Diuretics are the cornerstone of heart failure treatment. So, what are the commonly used diuretics? What are their characteristics? At the 15th Qianjiang International Cardiovascular Disease Conference, Professor Mao Wei from Zhejiang Provincial Hospital of Traditional Chinese Medicine shared his insights on these questions!
Recommended Common Diuretics
Professor Mao Wei mentioned that the 2018 heart failure guidelines in China categorize diuretics mainly into two types: sodium-excreting and water-excreting. Among them, the water-excreting diuretic is mainly tolvaptan, while sodium-excreting diuretics are divided into loop diuretics, thiazide diuretics, and potassium-sparing diuretics.
Additionally, Professor Mao pointed out the differences between the guidelines for diuretics in China and those in European countries:
In the recommendation for loop diuretics, the recommended dose of furosemide in China is lower than that in the European guidelines, while the recommended dose of torsemide is higher than that in the European guidelines;
In the recommendation for thiazide diuretics, the European guidelines include bendroflumethiazide;
In the recommendation for potassium-sparing diuretics, spironolactone is not classified as a diuretic in China, whereas in the ESC guidelines, spironolactone/eplerenone is included in both neurohormonal inhibitors and diuretics, and the AHA guidelines recommend spironolactone as an oral diuretic.
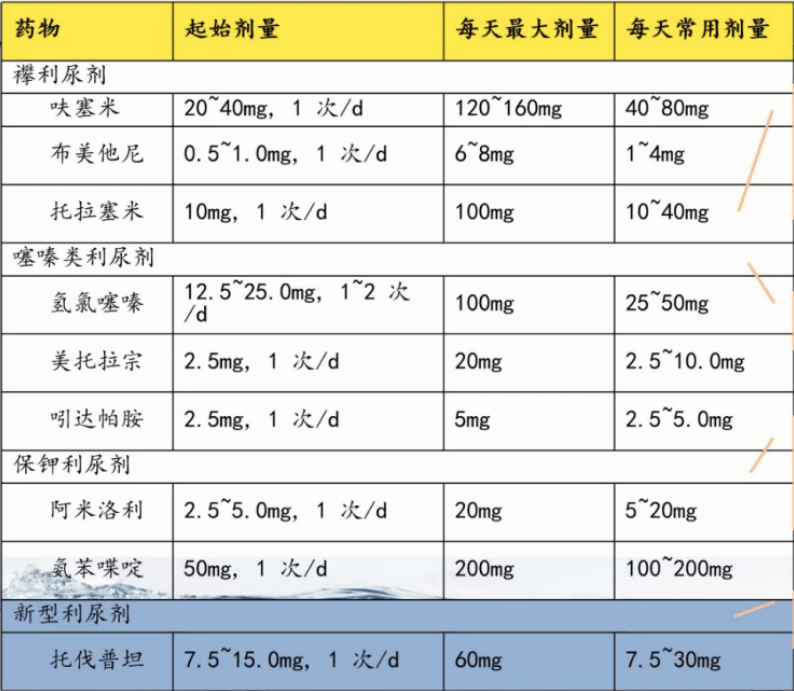
Figure 1. Recommended Diuretics in the 2018 Heart Failure Guidelines in China
Characteristics of Various DiureticsProfessor Mao then explained the characteristics of loop diuretics, thiazide diuretics, potassium-sparing diuretics, and various new diuretics.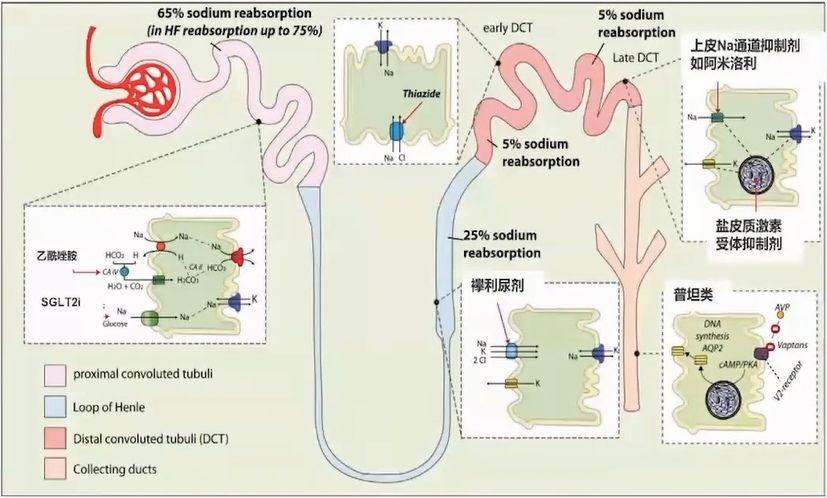 Figure 2. Target Sites of Different Diuretics1. Loop DiureticsSuitable for most heart failure patients, especially those with significant fluid retention or impaired renal function, including furosemide, torsemide, and bumetanide.Patients with severe renal impairment [eGFR < 15 mL/(min·1.73 m²)] require increased doses.40 mg furosemide, 20 mg torsemide, 1 mg bumetanide have comparable diuretic effects.When there is no severe renal impairment, the diuretic effect of furosemide injection is equivalent to 2 times that of the oral form (i.e., intravenous furosemide 10 mg = oral furosemide 20 mg);due to the higher oral bioavailability (80%-100%) of torsemide and bumetanide, which is less affected by intestinal congestion, the efficacy of intravenous and oral forms is similar.Moreover, Professor Mao particularly emphasized that loop diuretics are a threshold drug, meaning that diuretic action occurs only when the concentration exceeds the threshold. As the blood concentration increases, the diuretic effect follows an S-shaped curve, reaching a plateau at commonly used doses.In patients with acute decompensated heart failure (ADHF), the concentration-effect curve for diuretics shifts to the right, the maximum effect plateau decreases, and the diuretic threshold increases.
