This article, “Unveiling the Potential of Antibody-Drug Conjugates,” is an excellent industry review that provides a panoramic view of the hot field of Antibody-Drug Conjugates (ADCs). Next, we will journey from history to the future, delving into molecular mechanisms and clinical practices, connecting textbook knowledge to cutting-edge research.
A Precision Guided “Trojan Horse”: An In-Depth Analysis and Future Outlook on ADCs by a Medical Student
Abstract: In the long and arduous battle against cancer, the medical community has been pursuing the dream of the “magic bullet” proposed by Paul Ehrlich a century ago—a drug that can precisely kill diseased cells without harming healthy tissues. Today, Antibody-Drug Conjugates (ADCs) are bringing us closer than ever to this dream. This article will systematically dissect the core technologies, mechanisms of action, development history, and future challenges of ADCs from the perspective of a medical student, using a review article on the potential of ADCs as a blueprint. We will utilize knowledge from foundational courses such as immunology, pharmacology, and oncology as our “scalpel” to analyze the exquisite design of this “biological missile” and explore how it is reshaping the future landscape of cancer treatment and beyond.
1. Introduction: From “Carpet Bombing” to the Precision Medicine Revolution
As medical students, our understanding of cancer treatment often begins with the classic “three pillars” from textbooks—surgery, radiotherapy, and chemotherapy. Among these, the advent of chemotherapy drugs has greatly expanded our ability to combat systemic and metastatic tumors. However, traditional chemotherapy is essentially a “cytotoxic therapy” that resembles a “carpet bombing”; while it kills rapidly proliferating cancer cells, it inevitably damages normal cells that also divide quickly, such as hematopoietic cells, gastrointestinal epithelial cells, and hair follicle cells. This is the fundamental reason why chemotherapy is often accompanied by severe side effects such as bone marrow suppression, nausea, vomiting, and hair loss. Its therapeutic window (the gap between effective and toxic doses) is very narrow.
The advancement of medicine is essentially a continuous pursuit of “precision.” We yearn to find a method to deliver powerful “ammunition” (cytotoxic drugs) precisely to the “enemy territory” (tumor cells) while ensuring the safety of the “civilian areas” (normal tissues). This concept is at the core of “targeted therapy.”
In this pursuit of precision, ADCs have emerged in an extremely clever way. They are not entirely new drugs but rather an intelligent “composite.” They perfectly combine two types of weapons we are already familiar with—monoclonal antibodies (biologics, akin to a high-precision GPS navigation system) and small molecule chemotherapeutics (cytotoxic payloads, like powerful bombs)—through a special linker. This design is reminiscent of the “Trojan Horse” from Greek mythology, disguising lethal power beneath a highly targeted antibody shell, infiltrating tumor cells, and then releasing it to deliver a fatal blow.
The review we are about to explore paints a grand blueprint for this field. It not only reviews the century-long journey of ADCs from concept to clinic but also analyzes their hot research and market status, while profoundly pointing out the challenges they face and the vast future beyond cancer treatment. Now, let us use this review as a starting point, armed with the knowledge we have learned in class, to embark on this exploration of the “magic bullet.”
2. Core Content Interpretation: A Panoramic Scan of the ADC Field
The core of this review article can be summarized in four parts: The Glorious History and Market Status of ADCs, The Ingenious “Trinity” Structure and Mechanism of Action, The Challenges and Limitations Behind Success, and The Imaginative Future Prospects.
1. The “Past and Present” of ADCs and the Market Boom
The article begins by depicting the vigorous development of the ADC field with data. In the past three years, the number of related publications (journals and patents) has increased by 30%, with the number of patents surpassing that of journals, indicating a large-scale transition of basic research to clinical applications and commercial products. The United States, China, and Japan are the leaders in this field. The capital market is equally enthusiastic, with private investments sharply increasing since 2018, and the global market size is expected to double within a decade.
