Antibody-drug conjugates (ADCs) have become a popular avenue in tumor treatment in recent years, typically covalently linking monoclonal antibodies (mAbs) with cytotoxic drugs (payloads) via chemically synthesized linkers. ADCs combine the advantages of highly specific targeting capabilities and effective killing actions, achieving precise and efficient clearance of cancer cells.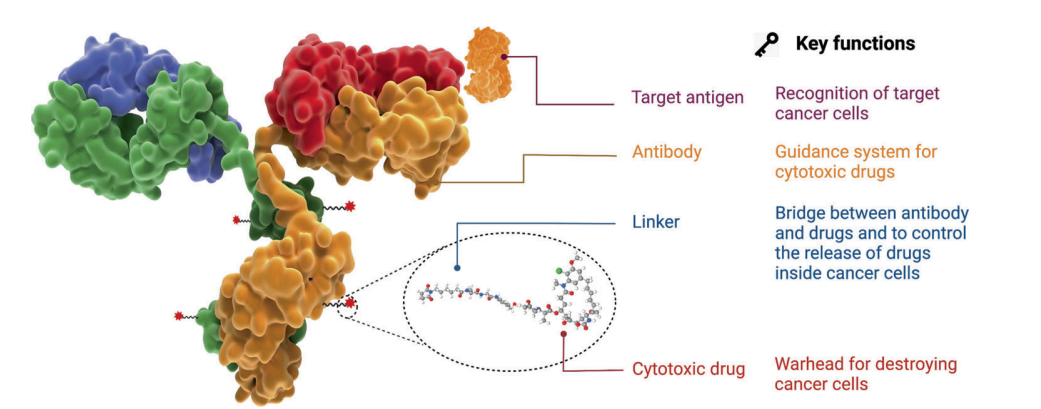 Figure 1. Structure and characteristics of ADC drugsSince the FDA approved the first ADC product, Mylotarg® (gemtuzumab ozogamicin), in 2000, as of December 2021, a total of 14 ADCs have received market approval globally for hematologic malignancies and solid tumors. Additionally, over 100 ADC candidates are currently in various stages of clinical trials.
Figure 1. Structure and characteristics of ADC drugsSince the FDA approved the first ADC product, Mylotarg® (gemtuzumab ozogamicin), in 2000, as of December 2021, a total of 14 ADCs have received market approval globally for hematologic malignancies and solid tumors. Additionally, over 100 ADC candidates are currently in various stages of clinical trials.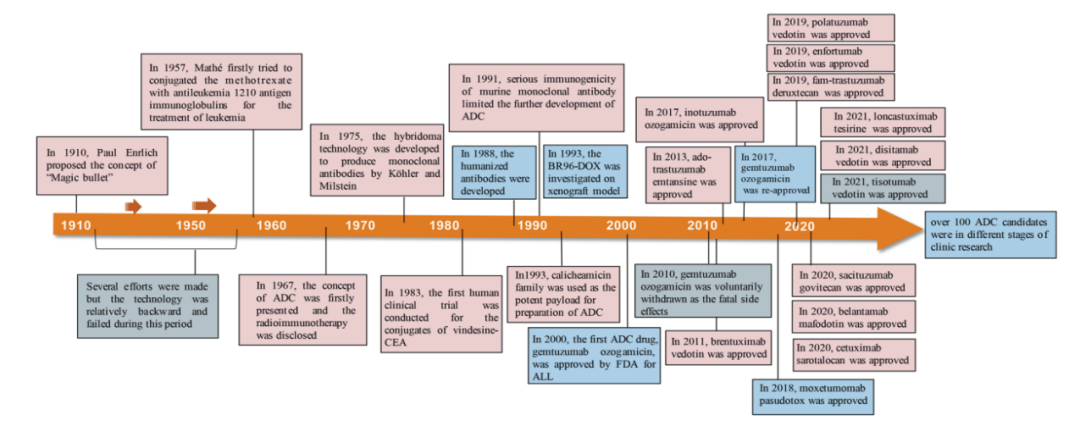 Figure 2. Key events in the development and approval process of ADC drugsHowever, the road to developing innovative oncology products is not always smooth, and the ADC field is no exception. For instance, the first globally marketed ADC product, Mylotarg®, and the recently failed Phase III clinical trial of Blenrep® serve as examples.
Figure 2. Key events in the development and approval process of ADC drugsHowever, the road to developing innovative oncology products is not always smooth, and the ADC field is no exception. For instance, the first globally marketed ADC product, Mylotarg®, and the recently failed Phase III clinical trial of Blenrep® serve as examples.
Blenrep® Phase III Study Failure
- On November 7, 2022, GlaxoSmithKline’s BCMA-targeted ADC product Blenrep® (belantamab mafodotin) failed in a Phase III clinical trial (DREAMM-3) for patients with a type of blood cancer, as it did not achieve the primary endpoint of progression-free survival (PFS) compared to the control group receiving low-dose dexamethasone in combination with pomalidomide. Previously, Blenrep (belantamab mafodotin) had received accelerated approval from the US FDA as a monotherapy for adult patients with relapsed or refractory multiple myeloma (RRMM) who had received at least four prior therapies.
