol analysis (210 patients in the capecitabine group and 220 patients in the observation group), the median OS in the capecitabine group was 53 months (compared to 36 months;
adjusted HR, 0.75; 95% CI, 0.58-0.97; p=0 .028), with a median disease-free survival of 25.9 months (compared to 17.4 months; adjusted HR, 0.70; 95% CI, 0.54-0.92; p= 0.0093).
Bridgewater et al. reported the long-term follow-up of this study in 2022, confirming these results. According to the BILCAP trial, capecitabine adjuvant therapy for 6 months has become the standard treatment for ICC resection patients, regardless of margin or lymph node status.
Further validation of the benefits of adjuvant therapy is ongoing in other clinical trials. The ACTICCA-1 study (NCT02170090) is an international, randomized, phase 3 trial comparing the combination of Gem and Cis with the use of either alone.
The Japanese Clinical Oncology Group JCOG1202 study is an open-label, multicenter, randomized phase 3 trial aimed at confirming the OS extension of S-1 adjuvant chemotherapy in resected biliary cancer patients.
Other adjuvant clinical trials include a phase 3 randomized trial comparing GEMOX with capecitabine in patients undergoing curative resection for ICC and a phase 2 study assessing the safety and efficacy of nab-paclitaxel combined with Gem after ICC resection.
Neoadjuvant Chemotherapy for Resectable ICC Patients
The rationale for neoadjuvant treatment in resectable ICC may include eradicating micrometastatic disease to reduce the risk of early recurrence; improving treatment options by identifying early progressors; and reducing primary tumor size to facilitate achieving R0 resection.
Despite these theoretical benefits, it remains unclear whether patients undergoing surgical resection after neoadjuvant chemotherapy have better survival than those with resectable tumors undergoing upfront surgery.
A retrospective study indicated that in stage I-III ICC patients, neoadjuvant chemotherapy was associated with longer OS compared to adjuvant chemotherapy after upfront resection (40.3 months vs. 32.8 months; p =0 .01).
Another cohort study involving over 4,000 patients showed that after propensity matching, neoadjuvant therapy reduced the risk of death by 23% compared to upfront surgery.
Despite the inherent biases and limitations of retrospective series, these studies suggest a potential advantage of neoadjuvant chemotherapy.
At the 2022 American Society of Clinical Oncology annual meeting, a phase 2 single-arm trial (NEO-GAP; NCT03579771) reported on the efficacy of Gem, Cis, and albumin-bound paclitaxel as neoadjuvant chemotherapy in 30 patients with stage IB-IIIB ICC.
The primary outcome was the completion of all preoperative and surgical treatments and the incidence of adverse events, with results showing: 23 patients (77%) completed all preoperative chemotherapy and underwent radical surgical resection.
Of these, 10 patients (33%) experienced ≥grade 3 treatment-related adverse events, with the most common being neutropenia and diarrhea, and there were no treatment-related deaths. The disease control rate (DCR) was 90% (partial response 23%; stable disease 67%; disease progression 10%).
Other ongoing trials include a single-center phase 2 trial (NCT03603834) aimed at assessing the efficacy of modified FOLFOXIRI (a combination of fluorouracil, leucovorin, irinotecan, and oxaliplatin) for borderline resectable cholangiocarcinoma (ICC/pCC/dCC), evaluated by overall response rate using MRI or CT.
The GAIN trial (NCT03823404) is a multicenter, randomized, controlled, open-label phase 3 study where patients receive perioperative chemotherapy (Gem plus Cis; three cycles preoperatively and postoperatively) or surgery alone.
Subsequently, treatment selected by the surgeon will occur, with the primary endpoint being OS, and secondary endpoints including progression-free survival (PFS), R0 resection rate, toxicity, perioperative morbidity, mortality, and quality of life.
The final trial is the OPT-IC trial (NCT03579771) for FGFR2 fusion intrahepatic cholangiocarcinoma, which will use ctDNA for molecular analysis in resectable ICC patients, followed by one cycle of Gem, Cis, and albumin-bound paclitaxel treatment,
patients with FGFR2 fusion will continue to receive two cycles of FGFR2 inhibitors, followed by surgery and adjuvant therapy, while patients without FGFR2 fusion will receive two additional cycles of chemotherapy, followed by surgery and adjuvant therapy. Feasibility will be the primary outcome of the study, with response and disease-free survival as secondary outcomes.