This is backed by a century-long exploration journey. We can outline this history with a timeline:
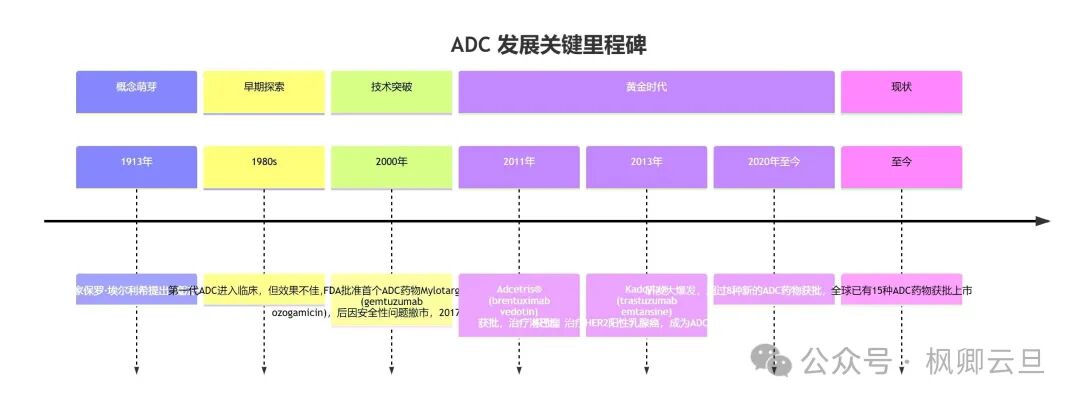
From this timeline, it is evident that ADCs did not achieve success overnight but underwent a long process of technological iteration and profound reflection on failures. Notably, the successes of Adcetris® and Kadcyla® truly ignited the entire field, proving the feasibility and immense potential of the ADC strategy.
2. The Ingenious “Trinity” Structure and “Trojan Horse” Mechanism of Action
This is the core of ADC technology and the foundation for understanding all its advantages and challenges. The article vividly compares it to a “Trojan Horse,” with its mechanism of action broken down into several key steps:
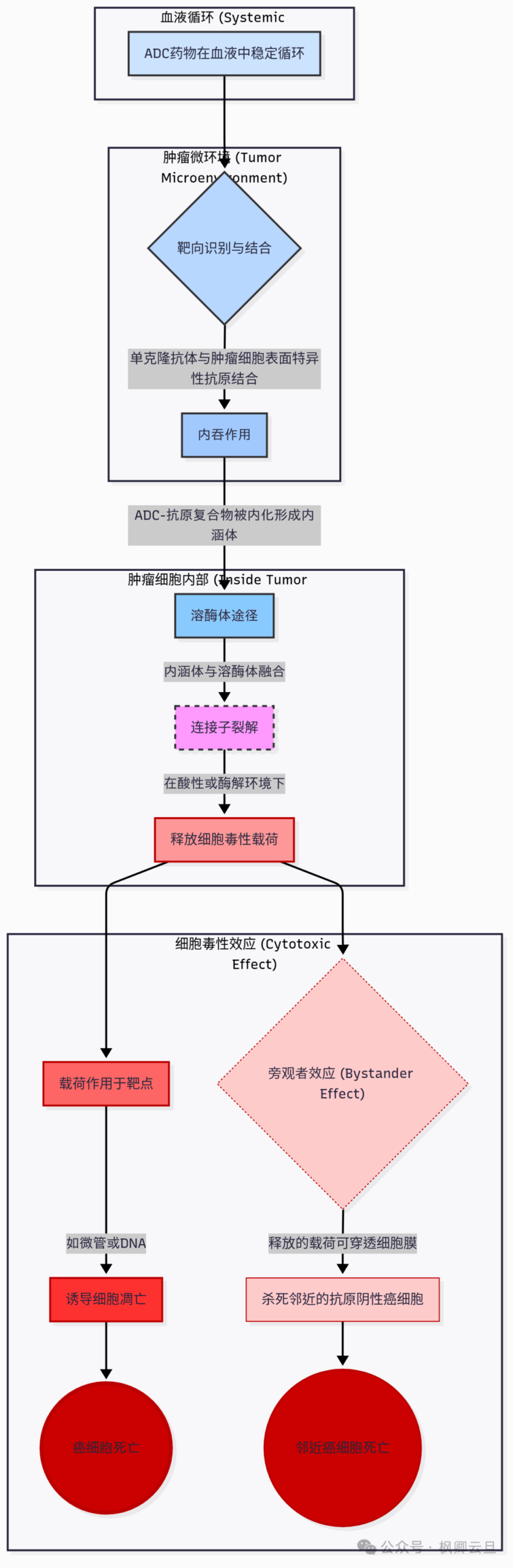
This process perfectly illustrates the “trinity” design philosophy of ADCs:
- Monoclonal Antibody (mAb): Navigation System. Its task is to specifically recognize and bind to antigens that are highly expressed on the surface of cancer cells but are lowly expressed or not expressed at all on normal cells (such as HER2, TROP2, etc.). This is the first step to achieving “precision.”
- Cytotoxic Payload: Warhead. Typically, these are highly potent chemotherapeutic agents whose toxicity is 100 to 1000 times greater than traditional chemotherapeutics. If administered systemically, they would be lethal. However, through ADC delivery, they are “captured” until they reach their destination.
- Linker: Key Bridge and Trigger. The design of the linker is highly technical. It must meet two seemingly contradictory requirements: remain absolutely stable in the bloodstream to prevent the “warhead” from prematurely detaching and causing systemic toxicity; and once the ADC is internalized into the specific environment of cancer cells (such as the acidic environment of lysosomes or protease environment), it must be precisely cleaved to release the “warhead.”
If any one of these components fails, the entire ADC design will be compromised.
3. Challenges and Limitations Behind Success