Figure 2. Target Sites of Different Diuretics1. Loop DiureticsSuitable for most heart failure patients, especially those with significant fluid retention or impaired renal function, including furosemide, torsemide, and bumetanide.Patients with severe renal impairment [eGFR < 15 mL/(min·1.73 m²)] require increased doses.40 mg furosemide, 20 mg torsemide, 1 mg bumetanide have comparable diuretic effects.When there is no severe renal impairment, the diuretic effect of furosemide injection is equivalent to 2 times that of the oral form (i.e., intravenous furosemide 10 mg = oral furosemide 20 mg);due to the higher oral bioavailability (80%-100%) of torsemide and bumetanide, which is less affected by intestinal congestion, the efficacy of intravenous and oral forms is similar.Moreover, Professor Mao particularly emphasized that loop diuretics are a threshold drug, meaning that diuretic action occurs only when the concentration exceeds the threshold. As the blood concentration increases, the diuretic effect follows an S-shaped curve, reaching a plateau at commonly used doses.In patients with acute decompensated heart failure (ADHF), the concentration-effect curve for diuretics shifts to the right, the maximum effect plateau decreases, and the diuretic threshold increases.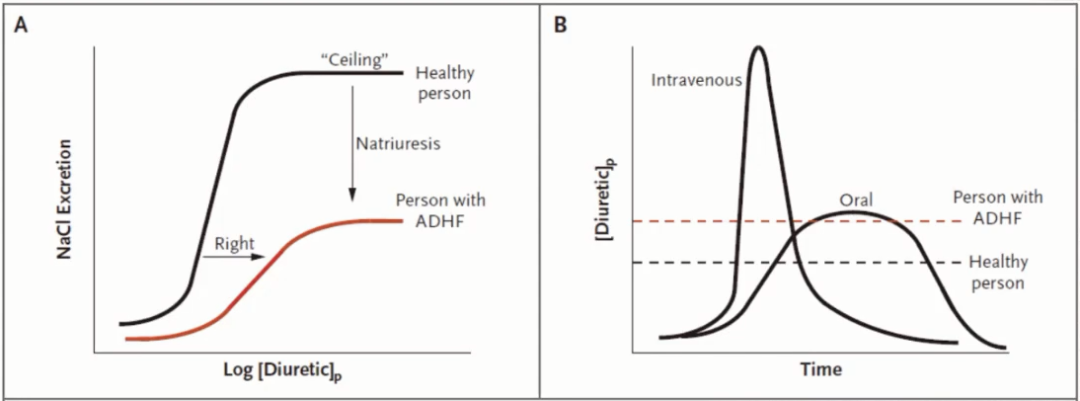 Figure 3. Pharmacokinetic Characteristics of Loop Diuretics2. Thiazide DiureticsThiazide diuretics have weaker diuretic effects compared to loop diuretics and are only suitable for heart failure patients with mild fluid retention and normal renal function accompanied by hypertension.Hydrochlorothiazide 100 mg/d has reached its maximum effect (the dose-effect curve has plateaued), and further increases are ineffective.In patients with renal impairment [eGFR < 30 mL/(min·1.73 m²)], the effect of thiazide diuretics is diminished, and their use is not recommended; however, in patients with resistant edema (furosemide daily dose exceeding 80 mg), thiazide diuretics can be combined with loop diuretics.3. Potassium-Sparing DiureticsAmiloride and triamterene have weak diuretic effects and are generally used in combination with other diuretics. Aldosterone receptor antagonists are also potassium-sparing diuretics.Clinically, non-diuretic doses of low-dose aldosterone receptor antagonists are mainly used to improve myocardial remodeling, such as spironolactone 20 mg or eplerenone 25-50 mg.To achieve diuretic effects, high doses of aldosterone receptor antagonists, such as 50-100 mg spironolactone, are required. Eplerenone is a selective aldosterone receptor antagonist with minimal effects on sex hormone receptors and fewer side effects.4. Vasopressin V2 Receptor AntagonistsThe representative of vasopressin receptor antagonists is tolvaptan. Tolvaptan does not need to be secreted into the renal tubule lumen to exert its effect, improving efficacy, and its diuretic effect does not depend on sodium and albumin levels.Tolvaptan is particularly