Mylotarg®’s Two Market Launches
- In 2000, the FDA granted accelerated approval for Pfizer’s CD33-targeted ADC product Mylotarg® as a single-agent (high-dose) therapy for adult patients with CD33-positive acute myeloid leukemia (AML) who had experienced their first relapse, were aged ≥60 years, and were not suitable for other cytotoxic chemotherapy. This was the first launch of Mylotarg®, making it the world’s first commercialized ADC product. However, shortly after its launch, due to safety issues, Pfizer announced in 2010 that Mylotarg® would be withdrawn from the US market.
- On September 1, 2017, Pfizer regained FDA approval by updating clinical evidence, adjusting drug specifications and administration regimens for: (1) newly diagnosed CD33-positive AML adult patients; (2) patients aged ≥2 years with CD33-positive, relapsed or refractory AML.
The efficacy and safety of ADCs, therapeutic windows, target limitations, and the heterogeneity of solid tumors and hematologic malignancies have all become limiting factors in ADC development.This article aims to explore the key components of ADCs and the mechanisms by which these key factors influence ADC activity through a review of the development history and mechanisms of ADCs, and to predict the development prospects of next-generation ADC products.
Antigen Selection for ADCs
The target antigens expressed on tumor cells serve as the navigation direction for ADC drugs to recognize tumor cells, and they also determine the mechanism by which the cytotoxic payload is delivered into tumor cells (e.g., endocytosis). Therefore, appropriate selection of target antigens is the primary consideration in ADC development.
- First, to reduce off-target toxicity, the targeted antigen should be expressed or predominantly expressed in tumor cells but minimally expressed in normal tissues. Ideally, the antigen should be a surface (or extracellular) antigen rather than an intracellular antigen, so that it can be recognized by circulating ADCs. For example, the expression of HER2 receptors in certain types of tumors is approximately 100 times higher than in normal cells, laying a solid foundation for the development of ado-trastuzumab emtansine (TDM-1, KADCYLA®), fam-trastuzumab deruxtecan (DS-8201a, Enhertu®), and disitamab vedotin (RC48, Aidixi®);
- Second, the targeted antigen should be non-secreted, as secreted antigens in circulation can lead to unwanted binding of ADCs outside the tumor site, reducing tumor targeting and increasing adverse reactions;
- Third, the targeted antigen should ideally be internalized upon binding with the corresponding antibody, allowing the ADC-antigen complex to effectively enter cancer cells, followed by appropriate intracellular transport pathways and rapid release of the cytotoxic payload.
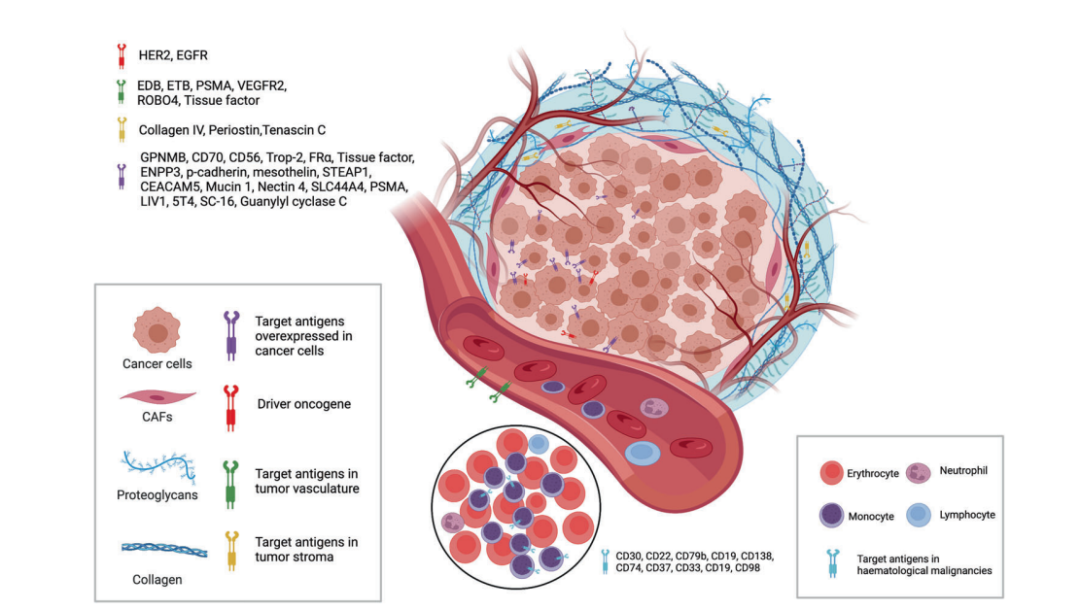 Figure 3. Available targets from tumor cells and tumor microenvironment for ADCsCurrently, as shown in the figure above, the target antigens of approved ADC drugs are typically specific proteins that are overexpressed in cancer cells, including HER2, trop2, nectin4, and EGFR in solid tumors, as well as CD19, CD22, CD33, CD30, BCMA, and CD79b in hematologic malignancies. Driven by foundational research in oncology and immunology, the selection of ADC target antigens has gradually expanded from traditional tumor cell antigens to targets in the tumor microenvironment, such as stroma and vascular systems. Emerging new evidence from preclinical and clinical studies suggests that components of the neovasculature, subendothelial extracellular matrix, and tumor stroma may serve as valuable target antigens for ADC drug development.
