Click to follow Xiaobai Learning MedicineIntroduction: Since the approval of the first ADC drug Mylotarg® (Gemtuzumab Ozogamicin) in 2000, the number of ADC drugs has exploded, with 14 types of ADCs approved for market, and hundreds of ADC drugs undergoing clinical trials for various tumor indications. 
While ADCs are effective, their clinical development and application still face significant challenges!
Whoever can provide targeted solutions to these challenges may represent the future direction of ADC drug updates and iterations.
01Obstacles in the Tumor Microenvironment
A key challenge affecting the efficacy of ADCs is the delivery efficiency to the tumor site. It is estimated that only 0.1% of the total dose of ADCs is delivered to the tumor site before cellular internalization, which is a dismal efficiency.
This is attributed to the large molecular weight of ADC antibodies (∼150 kDa), the heterogeneity of tumor-associated antigen (TAA) expression, and the physical and biological barriers of the tumor microenvironment.
These barriers include the tumor microenvironment (TME) and binding site barriers (BSB) that impose physical isolation on the drug and are related to antibody affinity.

For example, high-affinity antibodies administered at sub-saturating levels exhibit heterogeneity in their distribution within the tumor. For ADCs, this can be addressed by co-administering ADCs with unconjugated parent antibodies to saturate available binding sites and overcome BSB, which also minimizes the impact on ADC toxicity.
Combination therapy with anti-angiogenic drugs has also been explored to improve the intratumoral distribution of ADCs.
Additionally, the route of administration can alter the PK/PD of ADCs; intratumoral and subcutaneous administration routes have shown promise in enhancing efficacy and reducing dosage.
However, intratumoral injection requires invasive procedures, making it difficult to achieve injection precision at the tumor margins and limiting its applicability to metastatic diseases.
Subcutaneous injection is the preferred route for antibody therapies, but it is less effective for ADCs. Frequent injection site reactions hinder the clinical application of ADCs via subcutaneous injection, and subcutaneous administration may exclude the use of certain effective payloads (such as MMAE).
02Resistance is Very Difficult to Manage
Like other antitumor drugs, patients receiving ADC therapy may also develop resistance. The mechanisms are related to the parent antibody, linker composition, and cytotoxic payload.
First, ADC therapy may downregulate and reduce tumor antigen expression, leading to decreased binding between the antibody and antigen, thus reducing overall therapeutic efficacy. Additionally, the heterogeneity of tumor antigen expression is a significant contributor to ADC resistance.
Some tumor antigens shed into the tumor microenvironment can act as decoys to interfere with ADC binding.
Strategies to overcome tumor antigen-related ADC resistance include designing multispecific ADCs targeting multiple antigens, antibody engineering (Fc engineering), and combining ADCs with immune checkpoint inhibitors to effectively kill tumor cells.
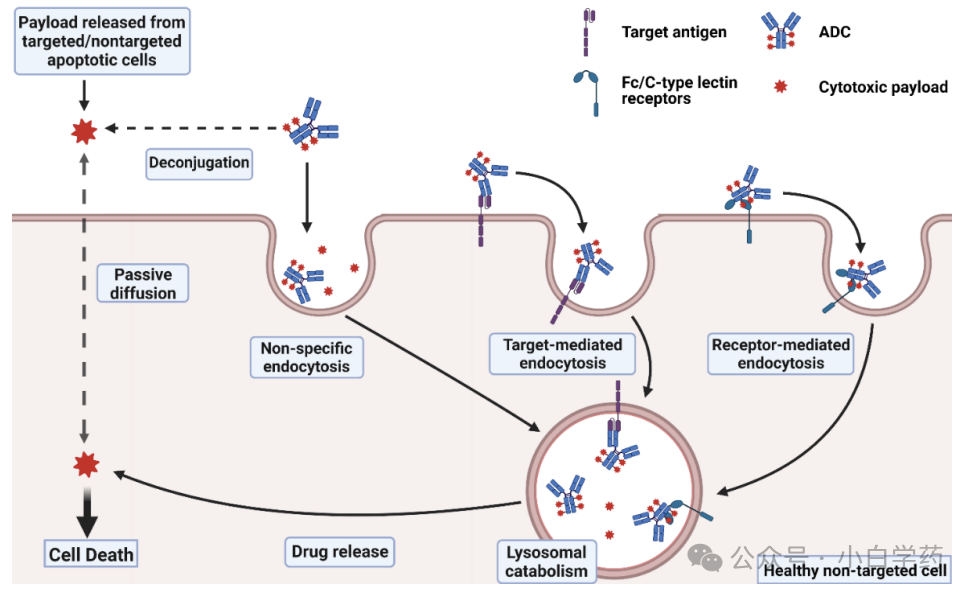
Moreover, most ADCs have small molecule cytotoxic payloads that can exert bystander effects in tumor cells with low TAA expression.

