I recently read a great review that coincides with some recent advancements in ADCs, so I decided to summarize and learn from it.
ADCs are a key milestone in the evolution from traditional drugs to precision-targeted therapies.Currently, 19 ADCs have been approved globally (including 2 that have been withdrawn), and over 300 ADCs are in clinical development.From the timeline of approvals, ADC research entered a period of explosive growth after 2019, with significant acceleration in technological iterations and clinical breakthroughs.
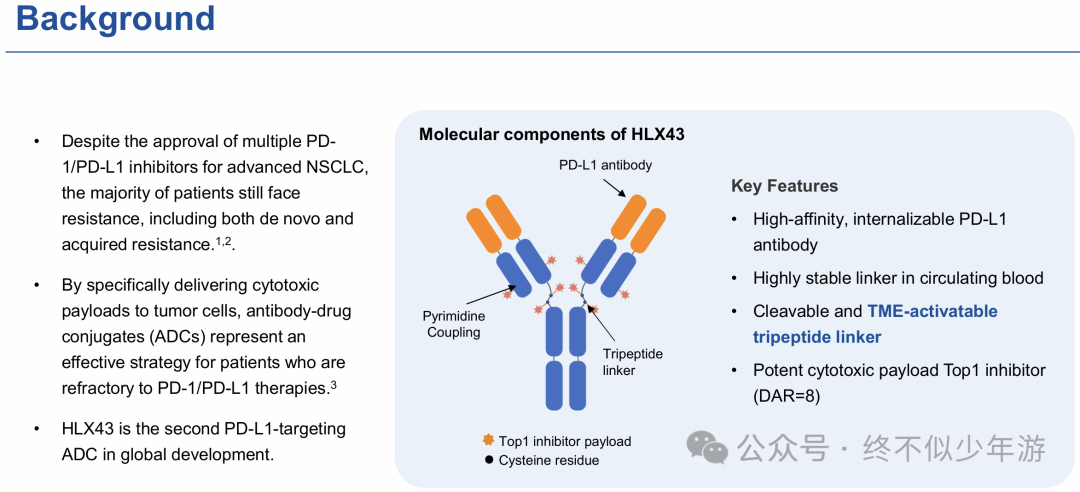
Note:Blenrep (Belantamab mafodotin) is seeking to be reintroduced, including a re-approval by the UK MHRA in April 2025 for use in combination therapy for relapsed/refractory multiple myeloma as a second-line treatment; it received EU approval in July for a combination treatment regimen for relapsed or refractory multiple myeloma; however, in the US, approval has been delayed until October 23 due to insufficient patient representation, clinical control scheme issues with SOC, and severe ocular toxicity problems. Although ADCs are widely recognized as transformative therapeutic agents, many critical questions regarding their mechanisms of action remain to be elucidated. Increasing evidence suggests that the mechanisms of ADCs are far more complex than simplified descriptions imply. For example, traditional explanations of ADCs often underestimate the role of exposure kinetics. Just as certain chemotherapeutic agents are more effective when administered via continuous infusion rather than bolus, the sustained release of ADC payloads in the circulatory system can maintain drug concentrations above the in vitro cytotoxic threshold for several days. This prolonged drug exposure may be one of the key reasons for the efficacy of ADCs. Conversely, traditional models tend to overemphasize the selective uptake of ADCs by tumors. Studies using radiolabeled antibodies have shown that typically less than 1% of the administered conjugates reach tumor cells, with the remainder distributed in normal tissues. A recent clinical outcome study further highlighted this characteristic: it found that among patients receiving T-DXd treatment, higher body fat percentage correlated with increased treatment toxicity and reduced efficacy. Furthermore, while certain toxicities are related to on-target, off-tumor uptake (such as HER2-related cardiac toxicity, TROP2-related mucositis, Nectin-4 and EGFR-related skin toxicity, and TF-related ocular toxicity), target-related adverse events rarely limit the tolerable dose of ADCs. In most cases, it is the payload-related toxicity that determines the maximum tolerated dose of ADCs, which is typically comparable to that of traditional small molecule analogs, with similar associated toxicities such as fatigue, vomiting, hair loss, blood cell reduction, and neuropathy. Revisiting the Role of Antigen Dependence and Extracellular Payload Release Increasing evidence challenges the notion that “the efficacy of ADCs strictly depends on high antigen expression and internalization processes.” There is a significant disparity in the association between target expression and ADC efficacy. For instance, T-DXd has shown clinically meaningful efficacy even in HER2-negative tumor