WCLC 2025 has numerous topics on ADCs, and in the spirit of learning, I am joining the discussion. Let’s see how ADCs are viewed in the field of lung cancer, a leading area in cancer treatment, and what research directions exist for ADCs in this domain.Biomarkers for ADCs: IHC and Beyond, presented by Dr. Sewanti Limaye from Sir H.N. Reliance Foundation Hospital in Mumbai, India. First, starting with “ADC and its Development,” the basic background of ADCs is introduced; then, through “Why Biomarkers are Needed,” the core value of biomarkers in ADC therapy is explained; next, it focuses on “New ADCs and the Demand for Biomarker Recognition in the New Era,” linking the cutting edge of clinical research and the innovation of biomarkers; the middle section delves into “IHC-based Biomarkers for ADC Target Recognition” and “Novel Biomarkers and Drug Development Beyond IHC,” covering both traditional detection methods and extending into emerging technology fields; finally, it concludes with “Challenges and Future Directions,” summarizing current limitations and looking forward to development paths.
First, starting with “ADC and its Development,” the basic background of ADCs is introduced; then, through “Why Biomarkers are Needed,” the core value of biomarkers in ADC therapy is explained; next, it focuses on “New ADCs and the Demand for Biomarker Recognition in the New Era,” linking the cutting edge of clinical research and the innovation of biomarkers; the middle section delves into “IHC-based Biomarkers for ADC Target Recognition” and “Novel Biomarkers and Drug Development Beyond IHC,” covering both traditional detection methods and extending into emerging technology fields; finally, it concludes with “Challenges and Future Directions,” summarizing current limitations and looking forward to development paths. Currently, 15 ADCs have been approved globally, reshaping the landscape of cancer treatment, particularly in addressing the three major clinical pain points of tumor heterogeneity, drug resistance, and off-target toxicity.
Currently, 15 ADCs have been approved globally, reshaping the landscape of cancer treatment, particularly in addressing the three major clinical pain points of tumor heterogeneity, drug resistance, and off-target toxicity.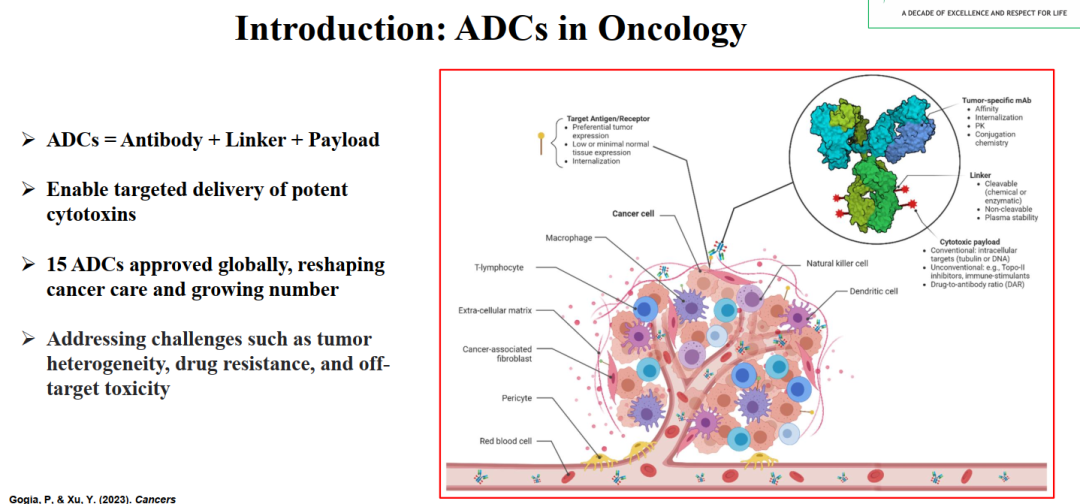 As of 2023, the approved ADC drugs include:Breast cancer-related ADCs include Kadcyla (Trastuzumab emtansine, targeting HER2, approved in 2013 for breast cancer), Sacituzumab govitecan (targeting TROP2, approved in 2020 for triple-negative breast cancer), etc.The selection of ADC targets in lung cancer appears to be broader than in breast cancer, with CEACAM5 and c-MET being previously unfamiliar research targets in breast cancer.
As of 2023, the approved ADC drugs include:Breast cancer-related ADCs include Kadcyla (Trastuzumab emtansine, targeting HER2, approved in 2013 for breast cancer), Sacituzumab govitecan (targeting TROP2, approved in 2020 for triple-negative breast cancer), etc.The selection of ADC targets in lung cancer appears to be broader than in breast cancer, with CEACAM5 and c-MET being previously unfamiliar research targets in breast cancer.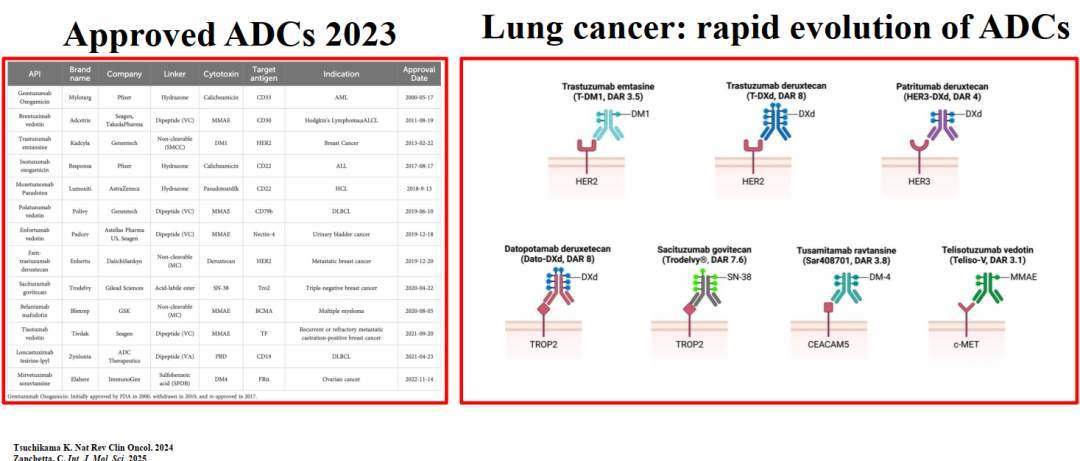 Currently, ADC drugs under investigation include:Glembatumumab vedotin (targeting gpNMB, for metastatic breast cancer and melanoma, Phase II), Ladiraturumab vedotin (targeting LIV-1, for breast cancer, Phase II), SARS666658 (targeting CA6, for triple-negative breast cancer, Phase II). These ADCs target previously underrepresented targets in breast cancer (e.g., high expression of gpNMB in triple-negative breast cancer), filling existing treatment gaps.From a technical perspective, most ADCs under investigation utilize cleavable dipeptide linkers, with cytotoxins primarily being MMAE (microtubule inhibitors) and DM4 (maytansinoids), balancing efficacy and safety; Phase III ADCs such as Rovalpituzumab tesirine (targeting DLL3, for small cell lung cancer) and Mirvetuximab soravtansine (targeting FRα, for ovarian cancer and non-small cell lung cancer) are not directly targeting breast cancer, but their research ideas (e.g., expression of FRα in certain breast cancer subtypes) provide references for breast cancer ADC development.