Local Treatment for Unresectable ICC Limited to the Liver
For advanced, unresectable ICC patients limited to the liver, surgical resection is not feasible due to technical, biological, or patient-specific factors, and various locoregional treatment techniques have been clinically applied, including transarterial chemoembolization (TACE), transarterial radioembolization (TARE), HAI, thermal ablation, and external beam radiotherapy.
Transarterial Embolization Therapy for Unresectable ICC Limited to the Liver
Transarterial embolization therapy is based on the dual blood supply characteristics of the liver to achieve tumor control. Almost all blood supply to liver tumors comes from the hepatic artery system, while the primary blood supply to liver parenchyma comes from the portal vein and hepatic artery system.
Therefore, infusing any particulate matter into the hepatic artery supply of the tumor will lead to significantly higher accumulation within the tumor than in normal parenchyma, thereby optimizing anti-tumor effects and minimizing liver and systemic toxicity.
Transarterial embolization therapy for cholangiocarcinoma includes TACE and TARE. TACE uses a chemotherapy agent combined with an emulsion of ethiodized oil (conventional TACE) or with special particles combined with chemotherapy agents (drug-eluting beads; DEB-TACE).
The choice of chemotherapy used is significantly heterogeneous, with studies reporting the objective response rates (ORR) for TACE with cisplatin, doxorubicin, mitomycin, irinotecan, or combinations of these drugs ranging from 10% to 50%, with median survival times of 12-20 months.
In a recent randomized trial comparing Gem/Cis with Gem/Cis plus DEB-TACE and irinotecan, the combination therapy group showed significantly improved PFS (31.9 vs. 10.1 months) and OS (33.7 vs. 12.6 months), with a significantly higher rate of resection/ablation downstaging in the combination therapy group compared to the chemotherapy alone group (p <0 .005), but with similar adverse event profiles.
Radioembolization requires transarterial delivery of radioactive glass or resin beads combined with Yttrium-90 (Y90). Over the past decade, Y90 has become an increasingly popular locoregional treatment option for unresectable ICC.
Retrospective studies have reported outcomes after a median of 1 to 3 treatments to achieve a cumulative radiation dose exceeding 100 Gray (Gy), with ORR ranging from 6% to 50% and median survival of up to 29 months.
Cucchetti et al. performed a meta-regression analysis of nine observational studies, indicating that TARE is most suitable for ICC patients with mass-forming lesions (compared to infiltrative ICC; median OS, 20 vs. 8 months).
These patients are treatment-naive (compared to those previously treated); median OS was 24 vs. 12 months) and those receiving concurrent systemic therapy (compared to TARE alone; median OS, 20 vs. 6 months).
TARE can promote downstaging to resectability, achieving a 3-year survival rate of 60%; surgical resection typically requires major liver resections and vascular reconstruction, which may be associated with approximately 40% perioperative morbidity and 25% postoperative mortality.
Important predictors of extended survival are performance status, tumor burden, RECIST response, and repeat radioembolization therapy. An increasingly popular method of improving radioembolization treatment is using ultra-high doses limited to small volume liver tumors, known as radiolytic segmentectomy, where high doses of up to 400-800 Gy are delivered to the target tumor.
Many studies have demonstrated the safety of this approach, and across various tumor types, the incidence of complete pathological necrosis increases with the dose.
A recent phase 2 non-randomized study reported the ORR for unresectable ICC patients (NCT 19122053), with 41 patients receiving 1 (65%), 2 (30%), or 3 (5%) Y90 treatments among untreated, unresectable ICC patients greater than 2 cm,
with a median dose of 120 Gy delivered to the target liver, including 317 Gy to the tumor and 87 Gy to surrounding thin-walled tissues; concurrently receiving a median of 6 cycles of Gem and Cis.
Results showed Y90 produced a 39% ORR and 98% DCR at 3 months, with mPFS of 14m and mOS of 12m.
This encouraging result has prompted a randomized study based on Gem chemotherapy ± Y90.
HAI Chemotherapy for ICC
HAI chemotherapy is a treatment strategy that involves surgically implanted subcutaneous pumps delivering high-dose chemotherapy drugs directly to the liver via arterial circulation.