Figure 3. Available targets from tumor cells and tumor microenvironment for ADCsCurrently, as shown in the figure above, the target antigens of approved ADC drugs are typically specific proteins that are overexpressed in cancer cells, including HER2, trop2, nectin4, and EGFR in solid tumors, as well as CD19, CD22, CD33, CD30, BCMA, and CD79b in hematologic malignancies. Driven by foundational research in oncology and immunology, the selection of ADC target antigens has gradually expanded from traditional tumor cell antigens to targets in the tumor microenvironment, such as stroma and vascular systems. Emerging new evidence from preclinical and clinical studies suggests that components of the neovasculature, subendothelial extracellular matrix, and tumor stroma may serve as valuable target antigens for ADC drug development.
Antibody Selection for ADCs
Tumor-targeting antibodies are crucial for the specific binding between the target antigen and ADC. In addition to having high binding affinity for the target antigen, the ideal antibody portion should promote effective internalization, exhibit low immunogenicity, and have a long plasma half-life.In the early stages of ADC drug development, murine antibodies were primarily used, but the failure rate was high due to severe immunogenicity-related side effects. With the advent of recombinant technology, murine antibodies have largely been replaced by chimeric and humanized antibodies. Currently, ADCs increasingly utilize fully humanized antibodies with significantly reduced immunogenicity. Most antibodies used for ADC drugs are immunoglobulin G (IgG) antibodies, including four subclasses: IgG1, IgG2, IgG3, and IgG4.
- IgG1 is the commonly used antibody subclass for ADCs because it is the most abundant in serum and can induce potent effector functions through high binding affinity to Fc receptors, such as antibody-dependent cell-mediated cytotoxicity (ADCC), antibody-dependent phagocytosis (ADCP), and complement-dependent cytotoxicity (CDC). These Fc-mediated effector functions play a crucial role in the anticancer activity of antibody drugs.
- Due to rapid clearance, IgG3 is rarely used for ADCs. Unlike the other three subclasses, which have a half-life of about 21 days, IgG3 has a half-life of only about 7 days in serum.
- IgG2 often exhibits a tendency to form dimers and aggregates in vivo, leading to reduced concentrations of ADC drugs.
- IgG4 can induce ADCP; however, IgG4 is an atypical dynamic antibody with Fab arm exchange, leading to reduced potency and ineffective targeting.
Regarding the internalization of the antibody-antigen complex, the efficiency mainly depends on the binding affinity between the antibody and tumor cell surface antigen, with higher affinity usually leading to faster internalization. However, antibodies with high antigen affinity may conversely reduce penetration into solid tumors. Treating solid tumors is more complex than treating hematologic malignancies because of the presence of a “binding site barrier (BSB)” in solid tumors, where extremely strong binding between antibodies and antigens leads to ADCs being captured near blood vessels after extravasation but less penetrating into tumor cells far from blood vessels. Therefore, optimizing the reasonable affinity between antigens and antibodies is necessary to balance rapid uptake in target cells and anticancer efficacy.In addition to binding affinity, another factor affecting tumor penetration is the size of the antibody. The large molecular weight of IgG antibodies (approximately 150 kDa) often limits their ability to penetrate capillaries and stroma in tumor tissues. Therefore, early ADCs primarily targeted hematologic malignancies. To better apply ADCs in solid tumor treatment, researchers have attempted to miniaturize antibodies by removing Fc fragments. Miniaturized antibodies not only retain high affinity and specificity but also penetrate solid tumors more easily through blood vessels, significantly enhancing their killing effect against solid tumors. However, this change can lead to a shortened in vivo half-life. Therefore, when designing ADCs with miniaturized antibodies, it is essential to consider various factors for reasonable optimization.
Linker Selection for ADCs
The linker in ADCs connects the antibody with the cytotoxic drug. It is one of the key factors related to ADC stability and payload release kinetics, thus important for the final therapeutic index of the ADC.An ideal linker should not induce ADC aggregation, is expected to limit the premature release of the payload in plasma, and promote the release of active drugs at the desired targeted sites. Based on the metabolic pathways within cells, most ADC drugs utilize two types of linkers, including cleavable linkers and non-cleavable linkers. Cleavable linkers leverage environmental differences between systemic circulation and tumor cells to accurately release free cytotoxic drugs and can be further divided into chemical cleavable linkers (hydrazone bonds and disulfide bonds) and enzyme-cleavable linkers (glucuronide bonds and peptide bonds). Hydrazone is a typical acid-sensitive (pH-sensitive) linker.Cleavable linkers utilize environmental differences between systemic circulation and tumor cells to accurately release free cytotoxic drugs and can be further divided into chemical cleavable linkers (hydrazone bonds and disulfide bonds) and enzyme-cleavable linkers (glucuronide bonds and peptide bonds). Another type of chemically cleavable linker sensitive to reducing glutathione (GSH). GSH plays a crucial role in maintaining intracellular redox balance during cell survival, proliferation, and differentiation. The concentration of GSH in blood is much lower than the intracellular concentration in cancer cells. Therefore, this type of linker can remain stable in the bloodstream while specifically releasing active payloads in cancer cells.Peptide-based linkers are sensitive to lysosomal proteases and have been used in many ADCs. Lysosomal proteases, such as cathepsin B, are often overexpressed in cancer cells, allowing for accurate drug release near tumors. Additionally, due to the presence of protease inhibitors in the bloodstream, enzyme-cleavable linkers are generally stable in systemic circulation, thus reducing various risks associated with premature cleavage. Among the approved ADC drugs, 9 out of 14 use peptide-based linkers.Non-cleavable linkers (e.g., thioether or maleimide-based) are inert to common chemical and enzymatic environments in vivo. The main advantage of non-cleavable linkers is their lower off-target toxicity due to increased plasma stability, but the bystander effect of the payload is affected.