Currently, ADC drugs under investigation include:Glembatumumab vedotin (targeting gpNMB, for metastatic breast cancer and melanoma, Phase II), Ladiraturumab vedotin (targeting LIV-1, for breast cancer, Phase II), SARS666658 (targeting CA6, for triple-negative breast cancer, Phase II). These ADCs target previously underrepresented targets in breast cancer (e.g., high expression of gpNMB in triple-negative breast cancer), filling existing treatment gaps.From a technical perspective, most ADCs under investigation utilize cleavable dipeptide linkers, with cytotoxins primarily being MMAE (microtubule inhibitors) and DM4 (maytansinoids), balancing efficacy and safety; Phase III ADCs such as Rovalpituzumab tesirine (targeting DLL3, for small cell lung cancer) and Mirvetuximab soravtansine (targeting FRα, for ovarian cancer and non-small cell lung cancer) are not directly targeting breast cancer, but their research ideas (e.g., expression of FRα in certain breast cancer subtypes) provide references for breast cancer ADC development.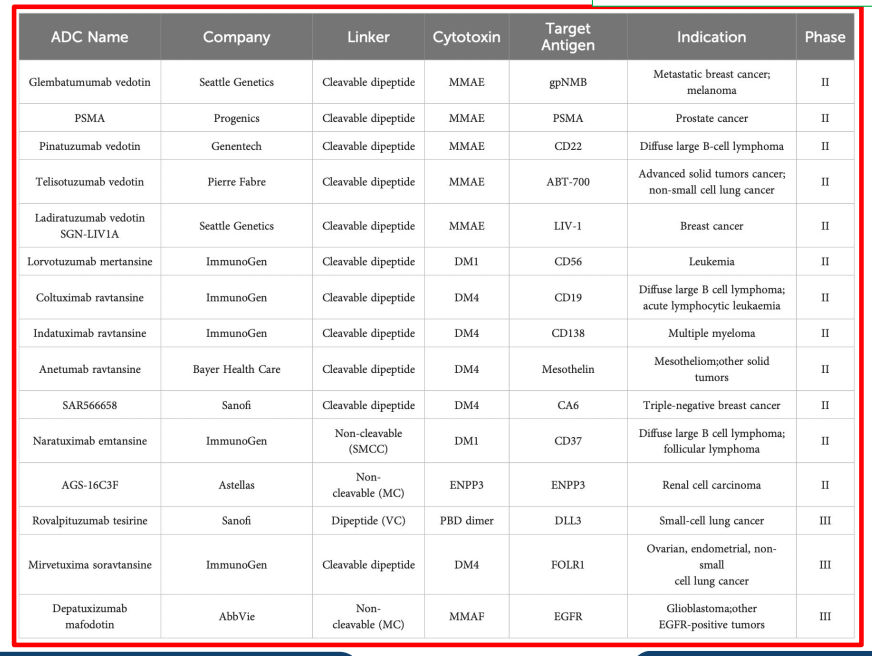 “New ADC Design: Bispecific ADCs,” a diagram of the mechanism of action of bispecific ADCs and a detailed table of in-development bispecific ADCs, aims to address the limitations of traditional single-target ADCs in dealing with tumor heterogeneity.The left diagram shows two designs of bispecific ADCs: one is a bispecific ADC (BL-B01D1), which binds to both EGFR and B7H3 simultaneously, precisely anchoring cancer cells; the other is a bispecific ADC (ZW49), which binds to different epitopes of the HER2 protein, enhancing affinity for HER2-expressing cells, both designs ultimately deliver payloads through linkers to induce apoptosis in cancer cells.The right table lists 16 bispecific ADCs under investigation, their target pairs (e.g., EGFR×B7H3, Nectin4×TROP2, HER2×TROP2), development codes, companies, molecular formats (e.g., 1+1, 2+2 Fab/ScFv), cytotoxins (primarily topoisomerase inhibitors), additional technologies (e.g., Fc silent to reduce ADCC effects, Common LC to simplify production), and development stages (mostly preclinical or discovery stages). Among them, HER2×TROP2, EGFR×HER3, etc., directly target breast cancer heterogeneity — for instance, HER2-low breast cancer may simultaneously express high levels of TROP2, and bispecific ADCs can target both antigens to enhance efficacy; technologies like Fc silent reduce off-target toxicity and improve the therapeutic window. This page reflects the potential of bispecific ADCs in the precise treatment of breast cancer, providing new strategies to address traditional ADC resistance and heterogeneity issues.