effective in patients with resistant edema or hyponatremia, remaining effective in high-risk populations such as the elderly, those with low blood pressure, hypoalbuminemia, and renal impairment.It is recommended for patients with poor response to conventional diuretics, those with hyponatremia, or those at risk of renal impairment. Additionally, its main adverse effect is hypernatremia.Optimizing Treatment1. Patients with Acute Decompensated Heart Failure (ADHF)Should maintain a negative fluid balance of about 500-5000 mL/d based on sodium and water retention, gradually transitioning to a balanced intake. For those with significant pulmonary congestion, systemic congestion, and edema, strict water and intravenous infusion speed limits should be observed.For patients without obvious hypovolemia (massive bleeding, severe dehydration, excessive sweating, etc.), daily fluid intake is generally within 1500 mL, maintaining a negative fluid balance of about 500 mL per day.For patients with severe pulmonary edema, the fluid balance is 1000-2000 mL/d, which can reach up to 5000 mL/d in severe cases, transitioning to a rough balance after 3-5 days. Sodium intake should be limited to < 2 g/d.For ADHF patients with low perfusion, diuretics should be avoided until adequate perfusion is achieved.2. Diuretic ResistanceProfessor Mao suggested the following methods for management:
Figure 3. Pharmacokinetic Characteristics of Loop Diuretics2. Thiazide DiureticsThiazide diuretics have weaker diuretic effects compared to loop diuretics and are only suitable for heart failure patients with mild fluid retention and normal renal function accompanied by hypertension.Hydrochlorothiazide 100 mg/d has reached its maximum effect (the dose-effect curve has plateaued), and further increases are ineffective.In patients with renal impairment [eGFR < 30 mL/(min·1.73 m²)], the effect of thiazide diuretics is diminished, and their use is not recommended; however, in patients with resistant edema (furosemide daily dose exceeding 80 mg), thiazide diuretics can be combined with loop diuretics.3. Potassium-Sparing DiureticsAmiloride and triamterene have weak diuretic effects and are generally used in combination with other diuretics. Aldosterone receptor antagonists are also potassium-sparing diuretics.Clinically, non-diuretic doses of low-dose aldosterone receptor antagonists are mainly used to improve myocardial remodeling, such as spironolactone 20 mg or eplerenone 25-50 mg.To achieve diuretic effects, high doses of aldosterone receptor antagonists, such as 50-100 mg spironolactone, are required. Eplerenone is a selective aldosterone receptor antagonist with minimal effects on sex hormone receptors and fewer side effects.4. Vasopressin V2 Receptor AntagonistsThe representative of vasopressin receptor antagonists is tolvaptan. Tolvaptan does not need to be secreted into the renal tubule lumen to exert its effect, improving efficacy, and its diuretic effect does not depend on sodium and albumin levels.Tolvaptan