Second, impaired internalization due to abnormal endocytosis can also limit ADC cellular uptake, leading to resistance.
Using non-cleavable linker ADCs relies on the antibody’s endosomal degradation and the lysosomal degradation of cleavable linkers to release the active payload. Changes in lysosomal function in tumor cells can prevent the release of the active payload, reducing ADC efficacy.
Third, efflux and metabolic reprogramming can also cause ADC resistance. Cytotoxic payloads are sensitive to efflux transporters (p-glycoprotein, BCRP), which are constitutively expressed in tumor cells, thus reducing the effective intracellular levels of cytotoxic drugs.
In addition to efflux, changes in tumor cell metabolism may lead to the degradation of cytotoxic payloads before they exert their therapeutic effects.
03ADME Studies are Quite Challenging
Absorption, Distribution, Metabolism, and Excretion (ADME) characteristics of ADCs are key determinants of their clinical safety and efficacy.
The parent antibody significantly influences the PK of ADC drugs, including prolonged circulation half-life, low volume of distribution, proteolytic degradation, and slow clearance.
Despite certain advantages, the development of ADCs still faces significant challenges from a PK perspective due to molecular heterogeneity.

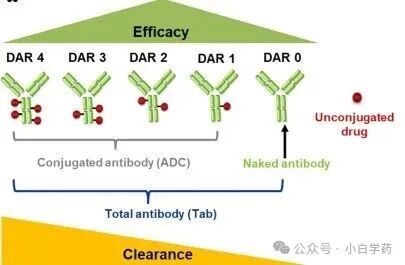
ADCs consist of two pharmacologically distinct parts— the antibody and the cytotoxic drug — which need to be evaluated separately for their PK characteristics as well as for the overall PK of the ADC.
Different drug-to-antibody ratios (DAR) or the heterogeneity of conjugation sites can lead to variations in drug payload distribution, and the chemical properties of the linker (stability and release rate) can significantly alter ADC PK characteristics.
Studies have shown that ADCs with high DAR (e.g., DAR = 8) exhibit rapid plasma clearance, significantly altering the PK characteristics of ADCs. This is primarily due to the increased hydrophobicity and aggregation tendency of high DAR, which promotes accelerated clearance.
In contrast, low DAR ADCs tend to have longer circulation times and more favorable PK characteristics.
These data indicate that DAR affects ADC PK, thus rational design of DAR is an important pathway to optimize the therapeutic index.
The low intratumoral accumulation of ADCs is a pharmacokinetic bottleneck faced by ADCs, limiting the amount of active payload reaching the target site. Imaging-guided biodistribution studies using radiolabeled ADCs have confirmed that tumor accumulation levels are approximately 0.1% of the total administered dose, with most ADCs sequestered by the liver and spleen.
These findings highlight the need for drug design to achieve tumor penetration, which includes improving delivery, payload, linker design, and DAR optimization.
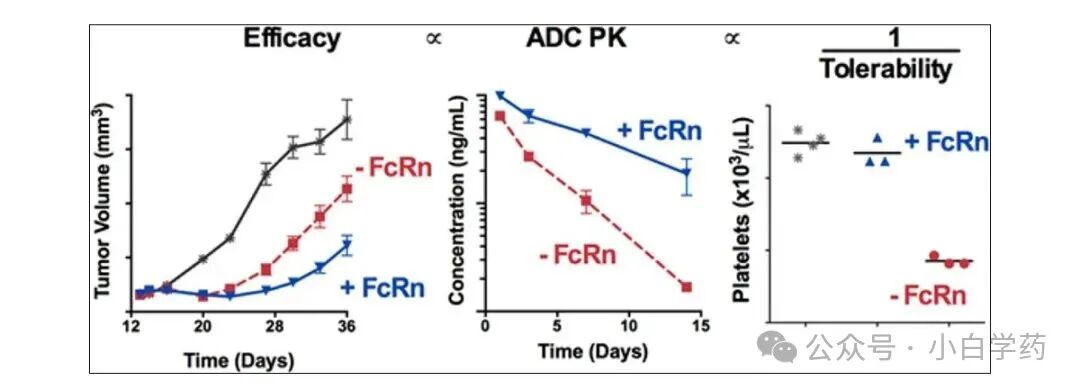
The parent antibody of ADCs can bind to FcRn, with up to approximately 65% of the FcRn binding ADCs being recycled. Given the role of FcRn in altering ADC PK, sufficient research is needed to evaluate the impact of FcRn binding to ADCs under formulation and physiologically relevant conditions.