The article also objectively points out four core challenges faced in ADC development:
- Complexity and High Cost of Production: The production of ADCs involves multiple complex steps, including antibody production, drug synthesis, and conjugation reactions, with extremely high process control requirements, leading to high costs and limiting accessibility.
- Target Antigen Selection Dilemma: An ideal target antigen should be “tumor-specific.” However, in reality, many antigens are also expressed at low levels in normal tissues, which may lead to “on-target, off-tumor toxicity.” Additionally, the heterogeneity within tumors (not all cancer cells express the same antigen) can also affect efficacy.
- The Art of Balancing Cytotoxic Payloads: The selection of payloads needs to find a perfect balance between “highly effective killing” and “controllability.” If too weak, it cannot kill cancer cells; if too strong, even a small leak can cause significant toxicity.
- Development of Resistance: This is a common enemy for all cancer therapies. Cancer cells can resist ADC attacks through various mechanisms, such as downregulating target antigen expression, increasing drug efflux pumps (like pumps that expel drugs from cells), and altering lysosomal function.
4. Imaginative Future Prospects: Beyond Cancer
Despite numerous challenges, the future of ADCs remains bright. The article points out several exciting directions:
- Combination Therapy: Combining ADCs with immunotherapies (such as PD-1 inhibitors) or other targeted drugs is expected to produce a synergistic effect of “1+1>2.” For example, the antigens released after ADC kills tumor cells can activate the immune system, which can then be enhanced by immune checkpoint inhibitors to “release the brakes” and boost immune attacks.
- Design Optimization: Researchers are developing more optimized ADCs, such as using new payloads, smarter linkers, and achieving more precise control over drug conjugation sites and quantities through antibody engineering techniques (site-specific conjugation technology).
