Pathological Diagnosis of Liver Cancer
Primary liver cancer refers to malignant tumors originating from hepatocytes and intrahepatic bile duct epithelial cells, mainly including HCC, ICC, and cHCC-CCA.
HCC: refers to malignant tumors arising from hepatocytes. The pathological diagnostic terms “hepatocellular carcinoma” or “hepatocellular type liver cancer” are not recommended.
ICC: refers to malignant tumors arising from the epithelial cells lining the branches of intrahepatic bile ducts, with adenocarcinoma being the most common. Histologically, it can be divided into:
① Large duct type: originating from larger bile ducts above the portal areas between the liver lobules, with large and irregular glandular duct diameters;
② Small duct type: originating from small bile ducts or fine bile ducts below the bile duct septum of liver lobules, with small and relatively regular glandular duct diameters, or appearing as solid thin strands with closed lumens. Studies have shown that the biological behavior and genetic phenotypic characteristics of these two subtypes of ICC are also different, with patients of the small duct type having better clinical prognosis than those of the large duct type.
Regarding the clinical and pathological significance of molecular typing of HCC and ICC, many aspects are still under research and validation. However, recent studies have shown that EB virus-related ICC has unique clinical pathological, immune microenvironment, and molecular characteristics, with better prognosis and significant benefits from immune checkpoint therapy, which may become a new subtype. Moreover, the high expression of phosphofructokinase 1 in ICC tissues is a useful indicator for assessing postoperative recurrence risk. The 2019 edition of the “WHO Classification of Digestive System Tumors” no longer recommends using the pathological diagnostic terms “cholangiocellular carcinoma” and “cholangiolocellular carcinoma” for ICC. The gross sampling and microscopic examination requirements for ICC mainly refer to those for HCC.
cHCC-CCA: refers to the simultaneous presence of HCC and ICC tissue components within the same tumor nodule, excluding collision tumors. Although some scholars suggest using a pathological diagnostic standard of ≥30% for both tumor components as a criterion for cHCC-CCA, there is currently no internationally unified pathological diagnostic standard for the proportion of HCC and ICC components in cHCC-CCA. Therefore, it is recommended to annotate the proportion of the two tumor components during the pathological diagnosis of cHCC-CCA to assist clinical evaluation of tumor biological characteristics and treatment plan formulation.
Standards for Pathological Diagnosis of Liver Cancer
The standards for pathological diagnosis of liver cancer consist of specimen handling, sampling, pathological examination, and pathological report.
Key points for specimen handling:
① The operating physician should clearly indicate the site, type, and quantity of the specimens on the pathological examination request form. The surgical margins and significant lesions can be marked with dye or sutures;
② The tumor specimens should be sent to the pathology department for cutting and fixation within 30 minutes of removal. Specimen collection for tissue banks should be conducted under the guidance of the pathology department to ensure sampling accuracy and should primarily meet the needs of pathological diagnosis;
③ Fixation with 4% neutral formaldehyde (10% neutral buffered formalin) solution for 12-24 hours.
Key points for sampling: The peripheral area of liver cancer is representative of the tumor’s biological behavior. Therefore, a 7-point baseline sampling method is required (Figure 1), sampling at the 12 o’clock, 3 o’clock, 6 o’clock, and 9 o’clock positions at the interface between the cancer and the surrounding liver tissue at a 1:1 ratio; at least one piece should be sampled from within the tumor; and one piece each should be sampled from liver tissue within ≤1cm (near cancer) and >1cm (far cancer) from the tumor margin. For small liver cancers with a maximum diameter of ≤3cm, all should be sampled for examination. The actual sampling sites and quantity should also consider the tumor’s diameter and number (Evidence Level 2, Recommendation A).