“New ADC Design: Bispecific ADCs,” a diagram of the mechanism of action of bispecific ADCs and a detailed table of in-development bispecific ADCs, aims to address the limitations of traditional single-target ADCs in dealing with tumor heterogeneity.The left diagram shows two designs of bispecific ADCs: one is a bispecific ADC (BL-B01D1), which binds to both EGFR and B7H3 simultaneously, precisely anchoring cancer cells; the other is a bispecific ADC (ZW49), which binds to different epitopes of the HER2 protein, enhancing affinity for HER2-expressing cells, both designs ultimately deliver payloads through linkers to induce apoptosis in cancer cells.The right table lists 16 bispecific ADCs under investigation, their target pairs (e.g., EGFR×B7H3, Nectin4×TROP2, HER2×TROP2), development codes, companies, molecular formats (e.g., 1+1, 2+2 Fab/ScFv), cytotoxins (primarily topoisomerase inhibitors), additional technologies (e.g., Fc silent to reduce ADCC effects, Common LC to simplify production), and development stages (mostly preclinical or discovery stages). Among them, HER2×TROP2, EGFR×HER3, etc., directly target breast cancer heterogeneity — for instance, HER2-low breast cancer may simultaneously express high levels of TROP2, and bispecific ADCs can target both antigens to enhance efficacy; technologies like Fc silent reduce off-target toxicity and improve the therapeutic window. This page reflects the potential of bispecific ADCs in the precise treatment of breast cancer, providing new strategies to address traditional ADC resistance and heterogeneity issues.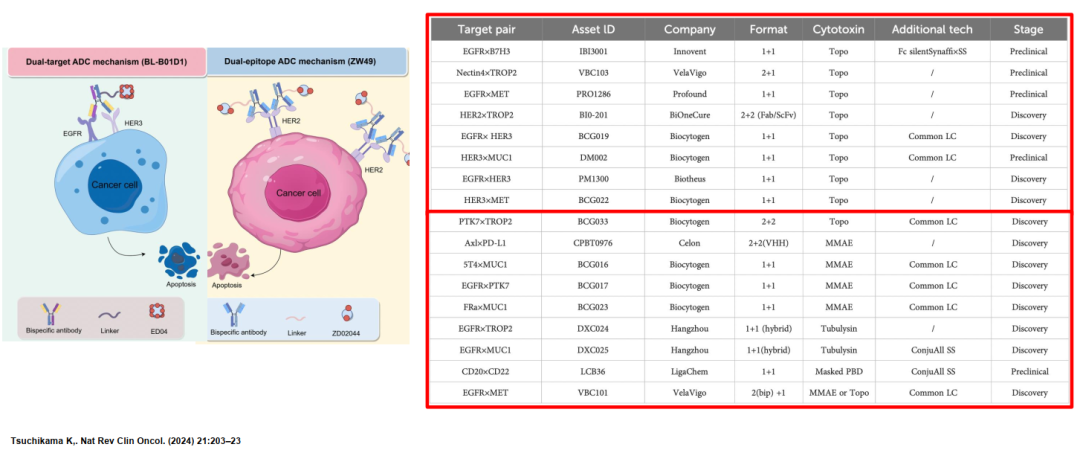 “New ADC Designs” focuses on three innovative structures: Prodrug ADCs, Immunostimulatory ADCs, and Degradative ADCs, breaking through the traditional ADC function of “only delivering cytotoxins.”
“New ADC Designs” focuses on three innovative structures: Prodrug ADCs, Immunostimulatory ADCs, and Degradative ADCs, breaking through the traditional ADC function of “only delivering cytotoxins.”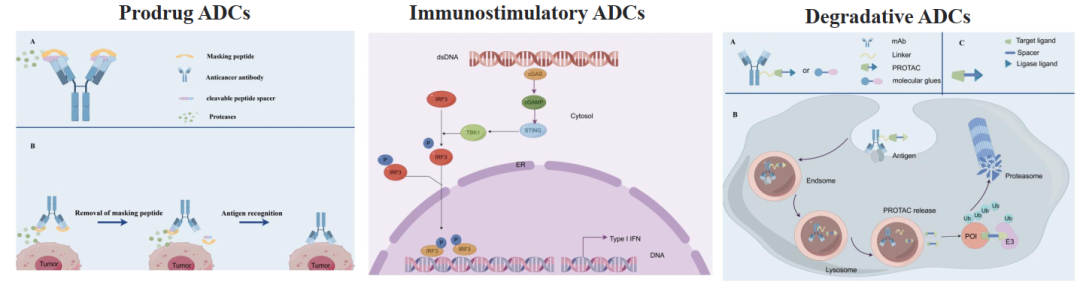 (Tsuchikama K. Nat Rev Clin Oncol. (2024) 21:203–23)
(Tsuchikama K. Nat Rev Clin Oncol. (2024) 21:203–23)
- Prodrug ADCs: By modifying antibodies or payloads with “masking peptides,” they remain inactive in normal tissues and become active upon entering the tumor microenvironment (e.g., activated by tumor-specific enzymes), shedding the masking peptide, restoring ADC activity and releasing the payload, significantly reducing off-target toxicity, especially suitable for payloads with high toxicity to normal tissues (e.g., potent topoisomerase inhibitors).
- Immunostimulatory ADCs: On the basis of traditional cytotoxicity, they integrate immunostimulatory elements (e.g., dsDNA), which not only directly kill cancer cells but also activate immune cells in the tumor microenvironment (e.g., dendritic cells, T cells), triggering an anti-tumor immune response, forming a dual mechanism of “cytotoxicity + immune activation,” suitable for immunosuppressive breast cancer subtypes (e.g., triple-negative breast cancer).
- Degradative ADCs: By combining ADCs with PROTAC (proteolysis-targeting chimeras), after entering cancer cells, ADCs not only release the payload but also mediate the ubiquitination and degradation of target antigen proteins (e.g., HER2), upgrading from “inhibiting target function” to “clearing target proteins,” effectively overcoming resistance caused by target mutations (e.g., HER2 mutant breast cancer). The mechanism diagram at the bottom of the page visually presents the process of degradative ADCs: after binding to the target antigen, ADCs are endocytosed into endosomes, then transported to lysosomes, where the linker breaks and releases PROTAC, which recruits E3 ubiquitin ligase to mediate target protein degradation. These new designs provide a “low toxicity, strong immune response, anti-resistance” direction for breast cancer ADC therapy, especially significant for refractory breast cancers (e.g., resistant triple-negative breast cancer, HER2 mutant breast cancer).
