 Introduction
Introduction
Protein drugs have the potential to induce immunogenicity, which can affect efficacy and even jeopardize life. New models of biotherapy, such as antibody-drug conjugates (ADC), fusion proteins, and pegylation, carry non-native human protein sequences and/or structural motifs, which may increase their immunogenicity risk. Therefore, comprehensive risk assessments, strategies, and analyses are needed to monitor and characterize the immunogenicity of ADCs and other biotherapies to predict and understand potential clinical outcomes.
ADCs are covalently linked to cytotoxic agents via stable linkers through monoclonal antibodies (mAb), combining the specificity of monoclonal antibodies for tumor cell surface target antigens with the efficacy of cytotoxic drugs. While current ADCs use human or humanized monoclonal antibodies and small molecule payloads, their semi-antigenic structures may increase their potential for immunogenicity compared to therapeutic monoclonal antibodies.
Anti-drug antibodies (ADAs) can target different domains in ADCs, such as mAb epitopes, novel mAb epitopes, linkers, and cytotoxic agents. If large ADC-ADA immune complexes are taken up by non-target immune cells leading to cell death, the presence of anti-cytotoxic agent ADAs poses potential safety risks.
It is generally accepted that industry practices and regulatory guidelines for assessing the immunogenicity of biotherapeutics apply to ADCs. A key aspect of ADC immunogenicity assessment is risk evaluation, appropriate testing, and additional characteristics of ADA domain specificity. Immunogenicity risk assessment includes various known factors related to patients and products that may affect the drug’s immunogenicity and the potential consequences of immune responses. For ADCs, this risk is typically considered higher than that for therapeutic monoclonal antibodies.
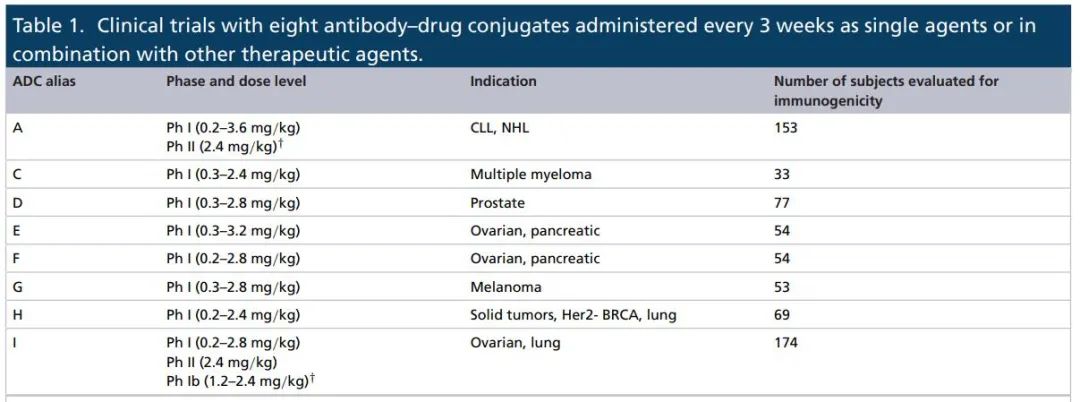
Based on risk assessment, immunogenicity data analysis for eight ADC drugs in eleven clinical trials involving a range of solid tumors and hematological malignancies is presented here. For each ADC, the incidence of ADAs at baseline, post-treatment incidence, and other characteristics of immune responses were evaluated.
Baseline Incidence of ADAs
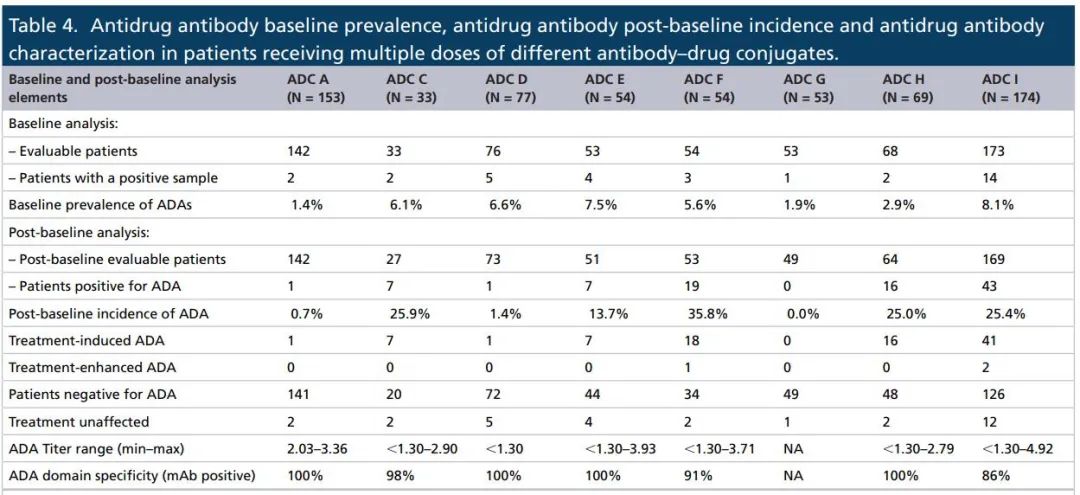
From the baseline incidence of ADAs data obtained from all ADC studies, the baseline incidence of ADAs ranged from 1.4% to 8.1%, which falls within the range reported for other monoclonal antibody-derived biotherapies, including the ADC drug Kadcyla.