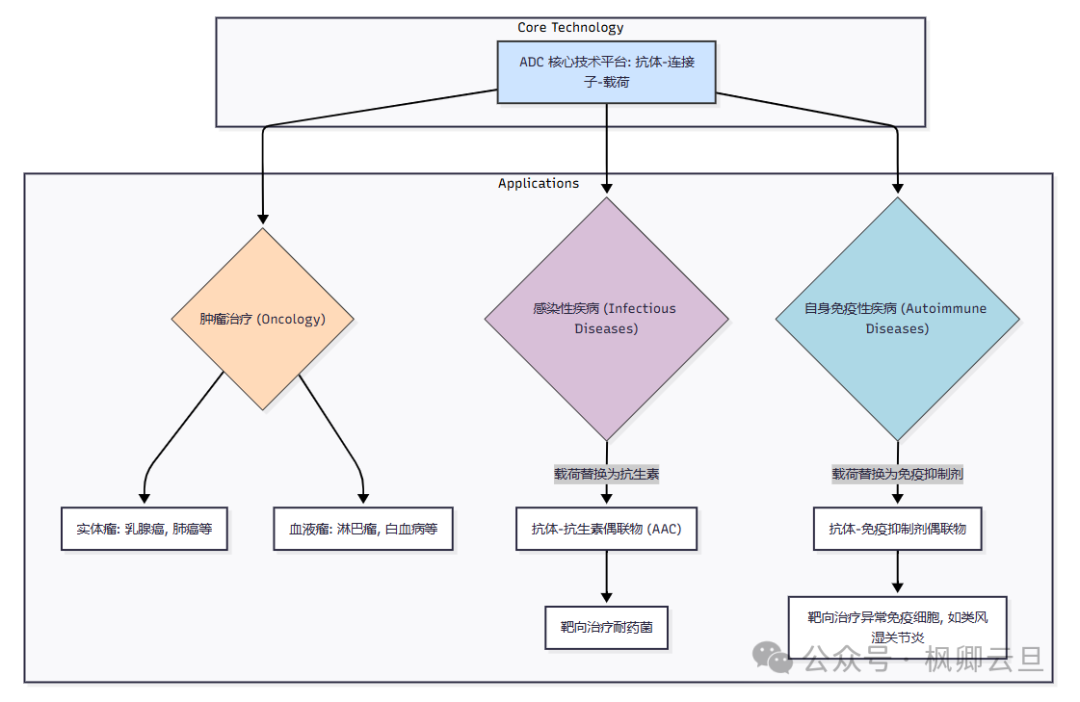
- Expansion into New Fields: The technology platform of ADCs has strong universality. The article mentions that by replacing the payload from “chemotherapeutics” to “antibiotics,” we can create Antibody-Antibiotic Conjugates (AAC) to combat resistant bacterial infections. Similarly, if the payload is changed to “immunosuppressants” (such as glucocorticoids), it can target the abnormally activated immune cells in autoimmune diseases, achieving effective anti-inflammatory effects while avoiding the side effects of systemic steroid use.
3. Learning Perspective from Medical Courses: Integrating ADC Knowledge into Our Knowledge System
This section is the core of this article. As medical students, we should not only be satisfied with knowing “what” but also understand “why” and be able to connect it with the foundational knowledge we have learned.
1. Immunology Perspective: Antibodies—The “Eyes” and “Skeleton” of ADCs
In our immunology courses, we learned about the structure and function of antibodies. A typical IgG antibody consists of two heavy chains and two light chains, divided into Fab (antigen-binding) and Fc (effector) regions.
- Fab Region and Targeting: The targeting ability of ADCs relies on the specific binding capacity of the Fab region to antigens. Concepts we learned in class, such as “epitopes” and “affinity,” directly determine whether ADCs can “find the right door.” The selection of antibodies is crucial; they need to recognize human proteins, so they must undergo “humanization” to avoid our bodies producing antibodies against this “navigation system” (i.e., anti-drug antibodies, ADA).