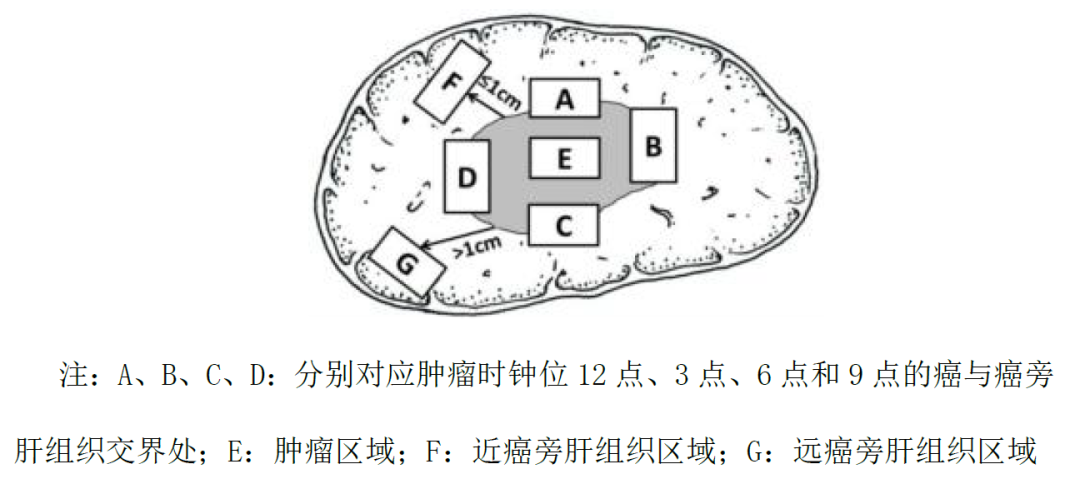
Figure 1 Diagram of baseline sampling sites for liver tumor specimens
Key Points for Pathological Examination of Liver Cancer
Gross specimen observation and description: A comprehensive observation of all surgical specimens submitted for examination should be conducted, with a focus on describing the tumor’s size, number, color, texture, relationship with blood vessels and bile ducts, capsule status, surrounding liver tissue lesions, type of liver cirrhosis, distance from the tumor to the margin, and margin status.
Microscopic observation and description: A comprehensive observation of all sampled tissues should be performed, with the pathological diagnosis of liver cancer referring to the 2019 edition of the “WHO Classification of Digestive System Tumors,” focusing on the following content. The degree of differentiation of liver cancer can be assessed using the internationally used Edmondson-Steiner grading system (I-IV) or the WHO recommended high, medium, and low differentiation.
The histological morphology of liver cancer: Common types include trabecular, pseudoglandular, and solid types; special subtypes of liver cancer include fibrolamellar, sclerosing, clear cell, fatty, giant cell, chromophobe, neutrophilic, lymphocytic, and undifferentiated types; the extent and degree of tumor necrosis (e.g., after transarterial chemoembolization treatment), lymphocyte infiltration, and stromal fibrosis; the growth pattern of liver cancer: including peritumoral infiltration, capsule invasion or breakthrough, microvascular invasion (MVI), and satellite nodules; assessment of chronic liver disease: liver cancer often accompanies varying degrees of chronic viral hepatitis or liver cirrhosis, and the simpler Scheuer scoring system and the Chinese histological grading and staging criteria for chronic viral hepatitis are recommended.
MVI diagnosis: MVI refers to the presence of cancer cell nests in the vascular lumen lined by endothelial cells under the microscope. Liver cancer most commonly invades the branches of the portal vein (including intraparenchymal vessels), and lymphatic invasion may occur in ICC. The pathological grading method is as follows: M0: no MVI detected; M1 (low-risk group): ≤5 MVI, all occurring in the peritumoral liver tissue (≤1cm); M2 (high-risk group): >5 MVI, or MVI occurring in distant peritumoral liver tissue (>1 cm). MVI and satellite lesions can be considered different stages of intrahepatic metastasis of liver cancer. When it is difficult to distinguish between satellite nodules or lesions in the peritumoral liver tissue and MVI, they can be collectively counted in the MVI pathological grading. MVI is an important reference for assessing the recurrence risk of liver cancer and selecting treatment options, and should be included as an indicator in routine histopathological examinations (Evidence Level 2, Recommendation A).
Immunohistochemical Examination
The main purposes of immunohistochemical examination for liver cancer are:
① Differentiation between benign and malignant liver cell tumors;
② Differentiation between HCC and ICC as well as other special types of liver tumors;
③ Differentiation between primary liver cancer and metastatic liver cancer. Due to the high heterogeneity of histological types of liver cancer, existing liver cancer cell protein markers have certain limitations in diagnostic specificity and sensitivity, often requiring rational combinations and objective assessments, and sometimes needing to be used in conjunction with markers from other systemic tumors.