When antibodies are conjugated with payloads of different chemical compositions, the physicochemical properties of the antibody change, which can also affect the binding of ADCs to FcRn and the overall pharmacokinetic characteristics. Therefore, the impact of DAR on FcRn interactions should also be evaluated during early development.
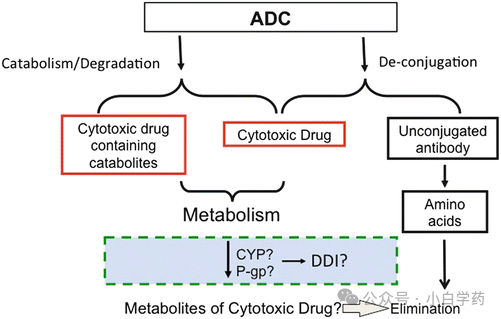
The elimination pathways of ADCs include decoupling and degradation through metabolic breakdown or proteolytic degradation, which may occur in the lysosomal compartment or intracellularly.
ADCs are internalized via endocytosis and transported through lysosomes. The metabolic breakdown of the antibody portion leads to the formation of antibody fragments.
The cytotoxic drug portion of ADCs forms metabolites that may diffuse to adjacent cells (bystander effect), and are subsequently metabolized by cytochrome P450 enzymes or effluxed by transporters (e.g., p-glycoprotein) for renal and biliary excretion.
Overall, the PK characteristics of ADCs are primarily driven by the parent antibody, while the toxicological characteristics are determined by the choice of linker and the pharmacology of the cytotoxic payload.
Analyzing the elimination pathways of ADCs is crucial for understanding dose-limiting toxicities and designing appropriate dosing regimens.
04The Toxicity of Drugs Cannot Be Ignored
First is immunogenicity. Most ADCs contain humanized or human antibodies and small molecule drugs, which increase the potential for immunogenicity due to their semi-antigenic structures compared to monoclonal antibodies.
Anti-drug antibodies (ADA) epitopes can target various domains of the ADC structure, including epitopes, linkers, and small molecules.
Among these, the formation of ADA-ADC immune complexes can lead to off-target toxicity due to non-immune cell internalization, making the ADA formed against the cytotoxic payload particularly concerning.
During the design process of ADCs, it is essential to conduct immunogenicity risk assessments for various ADCs to mitigate potential adverse events arising from ADA responses.
In addition to immunogenicity, ADC drugs also have toxic side effects characteristic of the drugs themselves. The marketed drug Gemtuzumab ozogamicin (Mylotarg®) was initially used for acute myeloid leukemia but was withdrawn from the global market in 2010 due to reports of venous occlusive disease.
Several factors can influence the adverse events associated with ADC administration. These include (i) cytotoxic payloads, (ii) linkers, and (iii) Fc-mediated ADC internalization-related toxicity.
Premature release of cytotoxic payloads in circulation can lead to off-target toxicity events of small molecule cytotoxic payloads. Additionally, the antibody Fc may interact with cell surface FcγR expressed in tissues, leading to its internalization and antibody-induced toxicity.