- Fc Region and Pharmacokinetics: The Fc region determines the half-life of the antibody in the body. By binding to the neonatal Fc receptor (FcRn), IgG antibodies can avoid rapid degradation, allowing them to circulate in the bloodstream for weeks. This grants ADCs long-lasting properties but also means that once side effects occur, they may persist for a long time. This is a typical PK/PD consideration in pharmacology.
- Consensus in the Medical Community: The concept of antibodies as targeting tools is already a consensus. The requirements for ADCs regarding antibodies, such as high affinity, low immunogenicity, and effective internalization capability, are current research hotspots in the field of antibody engineering.
2. Pharmacology Perspective: Payloads, Linkers, and the Reshaping of the “Therapeutic Window”
Pharmacology is another key to understanding ADCs.
- Cytotoxic Payloads and Mechanisms of Action: The payloads used in ADCs, such as Auristatins and Maytansinoids, are potent microtubule inhibitors. We have learned about traditional chemotherapeutics like paclitaxel and vincristine in pharmacology, which also act on microtubules. However, the potency of ADC payloads is significantly greater. Other payloads, such as Calicheamicin, are DNA damaging agents. These knowledge points can directly correspond to the content of our chemotherapy drug chapters.
- Linkers and Drug Release Kinetics: The design of linkers is a typical issue in medicinal chemistry and pharmacokinetics.
- Cleavable Linkers: Such as pH-sensitive hydrazone bonds or peptides that can be cleaved by lysosomal proteases (like cathepsin B). Their design cleverly utilizes the differences between the internal environment of tumor cells and the blood environment.
- Non-cleavable Linkers: These linkers are very stable, and the drug molecules linked to individual amino acids are only released when the entire antibody is completely degraded into amino acids in the lysosome. Drugs released in this manner are usually hydrophilic and less able to penetrate cell membranes, thus having a weaker bystander effect but higher specificity.
- Revolution of the Therapeutic Window: A core concept in pharmacology is the therapeutic index (TI), which is the ratio of the dose that produces toxic effects to the dose that produces therapeutic effects. Traditional chemotherapeutics have a low TI. ADCs, through targeted delivery, greatly reduce the effective drug concentration in systemic circulation while achieving high drug accumulation at the tumor site. This dramatically broadens the therapeutic window of highly toxic drugs, allowing many molecules that were previously too toxic to be developed to have a chance at “rebirth.” This is one of ADCs’ most profound contributions to pharmacology.
- Frontier Research: How to design linkers that can be cleaved under the unique matrix metalloproteinases (MMP) in the tumor microenvironment? How to develop new payloads with novel mechanisms of action to overcome resistance? These are current frontiers in pharmacology and medicinal chemistry.
3. Oncology and Pathology Perspective: From Target Selection to Resistance Mechanisms
- Target (Antigen) Selection: In oncology, we learn about various cancer driver genes and markers, such as HER2, ER, and PR in breast cancer. The selection of ADC targets is closely related to this. A good ADC target needs to meet:
- High expression on tumor cell surfaces, with low or no expression in normal tissues.
- Effective internalization after antibody binding.
- Relatively uniform expression to avoid “missed targets” due to tumor heterogeneity. Pathologists detect the expression levels of these targets through immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH), directly guiding the clinical use of ADC drugs (e.g., Kadcyla® for HER2-positive patients). This is a model of integrated “diagnosis-treatment” in precision medicine.
- Loss of Target: Tumor cells downregulate or mutate the target antigen, causing ADCs to “lose their way.”
- Endocytosis/Transport Barriers: The pathways for cells to internalize ADCs are blocked, or lysosomal function is abnormal, preventing the “Trojan Horse” from entering or opening.
- Drug Efflux: ABC transporters (like MDR1/P-gp) are overactivated, pumping the payload molecules out of the cells like a water pump.
4. Strategic Significance and Future Challenges of ADCs in Medical Science
Stepping back from specific molecules and mechanisms, what does the rise of ADCs mean for the entire field of medical science?