Three core values of biomarkers in ADC therapy — patient selection, efficacy prediction, resistance and safety management, while proposing solutions to key issues in breast cancer ADC therapy (e.g., antigen expression levels, tumor heterogeneity).Patient selection: By identifying patients most likely to respond to ADCs through biomarkers (e.g., HER2 expression, TROP2 expression), ineffective treatments can be avoided; attention must be paid to antigen expression heterogeneity (intra-tumor/inter-tumor differences), for example, HER2 expression may vary between different lesions in the same breast cancer patient, requiring multi-region biopsies or nuclear imaging assessments.Efficacy prediction: Correlating biomarker status with treatment outcomes, for instance, markers related to payload delivery efficiency and target antigen internalization capacity (e.g., HER2 internalization rate) can predict T-DXd efficacy; simultaneously guiding optimal treatment choices, such as prioritizing Sacituzumab govitecan for TROP2 high-expressing triple-negative breast cancer.Resistance and safety: Early detection of resistance mechanisms (e.g., high expression of drug efflux pump genes) allows timely adjustments; monitoring toxicity-related markers (e.g., UGT1A1 polymorphisms and the risk of neutropenia with Sacituzumab govitecan) reduces adverse reactions. Intermediate expression level antigens (e.g., HER2 1+) may require combination therapy (ADC + immune checkpoint inhibitors / ADC + anti-angiogenic drugs); distinguishing between “driver factors” (e.g., HER2, which directly regulates tumor growth and shows significant ADC efficacy) and “passenger factors” (e.g., Nectin-4, which is highly expressed but not essential for tumors, showing limited efficacy); low-expressing antigens need to be quantified through digital pathology to avoid missing screenings; high-expressing antigens may consider de-escalation therapy (e.g., maintaining low-dose ADC). This content directly guides clinical decisions for breast cancer ADCs, for instance, HER2-low breast cancer requires precise detection to determine expression thresholds, avoiding misclassification as HER2-negative and missing treatment opportunities.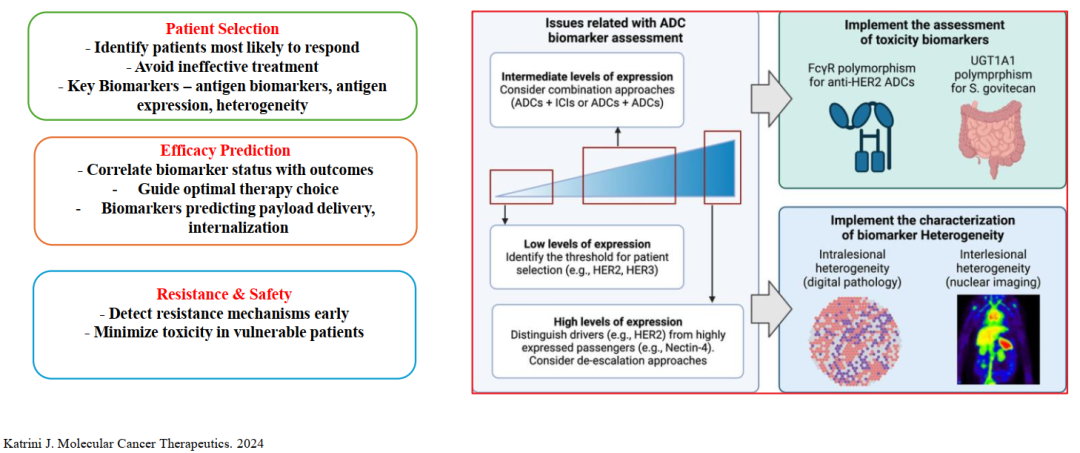 “The Current Role and Controversies of IHC,” the status and limitations of immunohistochemistry (IHC) as the gold standard for ADC biomarkers, especially addressing the core controversy in breast cancer ADC therapy — the HER2-low / ultra-low expression issue.Core but Limited Role: IHC is the standard detection method for ADC target antigens such as HER2, TROP2, Nectin-4, TF, FRα, for example, HER2 IHC 3+/FISH + is the basis for the indication of Trastuzumab – emtansine (T-DM1); however, IHC is not a universal predictive factor, for instance, the FDA approval of Sacituzumab govitecan (targeting TROP2) does not require strict TROP2 IHC thresholds, and some patients with low TROP2 expression can still benefit, indicating that IHC cannot fully define the treatment population.Heterogeneity Issues: Differences in antigen expression within tumors (different regions of the same lesion) and between tumors (different lesions) lead to false negatives/positives in IHC detection, for example, HER2 IHC 2+ in the primary breast cancer lesion may be IHC 1+ in metastatic lesions, affecting ADC selection.HER2-low / Ultra-low Challenges: Traditional HER2 testing divides patients into positive (3+/FISH+) and negative (0/1+), but HER2-low (IHC 1+ or 2+/FISH-) breast cancer accounts for about 40%-50%, and the significant efficacy of T-DXd in this population (e.g., DESTINY-Breast04 study) proves that HER2-low is a treatable subtype, while the semi-quantitative nature of IHC (0/1+/2+/3+) cannot accurately distinguish between “effective HER2-low” and “ineffective ultra-low HER2,” weakening its status as the sole biomarker.ADC’s “Bystander Effect” (the released payload diffusing to adjacent cancer cells) can kill cells with low-expressing target antigens, which is also a key mechanism for HER2-low patients responding to T-DXd, while IHC cannot assess this “effect coverage range.”
“The Current Role and Controversies of IHC,” the status and limitations of immunohistochemistry (IHC) as the gold standard for ADC biomarkers, especially addressing the core controversy in breast cancer ADC therapy — the HER2-low / ultra-low expression issue.Core but Limited Role: IHC is the standard detection method for ADC target antigens such as HER2, TROP2, Nectin-4, TF, FRα, for example, HER2 IHC 3+/FISH + is the basis for the indication of Trastuzumab – emtansine (T-DM1); however, IHC is not a universal predictive factor, for instance, the FDA approval of Sacituzumab govitecan (targeting TROP2) does not require strict TROP2 IHC thresholds, and some patients with low TROP2 expression can still benefit, indicating that IHC cannot fully define the treatment population.Heterogeneity Issues: Differences in antigen expression within tumors (different regions of the same lesion) and between tumors (different lesions) lead to false negatives/positives in IHC detection, for example, HER2 IHC 2+ in the primary breast cancer lesion may be IHC 1+ in metastatic lesions, affecting ADC selection.HER2-low / Ultra-low Challenges: Traditional HER2 testing divides patients into positive (3+/FISH+) and negative (0/1+), but HER2-low (IHC 1+ or 2+/FISH-) breast cancer accounts for about 40%-50%, and the significant efficacy of T-DXd in this population (e.g., DESTINY-Breast04 study) proves that HER2-low is a treatable subtype, while the semi-quantitative nature of IHC (0/1+/2+/3+) cannot accurately distinguish between “effective HER2-low” and “ineffective ultra-low HER2,” weakening its status as the sole biomarker.ADC’s “Bystander Effect” (the released payload diffusing to adjacent cancer cells) can kill cells with low-expressing target antigens, which is also a key mechanism for HER2-low patients responding to T-DXd, while IHC cannot assess this “effect coverage range.”