patients, while T-DM1, which has the same antibody backbone, is only effective in HER2-high expressing tumor patients—likely because its payload lacks a bystander effect. Clinical trials of Mirvetuximab soravtansine found that high expression of folate receptor alpha (FRα) was a key factor for its efficacy in ovarian cancer, leading to its eventual approval for FRα-high expressing patients; similarly, Tisotumab vedotin was also only accelerated approved for cMet-high expressing patients. In contrast,Tisotumab vedotin clinical trials in cervical cancer showed no correlation between tissue factor (TF) expression and efficacy. Other targets exhibit similar situations: B7-H3, HER3, Nectin-4, TROP2 in solid tumors, and BCMA, CD19, CD22, CD30, CD33, CD79b in hematological malignancies, all show no clear association between expression levels and corresponding ADC efficacy. Another similar example is the recently popular PD-L1 ADC HLX43, which also showed significant efficacy in PD-L1 negative patients, whilePfizer’sSGN-PDL1V (PF-08046054) only demonstrated efficacy in PD-L1 positive patients, althoughHLX43 also had correspondingly higher toxicity. This may be related to the use of a tumor TME extracellular cleavable tripeptide linker in HLX43. 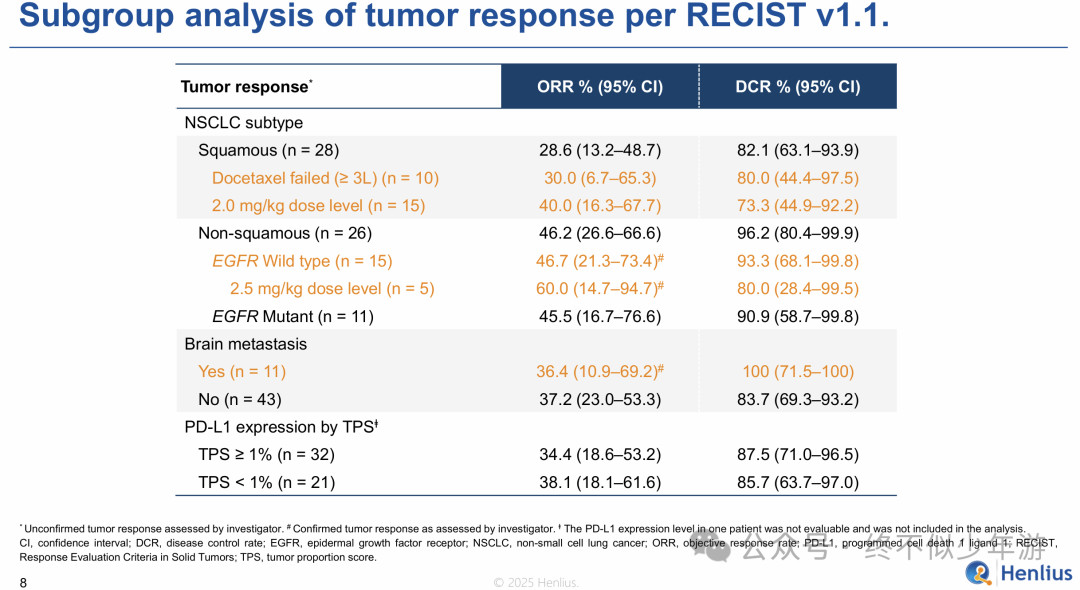
 HLX-43 2025 WCLC Results Announcement New preclinical studies may explain some of the reasons behind the aforementioned differences. Tsao et al. confirmed that T-DXd’s activity in HER2-negative breast cancer can occur independently of HER2 binding, indicating that the mechanism by which T-DXd exerts efficacy in HER2-low expressing tumors extends beyond direct targeting of the antigen. Specifically, cathepsin L, present in tumor cells and stromal cells within the tumor microenvironment, can cleave the linker of T-DXd, facilitating extracellular payload release and exerting antitumor activity—this process is independent of HER2 expression. This non-internalizing payload release differs from the traditional bystander effect (in which the drug must circulate from cancer cells to the tumor microenvironment). The discovery of cathepsin L-mediated extracellular payload release may be coincidental. The GGFG linker of T-DXd was initially designed to be cleaved by lysosomal proteases within cells. Other common proteases that can cleave linkers (such as valine-citrulline, valine-alanine) are also substrates for various proteases, including cathepsin L, and thus may also undergo similar extracellular cleavage. Previously mentioned in“PYX-201: Can Non-internalizing ADCs Be This Simple?” was the non-internalizing ADC PYX-201, which chose a conventional VC linker.These findings provide new impetus for the following research: 1) exploring the contribution of existing linkers to ADC efficacy, 2) developing novel tumor-selective linkers, and 3) assessing the feasibility of using protease expression as potential biomarkers for patient selection. Currently, research is actively underway to optimize the predictive efficacy of existing biomarkers. Standard immunohistochemistry (IHC) relies on manually categorizing samples into discrete categories (such as HER2 0, 1+, 2+, or 3+), which is overly broad, lacks specificity, and is subjective. New methods combine sensitive molecular detection with quantitative