Payload Selection for ADCs
Cytotoxic payloads are the warheads that exert cytotoxic effects once ADCs are internalized into cancer cells. Since only about 2% of ADCs can reach the targeted tumor site after intravenous administration, high-potency payloads (with IC50 in the nM and pM range) are critical in ADC development. Additionally, these compounds should remain stable under physiological conditions and possess available functional groups for binding with antibodies.Currently, the cytotoxic payloads used for ADCs primarily include potent microtubule inhibitors, DNA-damaging agents, and immunomodulators (Table 1).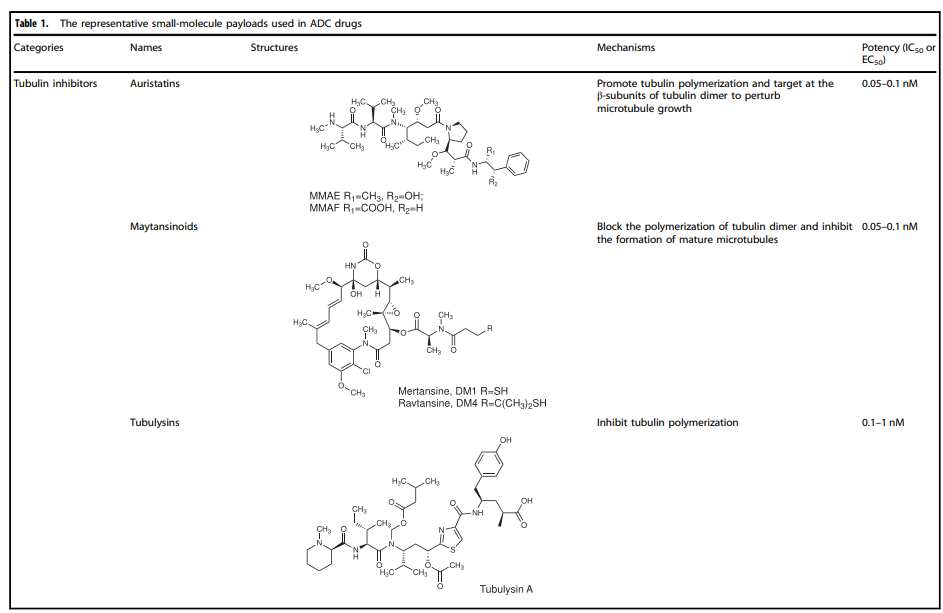
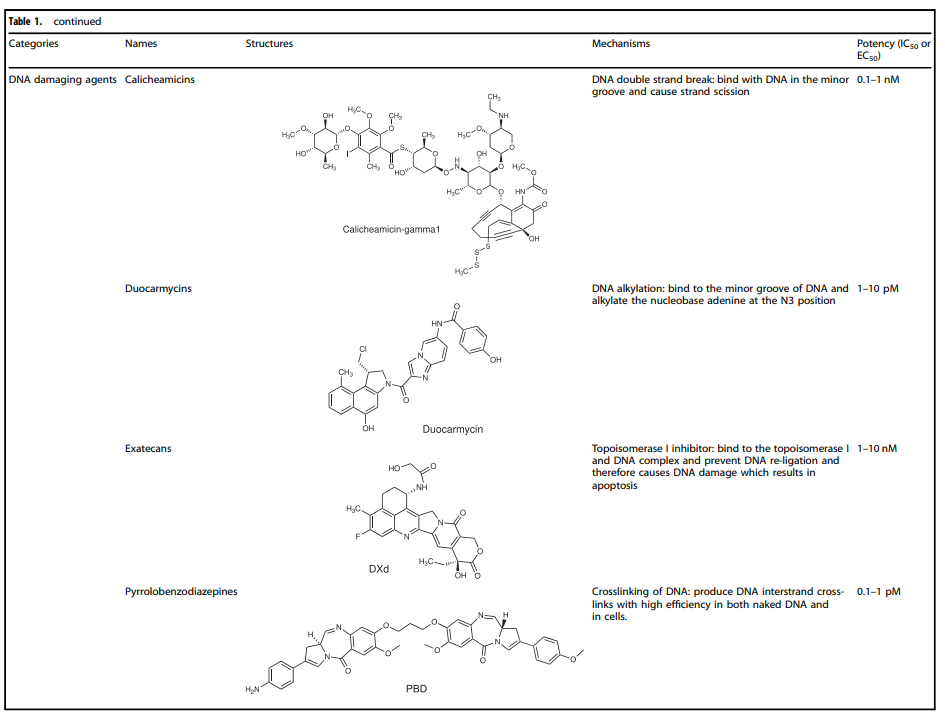
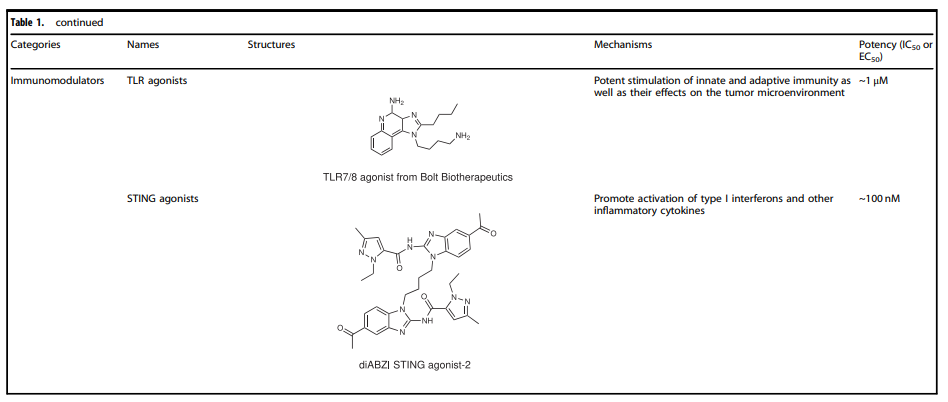 Table 1. Representative small molecule payloads used in ADC drugs
Table 1. Representative small molecule payloads used in ADC drugs
Microtubule Disruptors
Microtubules are a major component of the cytoskeleton and play a crucial role in cell division, especially during the rapid proliferation of tumor cells. Microtubule inhibitors have become important anticancer drugs. Auristatins are significant payloads used in ADCs, with monomethyl auristatin E (MMAE) or monomethyl auristatin F (MMAF) being the mainstream payloads for ADC development. Among the 14 approved ADC drugs, 5 use MMAE/MMAF as payloads.
Maytansinoid Derivatives (DM1 and DM4)Maytansine is a highly effective microtubule assembly inhibitor that can induce cell mitosis to stop. However, this structure is challenging to conjugate due to its lack of reactive functional groups. To overcome this issue, a series of highly effective derivatives containing SMe groups have been created. The first examples of this class of molecules are DM1 and DM4, which contain a methylthioacetyl group instead of the natural N-acetyl group.The FDA-approved ado-trastuzumab emtansine (TDM-1, KADCYLA®) in 2013 was the first ADC drug conjugated with maytansinoid derivatives. Additionally, microtubule proteases (microtubule protease A-D, isolated from slime molds) represent another class of microtubule polymerization inhibitors that show good anticancer activity. For example, EC1169, a microtubule lysate B hydrazone conjugate targeting prostate-specific membrane antigen (PSMA), is currently under clinical trial (NCT02202447).