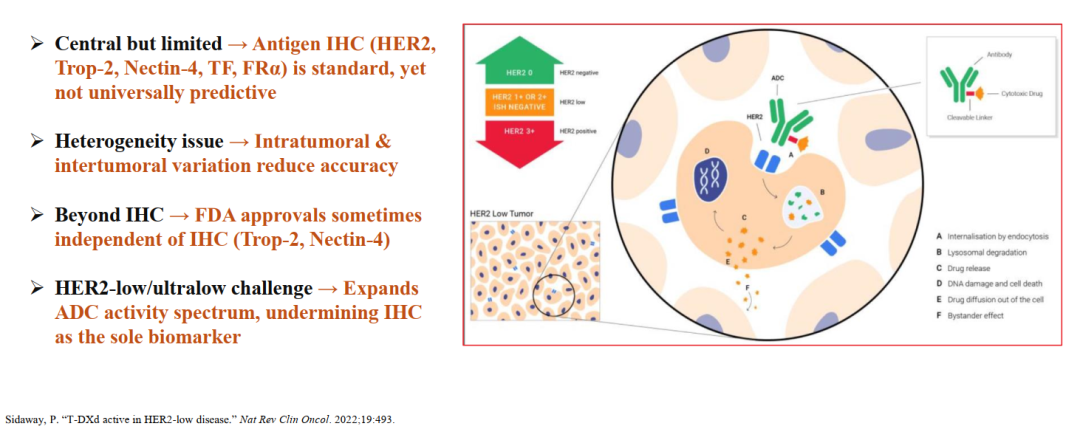 “New Biomarker Methods for ADCs” aims to address the limitations of IHC, listing six core technological directions and integrating the application scenarios of these methods through diagrams.Digital Pathology: Quantitative analysis of IHC slices through image analysis algorithms (e.g., AI) (e.g., continuous values of HER2 expression intensity, proportion of positive cells), replacing traditional semi-quantitative scoring, reducing inter-observer variability, especially suitable for precise definition of HER2-low.Molecular Imaging: For instance, PET-CT combined with target antigen-specific probes (e.g., HER2 probes, TROP2 probes) enables in vivo assessment of antigen expression in tumors, addressing the heterogeneity issue in multiple lesions (e.g., TROP2 expression detection in breast cancer bone metastases).Immunofluorescence (IF): Simultaneously detects multiple target antigens (e.g., HER2+TROP2+Ki-67), analyzing antigen co-expression patterns, guiding the selection of bispecific ADCs (e.g., HER2×TROP2 ADC).Mass Spectrometry: Quantitatively detects the absolute expression levels of target antigens in tumor tissues (rather than relative levels) through proteomics, accurately distinguishing between “effective expression” and “ineffective expression,” for example, the correlation between TROP2 protein concentration thresholds and the efficacy of Sacituzumab govitecan.Receptor mRNA: Detects target antigen mRNA levels through RT-PCR or RNA-seq, more sensitive than IHC (can detect low-expressing antigens), while capturing downstream signaling pathway genes (e.g., co-expression of HER2 mRNA + PI3K mRNA suggests potential benefit from ADC combined with PI3K inhibitors).Circulating Free DNA (cfDNA) and Circulating Tumor Cells (CTCs): Liquid biopsy technology, real-time monitoring of tumor gene mutations (e.g., HER2 mutations), changes in target antigen expression, used for monitoring resistance in ADC therapy (e.g., increased abundance of HER2 mutations in cfDNA after T-DXd treatment suggests resistance).These technologies can achieve “precise screening – efficacy monitoring – resistance warning” full-process management in breast cancer ADC therapy, especially valuable for refractory subtypes like HER2-low and triple-negative breast cancer.
“New Biomarker Methods for ADCs” aims to address the limitations of IHC, listing six core technological directions and integrating the application scenarios of these methods through diagrams.Digital Pathology: Quantitative analysis of IHC slices through image analysis algorithms (e.g., AI) (e.g., continuous values of HER2 expression intensity, proportion of positive cells), replacing traditional semi-quantitative scoring, reducing inter-observer variability, especially suitable for precise definition of HER2-low.Molecular Imaging: For instance, PET-CT combined with target antigen-specific probes (e.g., HER2 probes, TROP2 probes) enables in vivo assessment of antigen expression in tumors, addressing the heterogeneity issue in multiple lesions (e.g., TROP2 expression detection in breast cancer bone metastases).Immunofluorescence (IF): Simultaneously detects multiple target antigens (e.g., HER2+TROP2+Ki-67), analyzing antigen co-expression patterns, guiding the selection of bispecific ADCs (e.g., HER2×TROP2 ADC).Mass Spectrometry: Quantitatively detects the absolute expression levels of target antigens in tumor tissues (rather than relative levels) through proteomics, accurately distinguishing between “effective expression” and “ineffective expression,” for example, the correlation between TROP2 protein concentration thresholds and the efficacy of Sacituzumab govitecan.Receptor mRNA: Detects target antigen mRNA levels through RT-PCR or RNA-seq, more sensitive than IHC (can detect low-expressing antigens), while capturing downstream signaling pathway genes (e.g., co-expression of HER2 mRNA + PI3K mRNA suggests potential benefit from ADC combined with PI3K inhibitors).Circulating Free DNA (cfDNA) and Circulating Tumor Cells (CTCs): Liquid biopsy technology, real-time monitoring of tumor gene mutations (e.g., HER2 mutations), changes in target antigen expression, used for monitoring resistance in ADC therapy (e.g., increased abundance of HER2 mutations in cfDNA after T-DXd treatment suggests resistance).These technologies can achieve “precise screening – efficacy monitoring – resistance warning” full-process management in breast cancer ADC therapy, especially valuable for refractory subtypes like HER2-low and triple-negative breast cancer.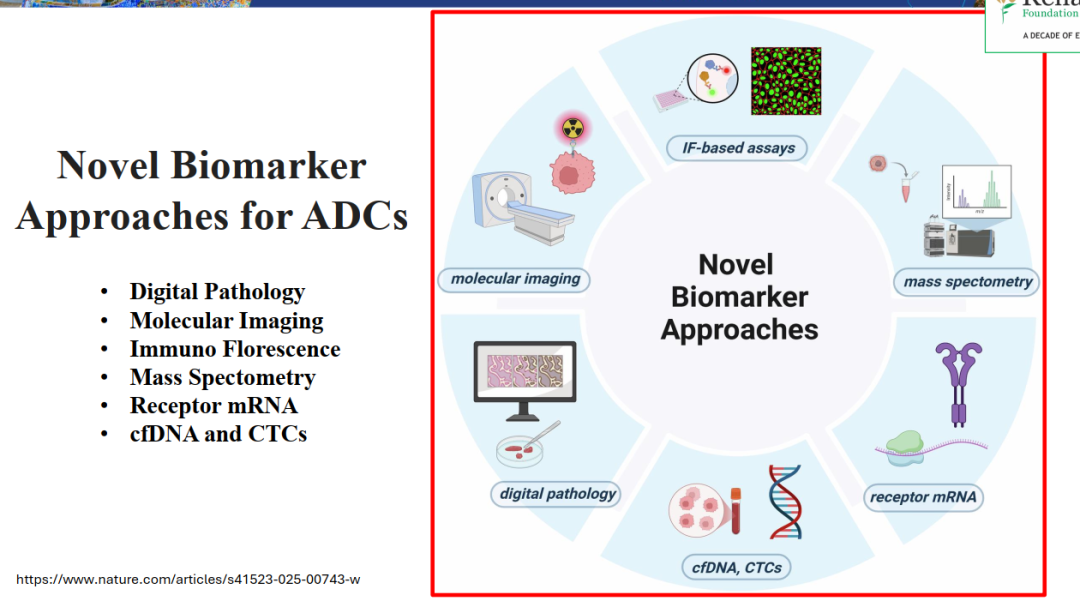 In the field of breast cancer, the analysis of biomarkers runs through the entire process of breast cancer treatment.