HCC:
The following markers are positive for liver cell labeling and can help suggest tumors of hepatocyte origin, but cannot be used as a basis for distinguishing between benign and malignant liver cell tumors.
① Arginase-1: positive staining in the cytoplasm/nucleus of hepatocytes.
② Hepatocyte antigen: positive staining in the cytoplasm of hepatocytes.
③ Specific antibodies for liver cell membrane bile duct: such as CD10, polyclonal carcinoembryonic antigen, and bile salt export pump protein, etc., can show specific staining on the bile duct surface of liver cell membranes, which helps confirm hepatocyte tumors.
The following markers are helpful for distinguishing benign and malignant liver cell tumors.
① Phosphatidylinositol protein-3: positive staining in the cytoplasm and cell membrane of hepatocellular carcinoma.
② CD34: Although CD34 immunohistochemical staining does not directly label liver parenchymal cells, it can show the microvascular density and distribution patterns of different types of liver tumors: hepatocellular carcinoma shows a diffuse pattern, cholangiocarcinoma shows a sparse pattern, hepatic adenoma shows a patchy pattern, and focal nodular hyperplasia shows a cord-like pattern, which, when combined with tumor histological morphology, helps in differential diagnosis.
③ Heat shock protein 70: positive staining in the cytoplasm or nucleus of hepatocellular carcinoma.
④ Glutamine synthetase: usually shows diffuse strong positivity in hepatocellular carcinoma; some hepatic adenomas, especially β-catenin mutation-activated hepatic adenomas, may also show diffuse positivity; in HGDN, it shows moderate intensity focal staining, with positive cells <50%; in focal nodular hyperplasia, it shows characteristic irregular map-like staining; in normal liver tissue, only hepatocytes around the central vein are stained, and these characteristics assist in differential diagnosis.
ICC:
① Mucins: positive staining in cholangiocarcinoma cell membranes.
② Cytokeratin (CK) 7/CK19: positive staining in cholangiocarcinoma cell cytoplasm.
③ Mucin-1: positive staining in cholangiocarcinoma cell membranes.
Although the positivity of the above markers can suggest tumors of biliary epithelial origin, they can also show positive expression in non-tumor bile duct epithelium, requiring careful differentiation.
cHCC-CCA:
Both HCC and ICC components express their respective tumor markers. In addition, positive expression of markers such as CD56, CD117, and epithelial cell adhesion molecule (EpCAM) may suggest the presence of stem cell differentiation characteristics in the tumor, indicating a more aggressive nature.
Pathological Assessment of Resection Specimens After Conversion/Neoadjuvant Therapy
Pathological evaluation of resected liver cancer specimens
Sampling: For liver cancer resection specimens marked clinically as having undergone conversion/neoadjuvant therapy, the following procedures can be followed: incise and measure the three-dimensional size at the maximum diameter of the tumor bed (the original position of the tumor before treatment). For small liver cancers with a maximum diameter of ≤3cm, all should be sampled; for tumors >3cm, the tumor should be incised at 0.5-1 cm intervals at the maximum diameter to select the most representative sections of tumor necrosis and residual tumor, ensuring that both the tumor bed and surrounding liver tissue are preserved for mutual comparison. Photographs of the gross specimens can also be taken for histological observation comparison.
Microscopic Evaluation: The main assessment of liver cancer resection specimens focuses on the proportions of three components in the tumor bed:
① Necrotic tumor;
② Viable tumor;
③ Tumor stroma (fibrous tissue and inflammation).
The sum of these three areas in the tumor bed equals 100%. The pathological report should indicate the number of samples taken, and the average percentage of residual tumor should be determined based on the assessment of the three components in each section.
Complete Pathological Response and Significant Pathological Response Assessment: These are important pathological indicators for evaluating the efficacy of preoperative treatment and exploring the best timing for surgery.
Complete Pathological Response (CPR): Refers to the absence of viable tumor cells upon complete assessment of the tumor bed specimen after preoperative treatment.