DNA Damaging AgentsCompared to the IC50 values of microtubule inhibitors in the nmol range (half-maximal inhibitory concentration), the IC50 values of DNA damaging agents can reach the pmol level, making ADCs conjugated with DNA damaging agents sometimes more effective and possibly working independently of the cell cycle (unlike microtubule inhibitors that primarily work during mitosis), and they can even be used for cells with low antigen expression.The detailed mechanisms involved with DNA damaging agents mainly include: (i) DNA double-strand breaks, such as calicheamicin; (ii) DNA alkylation, such as duocarmycin; (iii) DNA intercalation, such as topoisomerase I inhibitors; (iv) DNA cross-linking, pyrrolobenzodiazepines (PBD). It is precisely the various functions of the payload itself that inhibit tumor cell growth or directly kill tumor cells, enriching the action mechanisms of ADC drugs.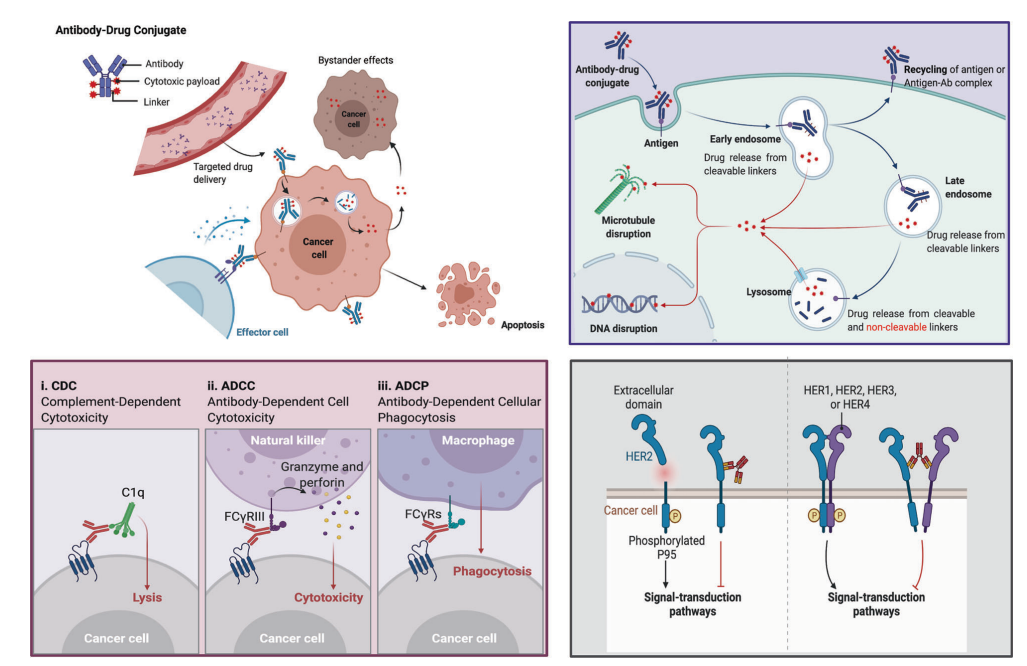 Figure 4. Overview of mechanisms by which ADCs kill cancer cellsUpper right: Main core action mechanisms of ADCs; lower left: ADC antibody components interact with immune effector cells, triggering antitumor immunity, including CDC, ADCC, and ADCP effects; lower right: ADC antibody components retain their active characteristics, thus interfering with target functions and inhibiting downstream signaling pathways that suppress tumor growth.Even with numerous antitumor mechanisms arising from the tumor-targeting clearance effect of ADCs themselves, the cytotoxic effects received by the antibody, and the multiple anticancer mechanisms of the payload, the key to ADC success lies in the conjugation method of the antibody, payload, and linker.
Figure 4. Overview of mechanisms by which ADCs kill cancer cellsUpper right: Main core action mechanisms of ADCs; lower left: ADC antibody components interact with immune effector cells, triggering antitumor immunity, including CDC, ADCC, and ADCP effects; lower right: ADC antibody components retain their active characteristics, thus interfering with target functions