In the field of breast cancer, the analysis of biomarkers runs through the entire process of breast cancer treatment.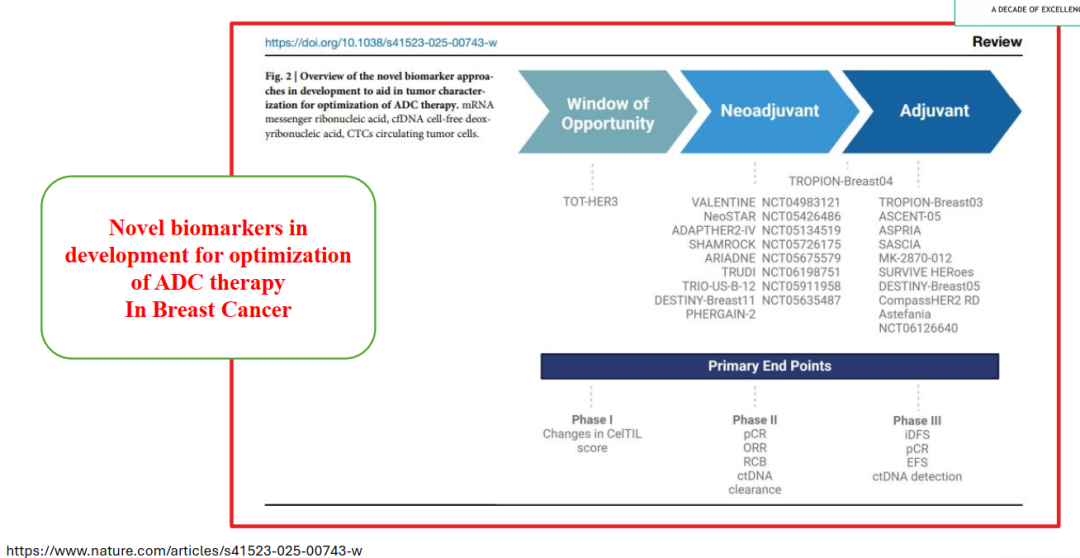 Lung cancer ADC’s new biomarker methodsALCAM (Activated Leukocyte Cell Adhesion Molecule): Corresponding ADCs include ORab-202, CX-2009, ADCT-601, ALCAM is highly expressed in NSCLC and is associated with tumor invasion and metastasis, and patients with high expression may respond better to these ADCs;TfR1 (Transferrin Receptor 1): Corresponding ADC is Vobramtma, TfR1 is highly expressed on the surface of NSCLC cells to meet the iron needs of rapid tumor proliferation, ADCs targeting TfR1 can precisely deliver cytotoxins, reducing damage to normal cells;NAPI2b (Sodium-dependent Phosphate Transporter 2b): Corresponding ADC is CX-2029, NAPI2b is expressed in about 40%-50% of lung adenocarcinoma, and also has some expression in squamous cell carcinoma, expanding the applicability of ADCs to lung cancer subtypes;LY6E (Lymphocyte Antigen 6 Complex E): Corresponding ADC is ASNoo4-X-5, LY6E is associated with tumor immune suppression in NSCLC, ADCs targeting LY6E can not only directly kill cancer cells but may also improve the tumor microenvironment, enhancing the synergistic effect of immunotherapy;LYPD3 (LY6/PLAUR Domain Containing Protein 3): No specific ADC name, but LY6D3 is highly expressed in NSCLC and is associated with poor prognosis, making it a potential ADC target, currently in preclinical or early development stages;ROR2 (Receptor Tyrosine Kinase-like Orphan Receptor 2): Corresponding ADC is Fre drug (simplified expression, presumed to be an investigational drug), ROR2 is involved in maintaining tumor stem cells in NSCLC, ADCs targeting ROR2 can inhibit tumor recurrence and metastasis;5T4 (Trophoblast Cell Surface Antigen 4): Corresponding ADC is BA30214, 5T4 is highly expressed in NSCLC and is associated with tumor invasiveness, especially higher expression rates in advanced NSCLC, making it suitable as a target for ADCs in advanced patients;B7-H3 (B7 Homolog 3 Protein): Corresponding ADC is xBozmab veloin (simplified expression, presumed to be investigational drugs like Ifinatamab deruxtecan), B7-H3 is expressed in about 50%-60% of NSCLC and does not significantly overlap with PD-L1 expression, providing a new ADC treatment direction for PD-L1 negative NSCLC;
Lung cancer ADC’s new biomarker methodsALCAM (Activated Leukocyte Cell Adhesion Molecule): Corresponding ADCs include ORab-202, CX-2009, ADCT-601, ALCAM is highly expressed in NSCLC and is associated with tumor invasion and metastasis, and patients with high expression may respond better to these ADCs;TfR1 (Transferrin Receptor 1): Corresponding ADC is Vobramtma, TfR1 is highly expressed on the surface of NSCLC cells to meet the iron needs of rapid tumor proliferation, ADCs targeting TfR1 can precisely deliver cytotoxins, reducing damage to normal cells;NAPI2b (Sodium-dependent Phosphate Transporter 2b): Corresponding ADC is CX-2029, NAPI2b is expressed in about 40%-50% of lung adenocarcinoma, and also has some expression in squamous cell carcinoma, expanding the applicability of ADCs to lung