analysis to determine predictive expression thresholds for targets, including mRNA detection, quantitative immunofluorescence, and reverse-phase protein array technologies. Some methods also incorporate pathway activation indicators (such as phosphorylation levels) or the expression levels of intracellular transport genes. Although most studies focus on HER2, the FDA recently granted “breakthrough device designation” for a TROP2 detection platform, which is a computational pathology companion diagnostic tool. When multiple ADCs are available, these quantitative methods are expected to better select patients and inform treatment sequence decisions (https://www.roche.com/media/releases/med-cor-2025-04-29).Antibody Component’s Immunomodulatory Role The antibody backbone of ADCs is another area of increasing attention. Traditional models focus on target specificity and endocytosis processes but underestimate the immune effector functions of the antibody backbone, such as antibody-dependent cellular phagocytosis (ADCP) and antibody-dependent cellular cytotoxicity (ADCC). Previous studies have shown that both T-DM1 and T-DXd retain the known mechanisms of action of unconjugated (naked) trastuzumab. ADCs carrying other payloads have also shown superior efficacy in immunocompetent mice compared to nude mice, suggesting that T cells may be involved in the antitumor activity of ADCs. Upregulation of the CD47 signaling pathway diminishes this immune-related activity, but co-administration of CD47 checkpoint inhibitors can restore it. Other preclinical studies have found that payload-induced immunogenic cell death (ICD) by ADCs can make tumors more sensitive to checkpoint inhibitors. In clinical applications,Enfortumab vedotin (EV) in combination with pembrolizumab has been approved for first-line treatment of urothelial carcinoma. Recent studies of Sacituzumab govitecan (SG) combined with pembrolizumab (pembrolizumab) for TNBC and Disitamab vedotin combined with Toripalimab for gastric cancer have yielded positive results, supporting the exploration of similar combination regimens across different tumor types. Meanwhile, certain toxicities of ADCs may stem from Fc-mediated interactions. For instance, thrombocytopenia associated with T-DM1 is related to FcγRIIa-dependent, HER2-independent impairment of platelet production. The interstitial lung disease (ILD) associated with T-DXd is also speculated to be related to interactions between Fc receptors and alveolar macrophages. Although all approved ADCs and most ADCs in clinical development retain a functionally intact Fc region, and only a few ADCs are associated with a high incidence of ILD, an increasing number of ADCs are being engineered to reduce or eliminate Fc receptor interactions to mitigate potential immune-related adverse events. However, the efficacy of these modifications remains speculative—there are currently no clinical data (even cross-trial data) available to compare ADCs that differ only in Fc receptor binding characteristics. Therefore, caution is warranted when designing structural modifications that may alter Fc function (such as Fc mutations, site-specific conjugation, or glycoengineering), weighing the potential benefits and drawbacks of silencing, retaining, or enhancing the Fc region.