Similar to the principles of TACE and other transarterial therapies, HAI achieves physiological and pharmacological isolation of the liver. Due to the short half-life and high first-pass metabolism of the cornerstone drug fluorodeoxyuridine (FUDR), HAI can achieve drug concentrations in the liver that are 400 times higher than those achievable with systemic administration.
HAI’s role has been well described as a therapy for patients with colorectal cancer liver metastases, which is its most common indication. Recently, emerging data support the role of HAI chemotherapy in advanced, unresectable ICC patients. A multicenter study compared HAI plus FUDR in multifocal ICC patients with OS after resection.
There was no statistically significant difference in median OS between HAI and resection (20.3 months vs. 18.9 months; p =0 .32). The 5-year OS rate for HAI was 12.5% (95% CI, 7.4%-21.1%), while the 5-year OS rate for resection was 20.7% (95% CI, 14.4%-29.7%).
Risk factors for reduced OS in patients treated with HAI or resection for multifocal ICC include tumor diameter (HR, 1.74; 95% CI, 1.20-2.52; p <0.01), number of lesions (HR, 1.84; 95% CI, 1.39-2.44; p <0 .01), and regional lymph node disease (HR, 1.51; 95% CI, 1.17-1.96; p <0 .01).
This data emphasizes the importance of treatment selection for patients and indicates that for multifocal patients, the timing of surgical resection should be strictly evaluated, as the lack of survival advantage may instead increase recurrence rates.
Prospective data evaluating HAI treatment for locally advanced ICC include three phase 2 clinical trials, with reported median OS ranging from 25.0 months to 29.5 months.
Cercek et al. reported a recent phase 2 single-arm study evaluating PFS in unresectable ICC patients receiving HAI and concurrent GEMOX therapy.
The cohort included 38 patients, most of whom were treatment-naive (92%), bilobar (66%), and/or multifocal (55%) tumors, with 47% having positive portal lymph nodes.
Despite these adverse features, HAI treatment still achieved 84% DCR, a partial response rate of 58%, and 4 patients (11%) converted to surgical resection.
The primary endpoint showed a median PFS of 11.8 months, a 6-month PFS rate of 84%, and a median OS of 25 months. These results prompted the initiation of a multicenter, randomized trial (NCT04891289) to evaluate the efficacy of HAI versus concurrent GEMOX in unresectable ICC.
Percutaneous thermal ablation is an established technique for treating primary or secondary liver cancer within certain tumor size and number thresholds.
Ablation methods include radiofrequency ablation (RFA), microwave ablation (MWA), and cryoablation. RFA is the first widely adopted thermal ablation method, while MWA is a newer technology, which is replacing RFA due to significantly shortened ablation times and larger achievable ablation areas.
Generally, ideal candidates for thermal ablation need tumors <3 cm (ideally <3 cm) and located away from critical structures, such as the major portal triad, gallbladder, or intestine; however, techniques such as hydrodynamic dissection can be used to adequately displace the latter to perform ablation safely.
Despite thermal ablation being shown to have high curative potential for various tumors in different organs, literature support for cholangiocarcinoma is relatively poor due to the rarity of small isolated or oligofocal ICC.
A recent systematic review and meta-analysis of 20 studies involving 917 patients treated with RFA or MWA reported that the pooled 1-year OS rate was 82.4%, 3-year OS rate was 42.1%, and 5-year OS rate was 28.5%, with a major complication rate of 5.7%. The pooled local tumor progression rates at 1 year, 3 years, and 5 years were 79.3%, 59.5%, and 58.2%, respectively.
The average tumor size treated in each study was up to 4.4 cm, with tumor size >3 cm associated with shorter OS. More tumor lesions, older age, and the presence of cirrhosis were also associated with shorter survival.
In a study comparing outcomes after resection versus ablation for recurrent ICC, OS and disease-free survival were similar for lesions <3 cm, but major complications significantly increased after repeat liver resection. However, for lesions >3 cm, repeat liver resection can extend OS.
Therefore, the authors recommend thermal ablation for recurrent lesions <3 cm and repeat resection for lesions >3 cm. Compared to surgical resection, thermal ablation has advantages such as lower major complication rates, lower costs, and shorter hospital stays.
Given the high likelihood of other distant intrahepatic metastases occurring, preserving maximal liver parenchyma can provide more treatment options for subsequent lesions, which may have long-term benefits. Notably, similar to resection, due to the infiltrative nature of ICC, it is recommended to at least expand the ablation margin by 1 cm to optimize disease control.