cancer subtypes;LY6E (Lymphocyte Antigen 6 Complex E): Corresponding ADC is ASNoo4-X-5, LY6E is associated with tumor immune suppression in NSCLC, ADCs targeting LY6E can not only directly kill cancer cells but may also improve the tumor microenvironment, enhancing the synergistic effect of immunotherapy;LYPD3 (LY6/PLAUR Domain Containing Protein 3): No specific ADC name, but LY6D3 is highly expressed in NSCLC and is associated with poor prognosis, making it a potential ADC target, currently in preclinical or early development stages;ROR2 (Receptor Tyrosine Kinase-like Orphan Receptor 2): Corresponding ADC is Fre drug (simplified expression, presumed to be an investigational drug), ROR2 is involved in maintaining tumor stem cells in NSCLC, ADCs targeting ROR2 can inhibit tumor recurrence and metastasis;5T4 (Trophoblast Cell Surface Antigen 4): Corresponding ADC is BA30214, 5T4 is highly expressed in NSCLC and is associated with tumor invasiveness, especially higher expression rates in advanced NSCLC, making it suitable as a target for ADCs in advanced patients;B7-H3 (B7 Homolog 3 Protein): Corresponding ADC is xBozmab veloin (simplified expression, presumed to be investigational drugs like Ifinatamab deruxtecan), B7-H3 is expressed in about 50%-60% of NSCLC and does not significantly overlap with PD-L1 expression, providing a new ADC treatment direction for PD-L1 negative NSCLC;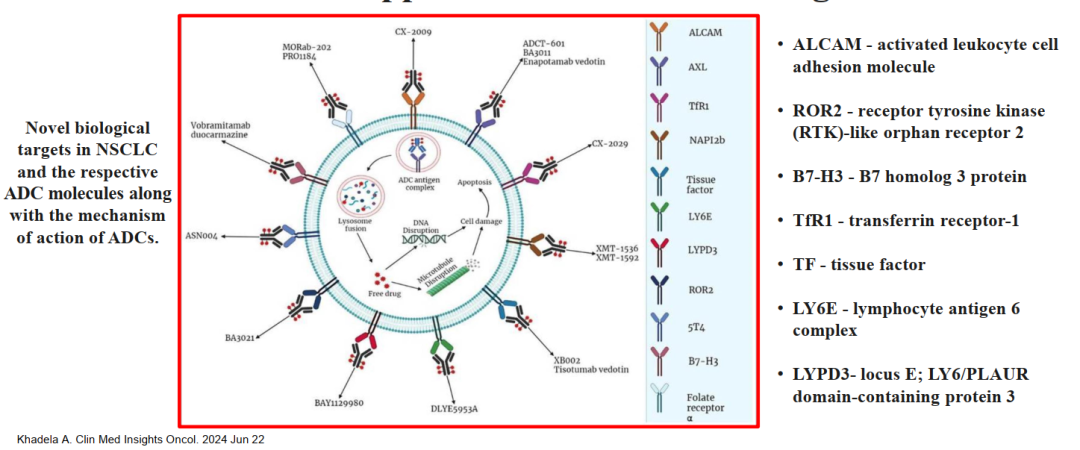 “Beyond IHC: AI and Digital Pathology”QCS-NMR Model: Targeting the TROP2 target antigen (the target of Sacituzumab govitecan), this AI model can accurately quantify the localization of TROP2 in tumor cells (e.g., cell membrane/cytoplasmic expression ratio) and expression intensity, rather than the semi-quantitative scoring of traditional IHC. Research (A Su et al., 2022, Nature affiliated journal) shows that in non-small cell lung cancer (NSCLC), QCS-NMR’s stratification effect on patients is superior to IHC, predicting TROP2-ADC efficacy more accurately; whether this technology can be transferred to breast cancer, especially suitable for the high heterogeneity of TROP2 expression in triple-negative breast cancer, avoiding patient misclassification due to IHC scoring differences, is worth studying.Universal IHC Analyzer (UIHC): Traditional IHC detection is greatly affected by staining conditions (e.g., antibody batches, staining time), resulting in low consistency of results between different laboratories; UIHC achieves “stain-independent” quantitative analysis through AI algorithms, standardizing the IHC interpretation process across different laboratories. For example, in HER2 detection, UIHC can eliminate inter-laboratory variability, ensuring consistent results for HER2-low (IHC 1+/2+/FISH-) breast cancer patients, providing a unified biomarker standard for multi-center ADC clinical trials (e.g., global trials of T-DXd). ADC biomarker detection has upgraded from “qualitative/semi-quantitative” to “precise quantitative + standardized,” providing technical support for the precise treatment of breast cancer ADCs, especially addressing the consistency issues in multi-center clinical practice.