and inhibiting downstream signaling pathways that suppress tumor growth.Even with numerous antitumor mechanisms arising from the tumor-targeting clearance effect of ADCs themselves, the cytotoxic effects received by the antibody, and the multiple anticancer mechanisms of the payload, the key to ADC success lies in the conjugation method of the antibody, payload, and linker.
Conjugation Methods
The conjugation sites and methods determine the drug-to-antibody ratio (DAR) and significantly impact the stability of the ADC and its pharmacokinetic – pharmacodynamic characteristics. High drug loads often lead to rapid plasma clearance, while low DAR ADCs exhibit weaker activity.
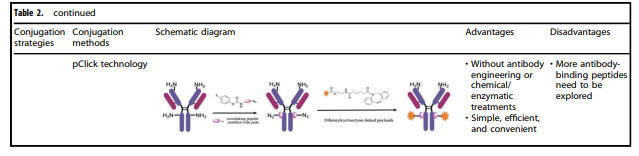 Table 2. Characteristics of various conjugation methods applied to ADCsTable 2 summarizes the characteristics of various commonly used conjugation methods for ADCs. Among them, chemical conjugation and enzyme conjugation are currently the two most widely used methods for linking antibodies and payload components.
Table 2. Characteristics of various conjugation methods applied to ADCsTable 2 summarizes the characteristics of various commonly used conjugation methods for ADCs. Among them, chemical conjugation and enzyme conjugation are currently the two most widely used methods for linking antibodies and payload components.
Chemical Conjugation
Chemical conjugation involves linking the handle part of the linker to accessible amino acid residues on the antibody, avoiding the complexity of identifying suitable mutation sites and potential challenges in scaling and optimizing cell culture. Early chemical conjugation methods exhibited great randomness in DAR and conjugation sites, resulting in significant variations in the produced ADCs and insufficient uniformity in quality.
Enzyme Conjugation
By using genetically encoded amino acid tags inserted into the antibody sequence, payload attachment can be achieved in a highly selective manner. These tags are specifically chosen to be recognized by enzymes capable of executing site-specific conjugation, such as formylglycine-generating enzyme (FGE), microbial transglutaminase (MTG), sortase, or tyrosinase.