Significant Pathological Response (MPR): Refers to the reduction of viable tumor cells to below the threshold that can affect clinical prognosis after preoperative treatment. In lung cancer research, MPR is often defined as residual tumor cells in the tumor bed reduced to ≤10%, which correlates with studies on the degree of tumor necrosis and prognosis after TACE treatment in liver cancer. The specific threshold for MPR still requires further clinical research for confirmation. It is recommended to broaden the sampling scope for tumors initially diagnosed as MPR to clarify.
Histological assessment methods for the degree of necrosis in liver cancer specimens after immune checkpoint inhibitor therapy can refer to related tumor types with more research conducted, deepening the understanding of the histological characteristics of liver cancer while observing for any immune-related liver injuries in the peritumoral liver tissue, including hepatocyte damage, lobular hepatitis, and cholangitis.
Pathological Diagnosis Report of Liver Cancer
The report mainly consists of gross specimen description, microscopic description, immunohistochemical examination, and pathological diagnosis name, with additional explanations and suggestions provided to clinicians when necessary (Table 1). Additionally, molecular pathological examination results related to the clonal origin detection of liver cancer, drug target detection, biological behavior assessment, and prognosis judgment can be attached to provide clinical reference.
Summary of Key Points
1. The standardized handling and prompt submission of liver cancer resection specimens are crucial for maintaining tissue and cell integrity and ensuring accurate pathological diagnosis.
2. The sampling of liver cancer specimens should follow the “seven-point baseline sampling” standard, which aids in obtaining representative pathological biological characteristic information of liver cancer.