HLX-43 2025 WCLC Results Announcement New preclinical studies may explain some of the reasons behind the aforementioned differences. Tsao et al. confirmed that T-DXd’s activity in HER2-negative breast cancer can occur independently of HER2 binding, indicating that the mechanism by which T-DXd exerts efficacy in HER2-low expressing tumors extends beyond direct targeting of the antigen. Specifically, cathepsin L, present in tumor cells and stromal cells within the tumor microenvironment, can cleave the linker of T-DXd, facilitating extracellular payload release and exerting antitumor activity—this process is independent of HER2 expression. This non-internalizing payload release differs from the traditional bystander effect (in which the drug must circulate from cancer cells to the tumor microenvironment). The discovery of cathepsin L-mediated extracellular payload release may be coincidental. The GGFG linker of T-DXd was initially designed to be cleaved by lysosomal proteases within cells. Other common proteases that can cleave linkers (such as valine-citrulline, valine-alanine) are also substrates for various proteases, including cathepsin L, and thus may also undergo similar extracellular cleavage. Previously mentioned in“PYX-201: Can Non-internalizing ADCs Be This Simple?” was the non-internalizing ADC PYX-201, which chose a conventional VC linker.These findings provide new impetus for the following research: 1) exploring the contribution of existing linkers to ADC efficacy, 2) developing novel tumor-selective linkers, and 3) assessing the feasibility of using protease expression as potential biomarkers for patient selection. Currently, research is actively underway to optimize the predictive efficacy of existing biomarkers. Standard immunohistochemistry (IHC) relies on manually categorizing samples into discrete categories (such as HER2 0, 1+, 2+, or 3+), which is overly broad, lacks specificity, and is subjective. New methods combine sensitive molecular detection with quantitative analysis to determine predictive expression thresholds for targets, including mRNA detection, quantitative immunofluorescence, and reverse-phase protein array technologies. Some methods also incorporate pathway activation indicators (such as phosphorylation levels) or the expression levels of intracellular transport genes. Although most studies focus on HER2, the FDA recently granted “breakthrough device designation” for a TROP2 detection platform, which is a computational pathology companion diagnostic tool. When multiple ADCs are available, these quantitative methods are expected to better select patients and inform treatment sequence decisions (https://www.roche.com/media/releases/med-cor-2025-04-29).Antibody Component’s Immunomodulatory Role The antibody backbone of ADCs is another area of increasing attention. Traditional models focus on target specificity and endocytosis processes but underestimate the immune effector functions of the antibody backbone, such as antibody-dependent cellular phagocytosis (ADCP) and antibody-dependent cellular cytotoxicity (ADCC). Previous studies have shown that both T-DM1 and T-DXd retain the known mechanisms of action of unconjugated (naked) trastuzumab. ADCs carrying other payloads have also shown superior efficacy in immunocompetent mice compared to nude mice, suggesting that T cells may be involved in the antitumor activity of ADCs. Upregulation of the CD47 signaling pathway diminishes this immune-related activity, but co-administration of CD47 checkpoint inhibitors can restore it. Other preclinical studies have found that payload-induced immunogenic cell death (ICD) by ADCs can make tumors more sensitive to checkpoint inhibitors. In clinical applications,Enfortumab vedotin (EV) in combination with pembrolizumab has been approved for first-line treatment of urothelial carcinoma. Recent studies of Sacituzumab govitecan (SG) combined with pembrolizumab (pembrolizumab) for TNBC and Disitamab vedotin combined with Toripalimab for gastric cancer have yielded positive results, supporting the exploration of similar combination regimens across different tumor types. Meanwhile, certain toxicities of ADCs may stem from Fc-mediated interactions. For instance, thrombocytopenia associated with T-DM1 is related to FcγRIIa-dependent, HER2-independent impairment of platelet production. The interstitial