Potential Development Directions for ADCs
With the continuous optimization of conjugation technology and advancements in antibody engineering technology, more ADC products targeting other targets are currently under clinical exploration. Examples include Trop2 ADC and Claudin18.2 ADC; among them, PD-L1 ADCs are also being explored by several companies.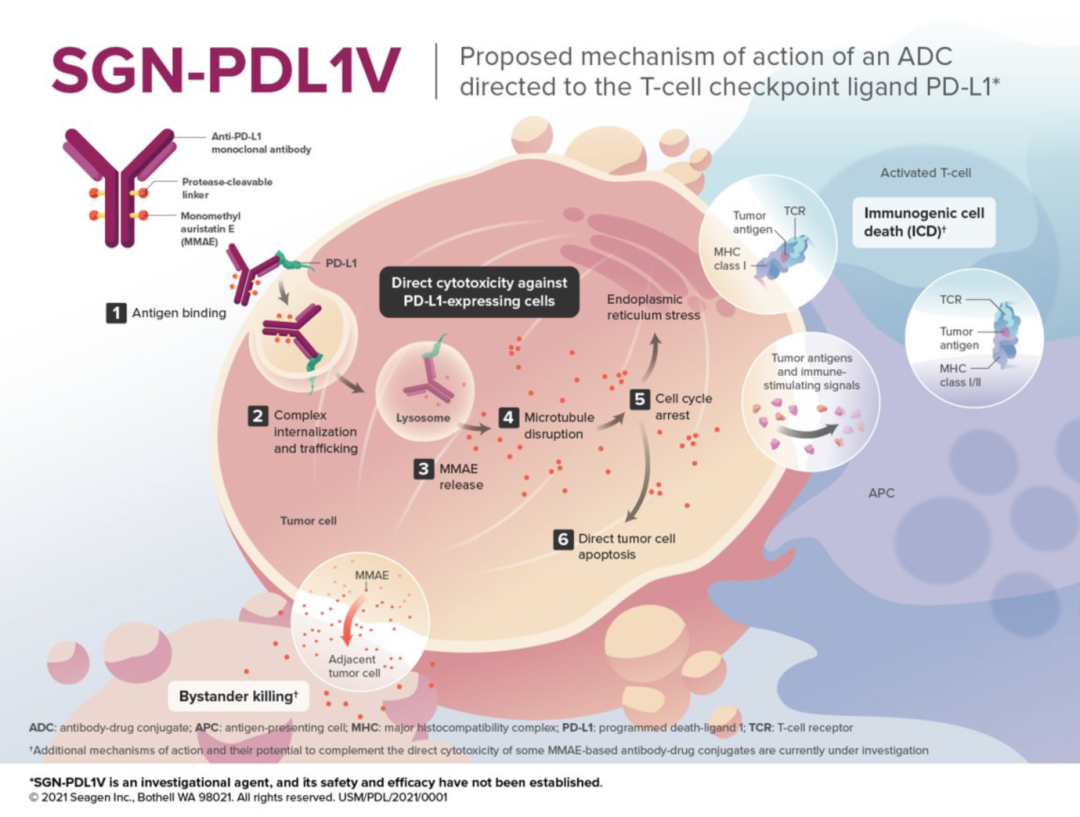 Figure 5. Mechanism of SGN-PDL1V (Source: 2021 SITC)For instance, SGN-PDL1V, a novel ADC product targeting PD-L1 in the early stages of development by Seagen, uses MMAE as the payload. MMAE (monomethyl auristatin E) is the most widely used payload in ADCs, accounting for approximately 30% of the total, primarily exerting effective mitotic inhibition by suppressing microtubule polymerization.ADCs show drug concentrations in tumor tissues >100 times higher, significantly expanding the therapeutic window of cytotoxic agents and effectively reducing the adverse reactions caused by systemic chemotherapy, thus enabling the exploration of combining ADCs with other tumor treatment modalities.Furthermore, the linker of SGN-PDL1V is protease-cleavable. The antibody is a fully humanized anti-PD-L1 monoclonal antibody (Seagen PD-L1 monoclonal antibody). The Seagen PD-L1 monoclonal antibody utilizes a human IgG1-Fc scaffold, engineered to eliminate the effector functions of the Fc segment, including complement-dependent cytotoxicity (CDC), antibody-dependent cytotoxicity (ADCC), and antibody-dependent cellular phagocytosis (ADCP).Additionally, given that single-target antibodies often exhibit high rates of resistance, dual-target bispecific antibodies are also being explored as ADCs by some companies.