3. The content of the pathological diagnosis report for liver cancer should be standardized and comprehensive, with particular emphasis on the diagnosis and pathological grading assessment of MVI, an important factor affecting the prognosis of liver cancer.
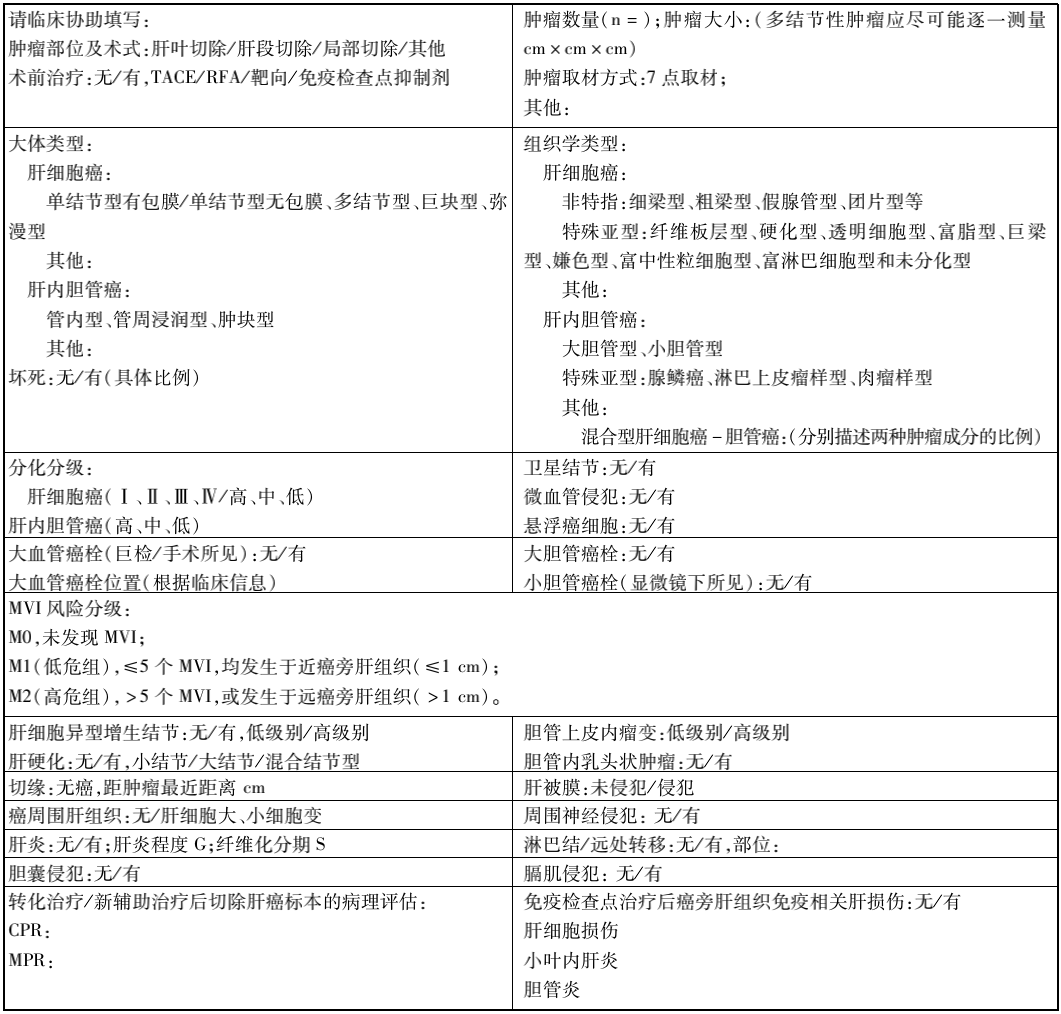
Table 1 Recommended liver cancer pathological diagnosis report and main descriptive indicators
Clinical Diagnosis Criteria and Flowchart for Liver Cancer
Based on the high-risk factors, imaging characteristics, and serological molecular markers of liver cancer, clinical diagnosis is performed according to the steps in the flowchart (Figure 2).
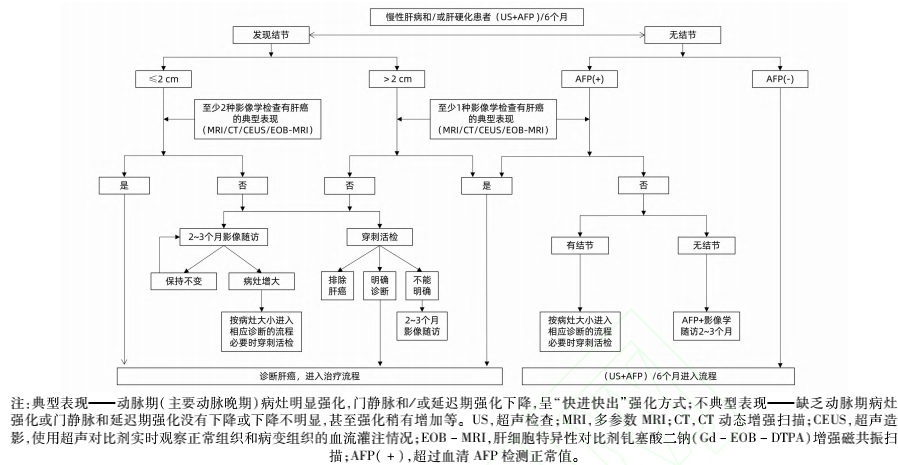
Figure 2 Liver Cancer Diagnosis Flowchart
1. For those with HBV or HCV infection, or any cause of liver cirrhosis, at least one ultrasound examination and serum AFP test should be conducted every six months. If a liver nodule with a diameter ≤ 2cm is found, and at least two of the four examinations (multiparametric MRI, dynamic contrast-enhanced CT, ultrasound contrast, or liver-specific contrast agent Gd-EOB-DTPA enhanced MRI) show significant enhancement in the arterial phase and low enhancement in the portal and/or delayed phase compared to liver parenchyma (the typical feature of liver cancer), a clinical diagnosis of liver cancer can be made; for nodules with a diameter >2cm, as long as one of the four imaging examinations shows a typical liver cancer feature, a clinical diagnosis of liver cancer can be made.
2. For those with HBV or HCV infection, or any cause of liver cirrhosis, if a liver nodule with a diameter ≤ 2cm is found and none or only one of the four imaging examinations shows a typical liver cancer feature, liver biopsy or follow-up imaging examinations every 2-3 months combined with serum AFP levels should be performed to confirm the diagnosis. For nodules with a diameter > 2cm, if none of the four imaging examinations show typical liver cancer features, liver biopsy or follow-up imaging examinations every 2-3 months combined with serum AFP levels should be performed to confirm the diagnosis.