Radiotherapy
Radiotherapy is an option for locally non-metastatic disease, especially for patients unfit for surgical resection or for palliative treatment in metastatic disease patients.
Radiotherapy methods include chemoradiotherapy or ablative radiotherapy (including stereotactic radiotherapy). Ablative radiotherapy delivers high doses of radiation in a limited number of treatments, optimizing target coverage while minimizing doses to surrounding normal tissues and ensuring accurate treatment delivery with imaging guidance during treatment.
A challenge in treating malignant liver tumors is inherent respiratory motion. During radiation simulation, motion is assessed, and if deemed significant, various respiratory management techniques can be employed, such as abdominal compression, gating treatment at phases of the breathing cycle, or breath-hold techniques.
In a series of studies at the University of Texas MD Anderson Cancer Center, 79 patients with unresectable ICC received radical radiotherapy.
The median tumor size was 7.9 cm, with most patients receiving systemic therapy prior to radiotherapy. Radiation doses delivered in 3-30 treatments ranged from 35 to 100 Gy.
Results showed a median OS of 30 months among patients, with overall prognosis highly correlated with radiation dose, with a 3-year OS rate of 73% for patients receiving higher biologically equivalent radiation doses, and no significant treatment-related toxicities were observed in this cohort.
A phase 2 multicenter study assessed the use of proton therapy in 92 patients identified as unresectable HCC or ICC after multidisciplinary review. Patients received an equivalent dose of up to 67.5 Gy, delivered in 15 fractions.
In the ICC cohort, the median tumor size was 6 cm, with 25% having multifocal tumors and 30% having vascular thrombosis. In the ICC cohort, the 2-year local control rate was 94%, and the 2-year OS rate was 47%.
Despite limited data, radiotherapy provides a potential option for achieving local disease control and potential long-term survival, with moderate toxicity. Considering this approach is reasonable for poor or marginal surgical candidates.
ICC Liver Transplantation
With the introduction of liver transplantation (LT) as a treatment option for end-stage liver disease, one of the main indications for LT is unresectable malignant liver and bile duct tumors.
However, early treatment outcomes have been accompanied by high recurrence rates and adverse events. Over the past few decades, as outcomes post-LT have improved, the indications for LT have expanded beyond HCC, particularly in the treatment strategies for optimal candidates with neuroendocrine liver metastases, hilar cholangiocarcinoma, and most recently colorectal liver metastases.
In unresectable ICC patients, LT has traditionally been contraindicated due to poor outcomes. Becker et al. estimated the role of LT in 280 ICC patients, showing a 1-year OS rate of 74% and a 5-year OS rate of 38%, significantly lower than LT outcomes for HCC patients, where the benchmark 5-year survival rate is 75%.
Similar findings were reported by Sapisochin et al., who evaluated 27 ICC patients whose OS at 1 year, 3 years, and 5 years post-LT was worse compared to matched patients receiving LT for HCC (78 %, 66% and 51%, respectively, compared to 100%, 98% and 93%; p <0.001).
Patients with multifocal or solitary tumors >2 cm had worse OS than ICC patients with smaller tumors (1 year, 3 years, and 5 years were 80%, 66%, and 61%, respectively).
Although outcomes after LT for ICC have historically been unacceptable, recent studies challenge this premise: LT combined with neoadjuvant chemotherapy has achieved relatively satisfactory transplant outcomes in carefully evaluated ICC patients.
Renshaw et al. reported on 12 unresectable ICC patients who achieved positive outcomes after at least 6 months of Gem-based chemotherapy followed by LT and radiotherapy or stable disease.
The study achieved positive results, with 1-year OS of 100% (95% CI, 100%–100%), 3-year OS of 83.3% (95% CI, 27.3%–97.5%), and 5-year OS of 83.3% (95% CI, 27.3%–97.5%), with a 5-year disease-free survival rate of 50% (95% CI, 11.1%–80.4%).
When considering LT, patient selection remains crucial: early (solitary tumors <2 cm) ICC patients undergoing LT have a 1-year, 3-year, and 5-year survival rate of 93%, 84%, and 65%, respectively, compared to late-stage (multinodular or solitary tumors >2 cm) ICC patients with 79%, 50%, and 45%, respectively (p=0 .02).