is particularly effective in patients with resistant edema or hyponatremia, remaining effective in high-risk populations such as the elderly, those with low blood pressure, hypoalbuminemia, and renal impairment.It is recommended for patients with poor response to conventional diuretics, those with hyponatremia, or those at risk of renal impairment. Additionally, its main adverse effect is hypernatremia.Optimizing Treatment1. Patients with Acute Decompensated Heart Failure (ADHF)Should maintain a negative fluid balance of about 500-5000 mL/d based on sodium and water retention, gradually transitioning to a balanced intake. For those with significant pulmonary congestion, systemic congestion, and edema, strict water and intravenous infusion speed limits should be observed.For patients without obvious hypovolemia (massive bleeding, severe dehydration, excessive sweating, etc.), daily fluid intake is generally within 1500 mL, maintaining a negative fluid balance of about 500 mL per day.For patients with severe pulmonary edema, the fluid balance is 1000-2000 mL/d, which can reach up to 5000 mL/d in severe cases, transitioning to a rough balance after 3-5 days. Sodium intake should be limited to < 2 g/d.For ADHF patients with low perfusion, diuretics should be avoided until adequate perfusion is achieved.2. Diuretic ResistanceProfessor Mao suggested the following methods for management:
-
Increase the dose of loop diuretics;
-
Change the route of administration (IV push combined with continuous IV infusion: continuous IV and multiple applications can avoid sodium and water reabsorption due to decreased loop diuretic concentration);
-
Combine two or more diuretics, such as adding thiazide diuretics to loop diuretics, or adding vasopressin V2 receptor antagonists;
-
Use medications that increase renal blood flow, such as low-dose dopamine or recombinant human brain natriuretic peptide, to improve diuretic effects and renal function, and enhance renal perfusion, though benefits are unclear;
-
SGLT2 inhibitors;
-
Correct low blood pressure, hypoxemia, metabolic acidosis, hyponatremia, hypoalbuminemia, infection, etc., especially paying attention to correcting hypovolemia;
-
Ultrafiltration therapy.
Summary1. Diuresis is the fundamental treatment for volume overload in heart failure;2. Early combination of loop diuretics + tolvaptan + nesiritide;3. SGLT2 inhibitors can provide osmotic diuresis while lowering blood sugar, reducing blood pressure, and decreasing cardiac preload, making them a promising option for patients with HFrEF/HFpEF and diuretic resistance;4. If all diuretic strategies fail, ultrafiltration should be considered.▎Further Reading:“Guidelines for the Diagnosis and Treatment of Heart Failure in China (2018 Edition)”▼ Click “Read Original” to read for free Formatting: lySubmission: [email protected]Cover image source: ZcoolImages in the text source: Speaker’s PPT
Formatting: lySubmission: [email protected]Cover image source: ZcoolImages in the text source: Speaker’s PPT