lung disease (ILD) associated with T-DXd is also speculated to be related to interactions between Fc receptors and alveolar macrophages. Although all approved ADCs and most ADCs in clinical development retain a functionally intact Fc region, and only a few ADCs are associated with a high incidence of ILD, an increasing number of ADCs are being engineered to reduce or eliminate Fc receptor interactions to mitigate potential immune-related adverse events. However, the efficacy of these modifications remains speculative—there are currently no clinical data (even cross-trial data) available to compare ADCs that differ only in Fc receptor binding characteristics. Therefore, caution is warranted when designing structural modifications that may alter Fc function (such as Fc mutations, site-specific conjugation, or glycoengineering), weighing the potential benefits and drawbacks of silencing, retaining, or enhancing the Fc region. Resistance, Treatment Sequence, and Payload Diversification Discussions about ADC resistance often focus on its unique resistance mechanisms, such as the loss of target antigen expression following ADC treatment. In ADCs targeting CD30, CD33, Nectin-4, and HER2, a decrease in target antigen expression has been observed. Similarly, target antigens often undergo mutations, such as truncation of the HER2 extracellular domain, splice variants of CD33 that lose target epitopes, and missense mutations in TROP2 that affect membrane localization. In addition, there are other non-antigen-dependent ADC-specific resistance mechanisms, including reduced lysosomal proteolytic activity and abnormal lysosomal membrane transport function. Recent research data has focused on payload-related resistance. In mBC, Abelman et al. confirmed that the emergence of TOP1 mutations leads to cross-resistance to multiple TOP1i payloads. Jacot et al. also detected TOP1 mutations in some patients receiving T-DXd treatment. Other preclinical studies and recent clinical data from the DESTINY-Breast02 and DESTINY-Breast03 trials support these findings: inmBC patients, efficacy can still be achieved after T-DXd treatment when subsequently using HER2-targeted small molecule drugs or antibody drugs. Other clinical evidence points to similar conclusions. A large real-world study of mBC patients after T-DXd treatment found that patients using non-TOP1i chemotherapy drugs had better outcomes compared to those using another TOP1i ADC (SG). Similarly, a retrospective analysis involving 111 metastatic breast cancer patients showed that HER2-high expressing patients receiving a second ADC with the same type of payload had shorter PFS than those receiving ADCs with different types of payloads. There are reasons to question whether this resistance dynamic applies to tumor types beyond HER2-positive cancers—HER2-positive cancers are characterized by strong oncogene dependence and abnormally high protein expression levels. Recent data indicate that payload-mediated resistance is not unique to HER2-positive cancers. Two real-world studies found thatmBC patients who received T-DXd treatment after stopping SG had shorter PFS and OS than those who had not received SG treatment. Similarly, in the prospective trial assessing Datopotamab deruxtecan, nearly all patients with efficacy had not previously received TOP1i drugs. In a smaller trial, Emiltatug legadotin, targeting B7-H4 and carrying anti-microtubule payloads, still showed activity in TNBC patients who progressed after treatment with TOP1i ADCs. Drug efflux pumps are another resistance mechanism related to payloads. Multi-omics analysis of tumor samples from 2799 breast cancer patients treated with T-DXd revealed that patients with high expression levels of the multidrug resistance protein 1 (MDR1) gene had shorter overall survival, regardless of their HER2 expression levels (high or low). Other studies have also found that patients with high expression levels of P-glycoprotein (another efflux pump associated with resistance) had poorer treatment responses. In acute myeloid leukemia (AML) patients, strong P-glycoprotein function was also associated with poor responses to Gemtuzumab ozogamicin treatment. Notably, preclinical models of urothelial carcinoma found that disrupting efflux pump function could restore sensitivity in cells resistant to ADCs. Several prospective trials