1. ADCs: A Bridge Connecting Biologics and Chemotherapeutics, the Culmination of Precision Medicine
ADCs perfectly integrate two of the most mainstream drug forms: large molecule monoclonal antibodies (biologics) and small molecule cytotoxic drugs (chemotherapeutics). They draw on the targeting of the former and the high killing power of the latter, compensating for the former’s lack of potency and the latter’s poor targeting. It can be said that ADCs are a product of the deep integration of modern biotechnology, chemical synthesis technology, and clinical medical needs, representing one of the most outstanding examples of precision medicine.
2. Transformation of R&D Models: From “Solo Operations” to “Multidisciplinary Collaboration”
The development of ADCs is extremely complex, requiring a team to be proficient in:
- Antibody Engineering: Screening, modifying, and producing high-affinity, low-immunogenicity antibodies.
- Medicinal Chemistry: Synthesizing highly potent and physically-chemically suitable cytotoxic payloads.
- Linker Chemistry: Designing and synthesizing linkers that can stably exist or be precisely cleaved under specific conditions.
- Bioconjugation Technology: Connecting antibodies, linkers, and payloads in precise stoichiometric ratios (DAR, Drug-to-Antibody Ratio).
- Preclinical and Clinical Research: Evaluating efficacy, toxicity, pharmacokinetics, and designing scientific clinical trials. This has driven the pharmaceutical industry to shift from traditional “chemically driven” or “biologically driven” models to a highly integrated, multidisciplinary collaborative R&D model.
3. Challenges and Considerations in Clinical Applications
- Management of Toxic Side Effects: Although the design of ADCs aims to reduce toxicity and enhance efficacy, they are not without toxicity. Common side effects include hematological toxicity (such as neutropenia), hepatotoxicity, and some specific “off-target” toxicities, such as ocular toxicity and interstitial lung disease. As future clinicians, we need to learn how to recognize and manage the unique adverse reactions brought by these new drugs.
- Precise Patient Selection: How to more accurately define the “positive” standards for target antigens? Are there subjective differences in interpreting IHC test results? Are there more quantitative detection methods than IHC (such as mass cytometry)? These are key factors determining whether patients can benefit from ADC treatment and pose new demands on our clinical diagnostic capabilities.
- Economic Toxicity and Drug Accessibility: The high R&D costs of ADCs will ultimately be reflected in their prices. How to balance drug innovation, corporate profits, and patient affordability is a global healthcare economics challenge.
5. Conclusion: The Reachable “Magic Bullet” and Endless Medical Exploration
Returning to the initial question: Are ADCs the “magic bullet” that Paul Ehrlich dreamed of?
In a sense, yes. ADCs achieve targeted strikes against cancer cells with unprecedented precision and efficacy, ushering cancer treatment into a new era. They have successfully changed the treatment landscape for various malignancies, bringing new hope to countless patients.
However, from another perspective, we are still distant from the perfect “magic bullet.” Challenges such as resistance, toxic side effects, and tumor heterogeneity remain. The story of ADCs is far from over; it is advancing towards smarter, safer, and broader application fields. The next generation of ADCs may feature more optimized antibodies, linkers that can be activated more specifically by the tumor microenvironment, novel mechanisms of action for payloads, and even the ability to carry two different payloads to address resistance. Its applications will also expand from tumors to infections, autoimmune diseases, and other difficult-to-treat conditions.
As a medical student, it is a privilege to be in this rapidly evolving era of biomedicine. The story of ADCs teaches us that every major breakthrough in medicine stems from a profound understanding and clever application of basic sciences (immunology, pharmacology, molecular biology). Every seemingly dull knowledge point we learn in class today may become the spark that ignites a therapeutic revolution in the future.
Therefore, let us continue to maintain curiosity and a thirst for knowledge, solidly build our foundations, and keep pace with cutting-edge developments. Because the future “magic bullet” may very well be created by our generation, based on a deep understanding of the essence of diseases.