 05Designing Doses is Very Difficult
05Designing Doses is Very Difficult
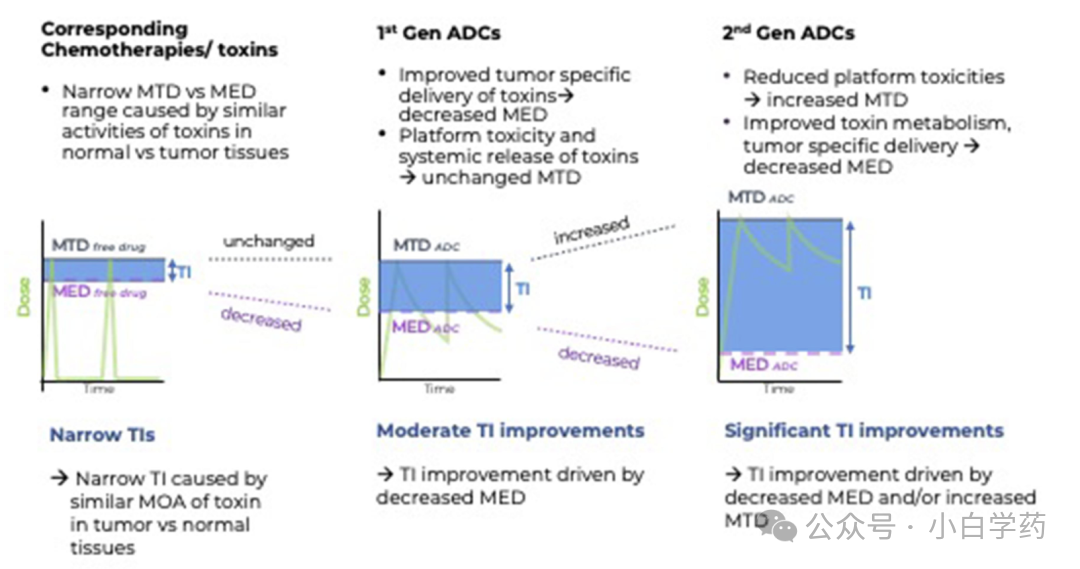
Rational dose regimen design provides key means for ADC drug product design and addressing dose-limiting toxicities.
The unique structure of ADCs presents challenges in clinical administration due to the narrow therapeutic window caused by systemic toxicity. Therefore, dose regimen design is a complex process that requires careful optimization while minimizing the occurrence of grade 3/4 toxic adverse events.
The FDA recommends testing various dose levels in early development to determine the relationship between ADC exposure, its active components, and overall safety and efficacy.
In later development, dosing strategies can be refined based on exposure-response relationships established in early clinical trials and stratified according to patient subtypes. Additionally, clinical (patient) and non-clinical (product) parameters, pharmacodynamic biomarker responses, exposure-response relationships, and target engagement data should be integrated.
In summary, whoever has a superior therapeutic index for their product will win the market in the future.
Click to follow Xiaobai Learning Medicine
Recommended Reading
Antibody Drug Development | From “Mouse” to “Human”, from a Trillion Market to Precision Medicine, the Past, Present, and Future of Antibody Drugs (Part 1) |
Antibody Drug Development | The “Fourth Generation Magic Bullet” is Ready: Understanding the 7 Major Breakthroughs in Antibody Drugs (Part 2) |
Antibody Drug Development (Part 3) | Antibodies: Precise Guardians of the Immune System |
Antibody Drug Development | Indispensable Antibodies: A Comprehensive Interpretation from Immune Defense to Medical Applications (Part 4) |
Antibody Drug Development | Antibodies: A Perfect Symphony of Structure and Genes (Part 5) |
Antibody Drug Development | One Key Opens One Lock? Far Beyond Imagination! Unveiling the Immunological Foundation of the Trillion Market of Antibody Drugs (Part 6) |
Antibody Drug Development | From “Street Mouse” to “Drug King” Legend: The Ultimate Camouflage of Antibody Drugs (Part 7) |
Antibody Drug Development | The Dual Evolution of Antibody Drugs: Fusion Proteins for “Precision Guidance” and CAR-T Cells for “Live Pursuit” (Part 8) |
Innovative Cancer Dual Heroes: Breakthroughs and Prospects of CAR-NK Cells and ADC Drugs |
Antibody Drug Development | Killing Two Birds with One Stone: How Dual Antibody Drugs Become New Weapons Against Cancer? (Part 9) |
New Generation Cancer Weapons: A Comprehensive Analysis of Trispecific Antibodies and Enhanced Antibody Technologies (Part 10) |
Disclaimer:This public account does not constitute any investment opinions or advice.Reprint with source indicated:Xiaobai Learning Medicine Public Account.Some content is sourced from publicly available information on the internet, used for knowledge dissemination and learning purposes, and will be deleted upon request.Due to limited expertise, if any errors occur, please feel free to point them out.