3. For those with HBV or HCV infection, or any cause of liver cirrhosis, if serum AFP is elevated, especially if it is persistently elevated, imaging examinations should be conducted to confirm liver cancer diagnosis; if any of the four imaging examinations show a typical liver cancer feature, a clinical diagnosis of liver cancer can be made; if no intrahepatic nodules are found, and after excluding pregnancy, chronic or active liver disease, germ cell tumors, and digestive tract tumors, serum AFP changes should be closely monitored, and imaging re-examinations should be conducted every 2-3 months.
Staging of Liver Cancer
The staging of liver cancer is crucial for treatment selection and prognosis assessment. There are various staging systems abroad, such as BCLC, TNM, JSH, and APASL. Based on China’s specific national conditions and practical experience, the China Liver Cancer Staging (CNLC) scheme has been established, which includes: CNLC Stage Ia, Ib, IIa, IIb, IIIa, IIIb, and IV, with specific staging descriptions shown in Figure 3.
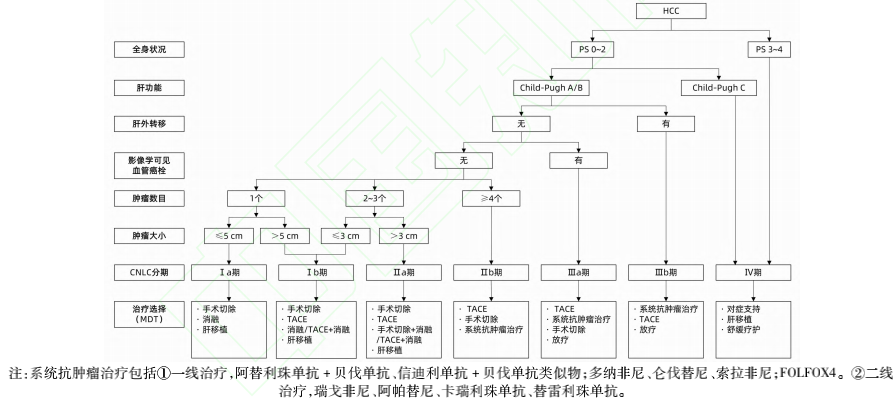
Figure 3 Clinical Staging and Treatment Flowchart for Liver Cancer in China
CNLC Stage Ia: PS 0~2 points, liver function Child-Pugh A/B, single tumor, diameter ≤ 5cm, with no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC Stage Ib: PS 0~2 points, liver function Child-Pugh A/B, single tumor, diameter > 5cm, or 2-3 tumors, maximum diameter ≤ 3cm, with no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC Stage IIa: PS 0~2 points, liver function Child-Pugh A/B, 2-3 tumors, maximum diameter > 3cm, with no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC Stage IIb: PS 0~2 points, liver function Child-Pugh A/B, ≥4 tumors, regardless of tumor diameter, with no radiologically visible vascular cancer thrombus or extrahepatic metastasis;
CNLC Stage IIIa: PS 0-2 points, liver function Child-Pugh A/B, regardless of tumor status, with radiologically visible vascular cancer thrombus but no extrahepatic metastasis;
CNLC Stage IIIb: PS 0~2 points, liver function Child-Pugh A/B, regardless of tumor status, with or without radiologically visible vascular cancer thrombus, with extrahepatic metastasis;
CNLC Stage IV: PS 3-4 points, or liver function Child-Pugh C, regardless of tumor status, with or without radiologically visible vascular cancer thrombus, with or without extrahepatic metastasis.
References:
National Health Commission Office “Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022)”, Medical Doctor Time
Recommended Reading:
1. Understanding: Common Drugs for Digestive Tract Tumors such as Liver Cancer, Gastric Cancer, Esophageal Cancer, and Intestinal Cancer (Medication Precautions)
2. “A Shot” Treatment for Cancer, 8 Questions about “Yttrium [90Y] Microspheres”
——End of this issue——
We (Medical World Image, WeChat ID: medhealife) are committed to reporting research achievements in the field of tumors and disseminating popular science knowledge;
We focus on tumor prevention, early screening and diagnosis, treatment, and rehabilitation management throughout the entire life cycle of tumors;
Providing the latest information for doctors, patients, and related personnel;
Contributing to the benefit of medicine for the people.