In another study, McMillan et al. found that in locally advanced, unresectable ICC patients who received neoadjuvant chemotherapy and demonstrated stable disease for 6 months without extrahepatic disease, patients undergoing LT had 1-year, 3-year, and 5-year overall survival rates of 100%, 71%, and 57%, respectively.
Since these results come from retrospective analyses and/or single-center, non-randomized studies, LT is not currently recommended as the standard treatment for ICC. Currently, multiple clinical trials are underway to determine the benefits of LT for this population and identify which patients may be ideal candidates for LT.
Systemic Treatment for Advanced ICC Patients
Systemic chemotherapy is a key strategy for treating 70%-80% of unresectable and metastatic ICC patients. According to the results of the ABC-02 trial reported in 2010 (NCT01926236), the combination of Gem and Cis is the preferred first-line therapy.
In phase 3 of the trial, OS and PFS were compared between Gem/Cis and Gem alone, with the combination therapy group showing better benefits: OS and PFS were 11.7m vs 8.1m and 8m vs 5m, with DCR being 81% vs 72%.
Outside the US, phase 3 data supports an alternative strategy of Gem plus S-1 (Gem/S-1), with efficacy comparable to Gem/Cis (median OS, Gem/Cis 13.4 months, Gem/S-1 15.1 months; HR, 0.945; 90% CI, 0.78-1.15; p = 0.046; median PFS of 5.8 months vs 6.8 months, HR, 0.86; 95% CI, 0.70-1.07).
Published triplet regimens have shown mixed results in locally advanced unresectable or metastatic biliary cancers (including ICC).
In the PRODIGE 38 AMEBICA trial (NCT02591030), the combination of oxaliplatin, irinotecan, and infusional fluorouracil (mFOLFIRINOX) was not as effective as Gem/Cis in first-line therapy.
In this randomized phase 2/3 trial, the 6-month PFS (mFOLFIRINOX group 44.6%, Gem/Cis group 47.3%), median PFS (6.2 months and 7.4 months, respectively), and median OS (11.7 months and 13.8 months, respectively) were superior in the Gem/Cis group.
Recently, results have also been reported from a single-arm phase 2 trial adding albumin-bound paclitaxel to Gem/Cis in first-line therapy:
The median PFS for Gem/Cis/Nab-paclitaxel was 11.8 months, with a median OS of 19.2 months, observing an ORR of 15 (44%) among 38 ICC patients, with 14 (41%) patients having SD, and 8 (21%) of unresectable ICC patients ultimately undergoing resection, indicating that this regimen may have potential to downstage disease to facilitate curative surgery.
Compared to historical experiences with dual regimens, these improved results have prompted a randomized trial (NCT03768414) to validate the benefits of adding albumin-bound paclitaxel to Gem/Cis.
Targeted Therapy and Immunotherapy in ICC
Large-scale tumor sequencing efforts have identified numerous genomic alterations present in ICC, although only a few commercially approved therapies such as FGFR2 and IDH1 inhibitors exist, research targeting other targets (such as BRAF, HER2, and IDH2) is still ongoing.
FGFR2 fusions are detected in 10%-15% of ICC and tend to occur in younger patients, with IDH1 mutations found in 25% of ICC patients.
Abou-Alfa et al. reported the results of a phase 2 non-randomized study evaluating pemigatinib in 146 patients with unresectable or metastatic cholangiocarcinoma progressing after Gem-based chemotherapy.
The primary endpoint of the study was ORR in FGFR2 fusion/rearrangement positive patients, with secondary endpoints including ORR in patients with other FGFR2 alterations, DCR, PFS, OS, safety, and pharmacokinetics.
Compared to FGFR2 wild-type ICC patients, patients with FGFR2 fusion/rearrangement showed significantly improved clinical activity with pemigatinib (complete response, 3% vs 0%; partial response, 33% vs 0%; stable disease, 47% vs 40%; disease progression, 15% vs 35%), with a median PFS of 6.9 months and median OS of 21.1 months.
Javle et al. evaluated BGJ398 (infigratinib) in FGFR2 fusion-positive ICC patients after progression following Gem chemotherapy.
This phase 2 non-randomized study included 61 patients, with the primary endpoint being ORR, and secondary endpoints including PFS, DCR, and adverse events. The median PFS was 5.8 months, with an ORR of 15% and a DCR of 75%.