Figure 5. Mechanism of SGN-PDL1V (Source: 2021 SITC)For instance, SGN-PDL1V, a novel ADC product targeting PD-L1 in the early stages of development by Seagen, uses MMAE as the payload. MMAE (monomethyl auristatin E) is the most widely used payload in ADCs, accounting for approximately 30% of the total, primarily exerting effective mitotic inhibition by suppressing microtubule polymerization.ADCs show drug concentrations in tumor tissues >100 times higher, significantly expanding the therapeutic window of cytotoxic agents and effectively reducing the adverse reactions caused by systemic chemotherapy, thus enabling the exploration of combining ADCs with other tumor treatment modalities.Furthermore, the linker of SGN-PDL1V is protease-cleavable. The antibody is a fully humanized anti-PD-L1 monoclonal antibody (Seagen PD-L1 monoclonal antibody). The Seagen PD-L1 monoclonal antibody utilizes a human IgG1-Fc scaffold, engineered to eliminate the effector functions of the Fc segment, including complement-dependent cytotoxicity (CDC), antibody-dependent cytotoxicity (ADCC), and antibody-dependent cellular phagocytosis (ADCP).Additionally, given that single-target antibodies often exhibit high rates of resistance, dual-target bispecific antibodies are also being explored as ADCs by some companies.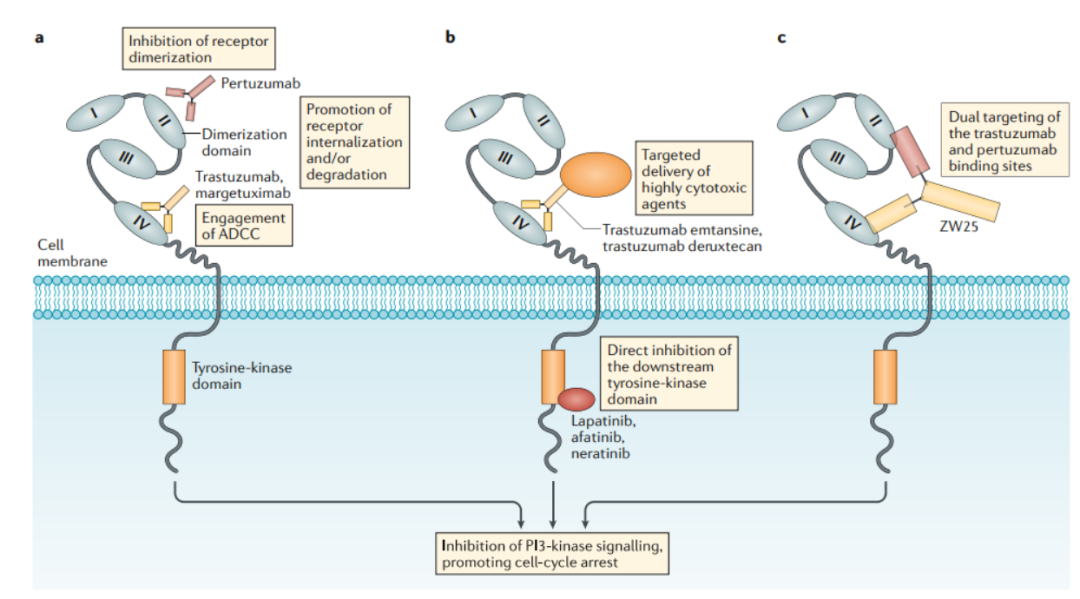 Figure 6. Mechanism of action of HER2-targeted drugsThis field is still in the early exploratory stages, with the fastest progress being ZW-49, a bispecific antibody ADC developed by Zymeworks utilizing its proprietary Azymetric™ Bispecifics and ZymeLink™ ADCs platforms. It can specifically bind to two non-overlapping epitopes of the HER2 receptor, namely the pertuzumab binding site and trastuzumab binding site, aiming to achieve good therapeutic effects in clinical applications for patients resistant to trastuzumab, pertuzumab, and even new ADC drugs like TDM-1.We look forward to more novel ADCs being commercialized and benefiting a broader range of patients in the fields of solid tumors and hematologic malignancies.References:1. Signal Transduction and Targeted Therapy (2022) 7:932. Bioorg Chem. 2021 Nov;116:105366.3. Oh DY, et al. Nat Rev Clin Oncol. 2019;10.1038/s41571-019-0268-3.4. Mark D. Pegram, et al. Mol Cancer Ther; 20(8) August 2021.This article is reprinted from Beike Society/Beibei
Figure 6. Mechanism of action of HER2-targeted drugsThis field is still in the early exploratory stages, with the fastest progress being ZW-49, a bispecific antibody ADC developed by Zymeworks utilizing its proprietary Azymetric™ Bispecifics and ZymeLink™ ADCs platforms. It can specifically bind to two non-overlapping epitopes of the HER2 receptor, namely the pertuzumab binding site and trastuzumab binding site, aiming to achieve good therapeutic effects in clinical applications for patients resistant to trastuzumab, pertuzumab, and even new ADC drugs like TDM-1.We look forward to more novel ADCs being commercialized and benefiting a broader range of patients in the fields of solid tumors and hematologic malignancies.References:1. Signal Transduction and Targeted Therapy (2022) 7:932. Bioorg Chem. 2021 Nov;116:105366.3. Oh DY, et al. Nat Rev Clin Oncol. 2019;10.1038/s41571-019-0268-3.4. Mark D. Pegram, et al. Mol Cancer Ther; 20(8) August 2021.This article is reprinted from Beike Society/Beibei
Disclaimer
This article is a reprint for sharing purposes only and does not represent the views of the platform. The copyright of the images and articles belongs to the original authors. If there is any infringement, please let us know, and we will handle it promptly.
——————————-
「Long press」 Add Xiao Da via QR code「Join the group」Explore market frontiers with more industry partners Aimeda Medical ConsultingAimeda (Beijing) Medical Information Consulting Co., Ltd., established in April 2014, is a professional consulting service provider in the pharmaceutical industry. The company is committed to deeply integrating industrial policy research with real-world data mining, gaining insights into the impact of industry policies on the market, and providing forward-looking market analysis through professional research to offer comprehensive solutions for market access after product launch.
Aimeda Medical ConsultingAimeda (Beijing) Medical Information Consulting Co., Ltd., established in April 2014, is a professional consulting service provider in the pharmaceutical industry. The company is committed to deeply integrating industrial policy research with real-world data mining, gaining insights into the impact of industry policies on the market, and providing forward-looking market analysis through professional research to offer comprehensive solutions for market access after product launch.