In the clinical studies of these eight ADC antibodies, these antibodies are less likely to be associated with other components of the ADC. Additionally, in the evaluated eight ADCs, the background signal in the untreated patient population samples was similar to the mixed serum control signal from healthy volunteers.
Post-Treatment Incidence of ADAs
The incidence of ADAs post-baseline ranged from 0 to 35.8%, with ADC patients targeting hematological malignancies having fewer ADAs than those targeting solid tumors, with 8 out of 169 cases and 83 out of 459 cases, respectively, which can be attributed to immune killing in hematological malignancy patients.
However, there were some exceptions in ADA incidence, such as ADC C targeting plasma cells with an ADA incidence of 25.9%, while the incidence for ADC G in melanoma was 0%, but patients received glucocorticoids as part of treatment, which have known immunosuppressive effects.
Some studies were also conducted on ADC A and I; ADC A had only one patient with treatment-induced ADAs in one study. Regarding ADC I, the number of ADA-positive patients in the study ranged from 5 to 18, with corresponding ADA incidence rates from 20.8% to 32.0%. Notably, in phase I studies, the ADA incidence was higher in ovarian cancer patients than in lung cancer patients, at 31.0% (9/29) and 16.4% (9/55), respectively. Similar ADA incidence was observed in phase II studies for ovarian cancer patients.
TMB as a Biomarker: Applications and Challenges
For the eight ADCs evaluated here, most ADAs targeted the mAb domains of the ADCs, ranging from 86% to 100%. These results are consistent with those of Adcetris (brentuximab-vedotin), which shares the same linker and toxic drug as the eight ADCs introduced in this paper.
Overall, these data suggest that the semi-antigenic structures of these ADCs do not appear to increase their immunogenicity risk in most patients compared to traditional therapeutic monoclonal antibodies.
Regarding ADA levels, the total titers of these ADCs varied widely, from less than 1.30 to 4.92 titer units, with all ADCs having an average titer exceeding 2.50 titer units.
For the timing of treatment-induced ADA occurrence, it showed variability across all ADCs, with ADA occurrence timing ranging from 3 to 42 weeks. Furthermore, in six of the eight ADCs, more than 60% of patients developed ADAs within 3 to 6 weeks after starting treatment.
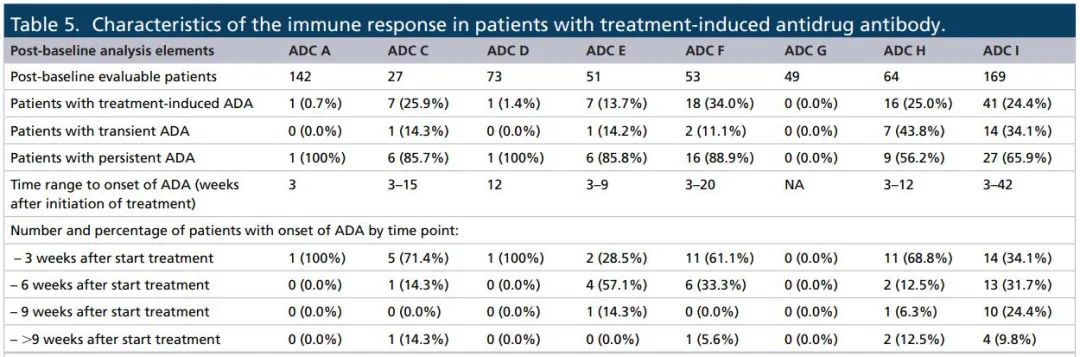
The majority of responses across all ADCs were sustained, with ADC H and I having the highest transient responses (43.8% and 34.1%, respectively). However, categorizing ADA responses as sustained or transient in oncology studies may be misleading due to typically short treatment durations. In fact, a more detailed data evaluation of ADA-positive responses indicated higher ADA positivity rates for three ADCs (ADC F, H, and I).