For patients with IDH1 mutations, a phase 1 study evaluated ivosidenib monotherapy in 73 patients with IDH1 mutant cholangiocarcinoma.
The median PFS was 3.8 months (95% CI, 3.6-7.3 months), with a 6-month PFS rate of 40.1% (95% CI, 28.4%-51.6%), and a 12-month PFS rate of 21.8% (95% CI, 12.3%-33.0%), with a median OS of 13.8 months (95% CI, 11.1-29.3 months).
Based on this efficacy, Abou-Alfa et al. recently reported the results of the ClarIDHy phase 3 global double-blind randomized trial (NCT02989857) comparing ivosidenib with placebo in 185 IDH1 patients.
Compared to placebo, ivosidenib significantly improved PFS (2.7 months [95% CI, 1.6-4.2 months] vs. 1.4 months [95% CI, 1.4-1.6 months]; HR 0.37; 95% CI, 0.25-0.54; one-sided p< 0.0001);
However, in the intention-to-treat population, OS was numerically improved but did not show statistical significance (median OS, 10.3 months [95% CI, 7.8-12.4 months] vs. placebo group 7.5 months [95% CI, 4.8-11.1 months]; HR, 0.79 [95% CI, 0.56-1.12]; one-sided p =0.09).
This result is thought to be caused by a 57% crossover rate; after crossover adjustment, the median OS for the placebo group was 5.1 months (95% CI, 3.8-7.6 months; HR, 0.49 [95% CI, 0.34-0.70]; one-sided p <0 .001).
Furthermore, the tolerability of ivosidenib is good, with only 2% of serious adverse events considered related to ivosidenib, and no treatment-related deaths. There was no decline in quality of life in the ivosidenib treatment group compared to the placebo group.
Recently, immune checkpoint inhibitors have played a role in the treatment of ICC. Prior studies of single-agent or dual-agent immune checkpoint blockade in refractory disease have shown responses in 10%-20% of patients, but the results have not gained regulatory approval;
The TOPAZ-1 trial (NCT03875235) has reignited researcher enthusiasm, being a phase 3, randomized, double-blind, placebo-controlled study comparing Gem/Cis plus durvalumab with Gem/Cis plus placebo.
The median OS in the durvalumab group was 12.8 months, while Gem/Cis was 11.5 months (HR, 0.80; 95% CI, 0.66-0.97; p= 0.021), with a median PFS of 7.2 months, while Gem/Cis was 5.7 months (HR, 0.75; 95% CI, 0.64-0.89; p= 0.001), with an ORR of 26.7%, while Gem/Cis was 18.7%.
Although the absolute differences in these survival endpoints (especially OS) are very small, the tail data on the survival curves is encouraging, with up to 25% of patients alive at 2 years, and possibly seeing unprecedented durable responses to cytotoxic therapies.
Other unresolved issues include whether this treatment strategy has efficacy differences among patients in different regions of the world. Pre-specified efficacy subgroup analyses conducted on patients enrolled in different regions show that the OS HR is numerically lower in Asia, but the study results still indicate that, regardless of geographic location, the trend of OS benefit tends to favor combination with durvalumab.
Conclusion
ICC is a rare and aggressive lethal malignancy with an increasing incidence rate year by year. Although ICC has been managed through surgical resection and cytotoxic therapies for locally advanced or metastatic disease, recent multimodal treatment approaches have shown trends toward improving patient survival.
This article comprehensively reviews various modern multimodal therapies that improve the prognosis of ICC patients. For locally resectable ICC patients, R0 resection of the liver with negative margins and adjuvant therapy with capecitabine should be considered standard treatment;
for patients with unresectable or metastatic ICC, locoregional treatments, triplet systemic regimens, and targeted immunotherapies are now increasingly utilized by clinicians, achieving encouraging results in optimally selected patients.
Despite current literature supporting multimodal treatment approaches and these alternative therapeutic options, future efforts remain crucial, and developing more effective treatments to further improve the prognosis of ICC patients is still the direction of ongoing endeavors.
Moris Dimitrios, Palta Manisha, Kim Charles et al. Advances in the treatment of intrahepatic cholangiocarcinoma: An overview of the current and future therapeutic landscape for clinicians.[J]. CA Cancer J Clin, 2023, 73: 198-222.
Source | VIP Talk
Editor | Joy
(Copyright belongs to the original author, if there is infringement, please contact the editor for deletion)