are currently evaluating the efficacy of TOP1i ADCs in patients who have previously received TOP1i ADCs, including TRADE-DXd (NCT06533826), SATEEN (NCT06100874), SERIES (NCT06263543), and ENCORE (NCT06774027). These studies will help clarify the benefits of sequential ADC treatment—this issue becomes particularly critical as ADCs are increasingly used in first-line and adjuvant therapies. Beyond HER2 targets, several next-generation ADCs are in clinical trials, including multiple novel ADCs targeting Nectin-4 with different TOP1i payloads. Many patients in these trials have previously received EV treatment, providing an opportunity to compare efficacy between different payloads. Among them, early trial results of the Nectin-4-targeting TOP1i ADC SHR-A2102 showed good therapeutic activity in urothelial carcinoma patients (including those who had previously received non-TOP1i ADCs). Payloads have become a core influencing factor in ADC resistance, highlighting the need to develop more differentiated payload categories. Early ADCs primarily used microtubule inhibitors or DNA-targeting drugs as payloads. Subsequently, the variety of payloads gradually diversified, with a significant increase in the application of topoisomerase inhibitors. Next-generation payloads in development are even more diverse, including radioactive ligands, RNA polymerase inhibitors, bifunctional and molecular glue degraders, Bcl-2 family protein modulators, and immune activators. Although differentiated payloads are attractive and necessary to develop, they still require comprehensive evaluation. For example, amanitin toxins are insensitive to drug efflux pumps, but their high systemic toxicity and hydrophilicity pose challenges for their application. The failure of several new payload developments also highlights the challenges in this field: multiple immunostimulatory ADCs, including NJH395, BDC-1001, SBT6050, SBT6290, and TAK-500, have been discontinued; two conjugates targeting BCL-XL, ABBV-155 and ABBV-637, have also been paused; recently, two Degrader-antibody conjugates (DAC) drugs: ABBV-787 (a bifunctional degrader targeting BET) and ORM-5029 (a molecular glue targeting GSPT1) have also announced termination of development. In addition to developing new therapeutic drugs, work is also underway to develop ADCs carrying multiple payloads. Advanced site-specific conjugation technologies have achieved precise control over DAR values, and even allow for the construction of homogeneous multi-payload ADCs. Currently, two dual-payload ADCs have entered clinical trials, and more than ten (including complex multi-payload constructs) have published preclinical data. Dual-payload/multi-payload strategies are expected to enhance efficacy by combining different mechanisms of action and non-overlapping toxicity profiles, blocking resistance escape pathways, and improving safety. A recent clinical trial using ADCs targeting different targets and carrying different payloads (SG and EV) in combination for urothelial carcinoma showed higher therapeutic activity, but also higher toxicity than using either drug alone. It remains unclear whether delivering multiple payloads simultaneously on a single antibody backbone will produce synergistic effects (or even additive effects), and whether the resulting therapeutic benefit increment can offset the higher toxicity risk and cross-resistance selection risk.Conclusion Over the past 40 years, we have made significant progress in understanding ADCs, but many questions remain to be clarified. This phenomenon may not be surprising: even traditional chemotherapeutic agents that have been widely used for decades have only partially understood the mechanisms behind their therapeutic indices. The mechanisms of ADCs are even more complex, relying on a combination of factors such as target expression, linker stability, cleavage mechanisms, tissue-specific sensitivity to payloads, immune interactions, and the complexity of the tumor microenvironment. To fully realize the therapeutic potential of ADCs, breakthroughs are needed in multiple areas: developing better detection methods, discovering new biomarkers, and continuing innovation in antibody engineering, payload diversification, and linker design. Equally important is data-driven clinical progress—developing patient-centered dosing regimens, treatment sequences, and combination strategies to maximize efficacy while ensuring tolerability. We anticipate that as numerous ADC clinical trials continue to generate new insights, ADC therapy will soon transition from a purely empirical approach to a more mechanism-guided modular design, ultimately leading to the development of safer, more selective, and more effective therapeutic options.References:
Resistance, Treatment Sequence, and Payload Diversification Discussions about ADC resistance often focus on its unique resistance mechanisms, such as the loss of target antigen expression following ADC treatment. In ADCs targeting CD30, CD33, Nectin-4, and HER2, a decrease in target antigen expression has been observed. Similarly, target antigens often undergo mutations, such as truncation of the HER2 extracellular domain, splice variants of CD33 that lose target epitopes, and missense mutations in TROP2 that affect membrane localization. In addition, there are other non-antigen-dependent ADC-specific resistance mechanisms, including reduced lysosomal proteolytic activity and abnormal lysosomal membrane transport function. Recent research data has focused on payload-related resistance. In mBC, Abelman et al. confirmed that the emergence of TOP1 mutations leads to cross-resistance to multiple TOP1i payloads. Jacot et al. also detected TOP1 mutations in some patients receiving T-DXd treatment. Other preclinical studies and recent clinical data from the DESTINY-Breast02 and DESTINY-Breast03 trials support these findings: inmBC patients, efficacy can still be achieved after T-DXd treatment when subsequently using HER2-targeted small molecule drugs or antibody drugs. Other clinical evidence points to similar conclusions. A large real-world study of mBC patients after T-DXd treatment found that patients using non-TOP1i chemotherapy drugs had better outcomes compared to those using another TOP1i ADC (SG). Similarly, a retrospective analysis involving 111 metastatic breast cancer patients showed that HER2-high expressing patients receiving a second ADC with the same type of payload had shorter PFS than those receiving ADCs with different types of payloads. There are reasons to question whether this resistance dynamic applies to tumor types beyond HER2-positive cancers—HER2-positive cancers are characterized by strong oncogene dependence and abnormally high protein expression levels. Recent data indicate that payload-mediated resistance is not unique to HER2-positive cancers. Two real-world studies found thatmBC patients who received T-DXd treatment after stopping SG had shorter PFS and OS than those who had not received SG treatment. Similarly, in the prospective trial assessing Datopotamab deruxtecan, nearly all patients with efficacy had not previously received TOP1i drugs. In a smaller trial, Emiltatug legadotin, targeting B7-H4 and carrying anti-microtubule payloads, still showed activity in TNBC patients who progressed after treatment with TOP1i ADCs. Drug efflux pumps are another resistance mechanism related to payloads. Multi-omics analysis of tumor samples from 2799 breast cancer patients treated with T-DXd revealed that patients with high expression levels of the multidrug resistance protein 1 (MDR1) gene had shorter overall survival, regardless of their HER2 expression levels (high or low). Other studies have also found that patients with high expression levels of P-glycoprotein (another efflux pump associated with resistance) had poorer treatment responses. In acute myeloid leukemia (AML) patients, strong P-glycoprotein function was also associated with poor responses to Gemtuzumab ozogamicin treatment. Notably, preclinical models of urothelial carcinoma found that disrupting efflux pump function could restore sensitivity in cells resistant to ADCs. Several prospective trials are currently evaluating the efficacy of TOP1i ADCs in patients who have previously received TOP1i ADCs, including TRADE-DXd (NCT06533826), SATEEN (NCT06100874), SERIES (NCT06263543), and ENCORE (NCT06774027). These studies will help clarify the benefits of sequential ADC treatment—this issue becomes particularly critical as ADCs are increasingly used in first-line and adjuvant therapies. Beyond HER2 targets, several next-generation ADCs are in clinical trials, including multiple novel ADCs targeting Nectin-4 with different TOP1i payloads. Many