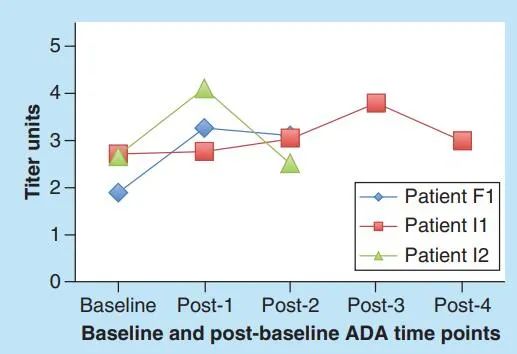
Out of 652 patients, 33 had antibodies at baseline, with 3 showing enhanced ADA responses. The ADA titers for these three patients varied over time, with baseline titers ranging from 1.89 to 2.71, while post-baseline titers ranged from 2.50 to 4.10. Among these three patients, 2 showed peak ADA responses at the first post-baseline time point, with the time range of enhanced responses being 3 to 9 weeks. The ADA levels for all patients at the last time point were below peak levels. ADA domain specificity remained consistent at baseline and post-baseline time points.
Impact of ADAs on Other Clinical Data
Immunogenicity is an important component of the clinical characteristics of protein drugs, and its data should be evaluated in the context of other factors (such as efficacy, PK, and safety). Here we focus on the three ADCs with a higher number of patients producing ADAs, namely ADC F, H, and I, with 19, 16, and 43 patients respectively showing post-baseline ADA positivity.
ADC F had an ADA incidence rate of 35.8% (19/53), with 18 patients having treatment-induced ADAs and 1 having treatment-enhanced ADAs. Overall, no differences in PK, safety, or efficacy outcomes were observed compared to patients who did not produce ADC F antibodies. Furthermore, ADA titers did have an impact on PK for these patients, but this had been previously reported in cynomolgus monkeys.
For ADC H, the ADA incidence rate was 25% (16/64), with all 16 patients having treatment-induced ADAs. Similar to ADC F, some patients with higher ADA titers had lower total antibody trough levels compared to those with lower ADA titers, but there was no correspondence between higher total ADA titers and lower total antibody levels.
For ADC I, a total of 43 patients showed ADAs, with 41 induced and 2 enhanced. Notably, 7 patients (including 2 with enhanced ADAs) had total antibody levels below the detection threshold at one or more trough time points. However, comprehensive analysis is still needed to conclude whether ADA titers have an impact on PK for these patients. It is noteworthy that high ADA titers (∼4.00) significantly affected the PK curve of trastuzumab ADC in cynomolgus monkeys.
Limited data from marketed ADCs indicate that ADAs have minimal impact on clinical outcomes. Adcetris has a 37% incidence of ADAs, with a higher frequency of infusion reactions in patients with persistent positive ADAs, leading to treatment discontinuation in two patients. The incidence of ADAs with Kadcyla is 5.3%, and the development of ADAs appears to have no effect on safety, PK, or efficacy. In a phase I study, Mylotarg had some ADA-positive patients, with one experiencing transient dyspnea associated with ADAs. No additional immunogenicity data for Mylotarg has been generated under the currently recommended dosing regimen in clinical trials. In the clinical trials of Besponsa, the incidence of ADAs was 3%, with no impact on the clearance rate of the ADC.
Conclusion
In a broad range of tumor indications across eleven clinical trials, the incidence of ADAs for eight vc-MMAE-ADCs ranged from 0-35.8%. The majority of ADA responses targeted the mAb domains within the ADCs, indicating that the semi-antigenic structures play a very minor role in generating immune responses against these ADCs. These results reinforce the fact that molecular structure is an important factor in biotherapy immune responses but not the only one.
Although the data for these eight vc-MMAE-ADCs suggest that the risk may decrease as projects enter later stages of clinical development, a conservative approach is still recommended for novel ADCs that may use different linkers and more potent cytotoxic agents. Furthermore, as predictive immunogenicity tools become more widely used, they will provide additional information for incorporating risk assessments and immunogenicity strategies for ADCs and novel therapies.
References:
1. Immunogenicity of antibody-drug conjugates: observations across 8 molecules in 11 clinical trials. Bioanalysis. 2019 Sep;11(17):1555-1568.