patients in these trials have previously received EV treatment, providing an opportunity to compare efficacy between different payloads. Among them, early trial results of the Nectin-4-targeting TOP1i ADC SHR-A2102 showed good therapeutic activity in urothelial carcinoma patients (including those who had previously received non-TOP1i ADCs). Payloads have become a core influencing factor in ADC resistance, highlighting the need to develop more differentiated payload categories. Early ADCs primarily used microtubule inhibitors or DNA-targeting drugs as payloads. Subsequently, the variety of payloads gradually diversified, with a significant increase in the application of topoisomerase inhibitors. Next-generation payloads in development are even more diverse, including radioactive ligands, RNA polymerase inhibitors, bifunctional and molecular glue degraders, Bcl-2 family protein modulators, and immune activators. Although differentiated payloads are attractive and necessary to develop, they still require comprehensive evaluation. For example, amanitin toxins are insensitive to drug efflux pumps, but their high systemic toxicity and hydrophilicity pose challenges for their application. The failure of several new payload developments also highlights the challenges in this field: multiple immunostimulatory ADCs, including NJH395, BDC-1001, SBT6050, SBT6290, and TAK-500, have been discontinued; two conjugates targeting BCL-XL, ABBV-155 and ABBV-637, have also been paused; recently, two Degrader-antibody conjugates (DAC) drugs: ABBV-787 (a bifunctional degrader targeting BET) and ORM-5029 (a molecular glue targeting GSPT1) have also announced termination of development. In addition to developing new therapeutic drugs, work is also underway to develop ADCs carrying multiple payloads. Advanced site-specific conjugation technologies have achieved precise control over DAR values, and even allow for the construction of homogeneous multi-payload ADCs. Currently, two dual-payload ADCs have entered clinical trials, and more than ten (including complex multi-payload constructs) have published preclinical data. Dual-payload/multi-payload strategies are expected to enhance efficacy by combining different mechanisms of action and non-overlapping toxicity profiles, blocking resistance escape pathways, and improving safety. A recent clinical trial using ADCs targeting different targets and carrying different payloads (SG and EV) in combination for urothelial carcinoma showed higher therapeutic activity, but also higher toxicity than using either drug alone. It remains unclear whether delivering multiple payloads simultaneously on a single antibody backbone will produce synergistic effects (or even additive effects), and whether the resulting therapeutic benefit increment can offset the higher toxicity risk and cross-resistance selection risk.Conclusion Over the past 40 years, we have made significant progress in understanding ADCs, but many questions remain to be clarified. This phenomenon may not be surprising: even traditional chemotherapeutic agents that have been widely used for decades have only partially understood the mechanisms behind their therapeutic indices. The mechanisms of ADCs are even more complex, relying on a combination of factors such as target expression, linker stability, cleavage mechanisms, tissue-specific sensitivity to payloads, immune interactions, and the complexity of the tumor microenvironment. To fully realize the therapeutic potential of ADCs, breakthroughs are needed in multiple areas: developing better detection methods, discovering new biomarkers, and continuing innovation in antibody engineering, payload diversification, and linker design. Equally important is data-driven clinical progress—developing patient-centered dosing regimens, treatment sequences, and combination strategies to maximize efficacy while ensuring tolerability. We anticipate that as numerous ADC clinical trials continue to generate new insights, ADC therapy will soon transition from a purely empirical approach to a more mechanism-guided modular design, ultimately leading to the development of safer, more selective, and more effective therapeutic options.References:
1、https://doi.org/10.1200/JCO-25-01235
2、https://www.henlius.com/upload/202509/07/HenliusWCLCHLX43HLX07HLX10Datareadout20250902.pdf
3、Sutro official website