“Beyond IHC: AI and Digital Pathology”QCS-NMR Model: Targeting the TROP2 target antigen (the target of Sacituzumab govitecan), this AI model can accurately quantify the localization of TROP2 in tumor cells (e.g., cell membrane/cytoplasmic expression ratio) and expression intensity, rather than the semi-quantitative scoring of traditional IHC. Research (A Su et al., 2022, Nature affiliated journal) shows that in non-small cell lung cancer (NSCLC), QCS-NMR’s stratification effect on patients is superior to IHC, predicting TROP2-ADC efficacy more accurately; whether this technology can be transferred to breast cancer, especially suitable for the high heterogeneity of TROP2 expression in triple-negative breast cancer, avoiding patient misclassification due to IHC scoring differences, is worth studying.Universal IHC Analyzer (UIHC): Traditional IHC detection is greatly affected by staining conditions (e.g., antibody batches, staining time), resulting in low consistency of results between different laboratories; UIHC achieves “stain-independent” quantitative analysis through AI algorithms, standardizing the IHC interpretation process across different laboratories. For example, in HER2 detection, UIHC can eliminate inter-laboratory variability, ensuring consistent results for HER2-low (IHC 1+/2+/FISH-) breast cancer patients, providing a unified biomarker standard for multi-center ADC clinical trials (e.g., global trials of T-DXd). ADC biomarker detection has upgraded from “qualitative/semi-quantitative” to “precise quantitative + standardized,” providing technical support for the precise treatment of breast cancer ADCs, especially addressing the consistency issues in multi-center clinical practice.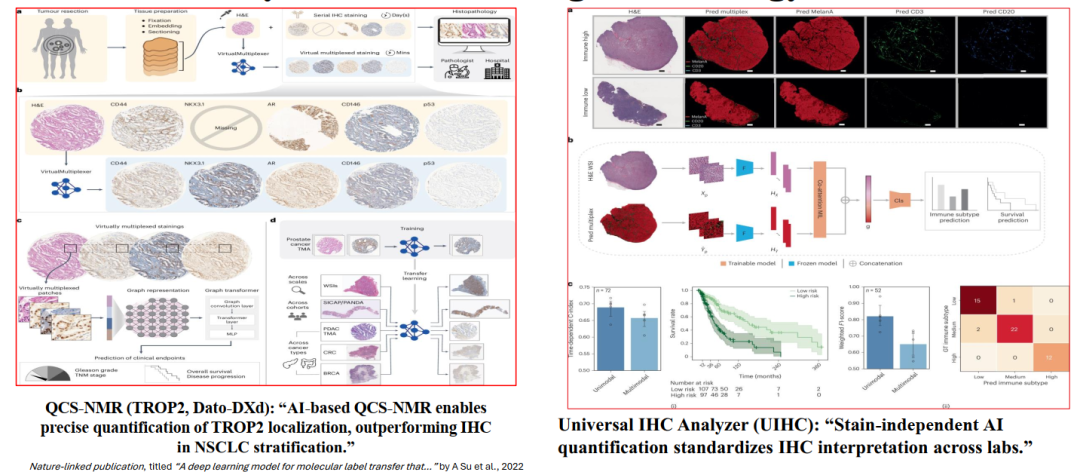 Current research processes for AI data interpretationData Generation (a): Obtaining paired slices of colon cancer cell blocks, performing H&E staining (routine pathological detection) and p53 IHC staining (tumor suppressor gene, can serve as a biomarker related to ADC efficacy); the dataset includes 5 pairs of non-cancerous tissues, 5 pairs of cancerous tissues (training set), and 22 pairs of cancerous tissues (test set), ensuring coverage of normal and tumor states.Dataset Construction and Preprocessing (b): Normalizing H&E images (eliminating staining differences) and aligning p53 IHC images with corresponding H&E images (ensuring spatial consistency), laying the foundation for subsequent annotations.Model Training (c): Annotating H&E images based on p53 IHC staining results (e.g., p53 positive regions corresponding to specific morphologies in H&E), and segmenting H&E images into thousands of small tiles; using convolutional neural networks (CNN) to train the model, learning the association between H&E image morphological features and p53 expression.Prediction and Reconstruction (d): Normalizing and segmenting new H&E slices (not stained for p53 IHC), using the trained CNN to predict the p53 expression status of each tile, ultimately reconstructing the p53 expression map of the entire slice. Research (Nature Machine Intelligence) shows that this AI model can predict multiple IHC markers (e.g., p53, HER2, TROP2) from routine H&E slices without additional IHC staining, significantly accelerating the biomarker analysis process and reducing costs. In breast cancer, this technology can predict the expression of HER2, TROP2, and other ADC target antigens through preoperative puncture H&E slices, avoiding the need for repeat biopsies; at the same time, for HER2-low breast cancer, AI analysis of H&E images can supplement IHC results, improving detection accuracy.
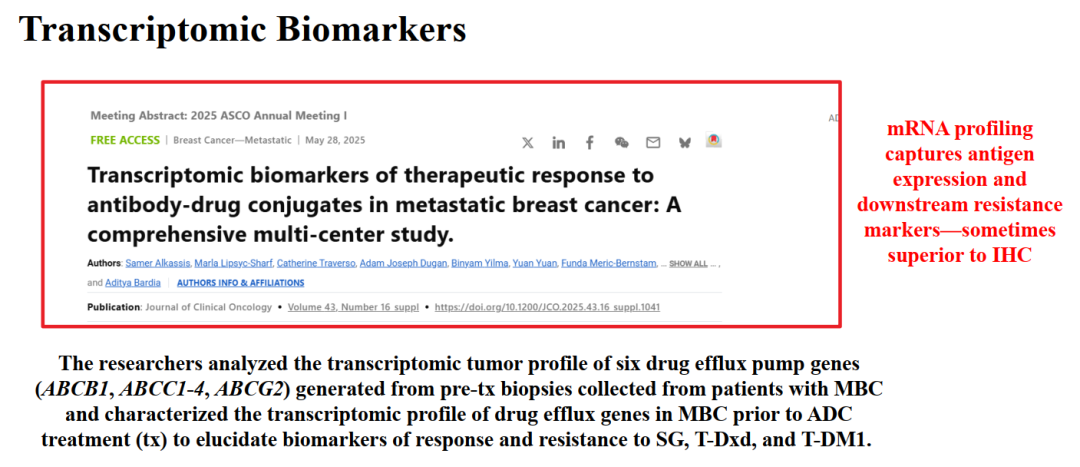
Current research processes for AI data interpretationData Generation (a): Obtaining paired slices of colon cancer cell blocks, performing H&E staining (routine pathological detection) and p53 IHC staining (tumor suppressor gene, can serve as a biomarker related to ADC efficacy); the dataset includes 5 pairs of non-cancerous tissues, 5 pairs of cancerous tissues (training set), and 22 pairs of cancerous tissues (test set), ensuring coverage of normal and tumor states.Dataset Construction and Preprocessing (b): Normalizing H&E images (eliminating staining differences) and aligning p53 IHC images with corresponding H&E images (ensuring spatial consistency), laying the foundation for subsequent annotations.Model Training (c): Annotating H&E images based on p53 IHC staining results (e.g., p53 positive regions corresponding to specific morphologies in H&E), and segmenting H&E images into thousands of small tiles; using convolutional neural networks (CNN) to train the model, learning the association between H&E image morphological features and p53 expression.Prediction and Reconstruction (d): Normalizing and segmenting new H&E slices (not stained for p53 IHC), using the trained CNN to predict the p53 expression status of each tile, ultimately reconstructing the p53 expression map of the entire slice. Research (Nature Machine Intelligence) shows that this AI model can predict multiple IHC markers (e.g., p53, HER2, TROP2) from routine H&E slices without additional IHC staining, significantly accelerating the biomarker analysis process and reducing costs. In breast cancer, this technology can predict the expression of HER2, TROP2, and other ADC target antigens through preoperative puncture H&E slices, avoiding the need for repeat biopsies; at the same time, for HER2-low breast cancer, AI analysis of H&E images can supplement IHC results, improving detection accuracy.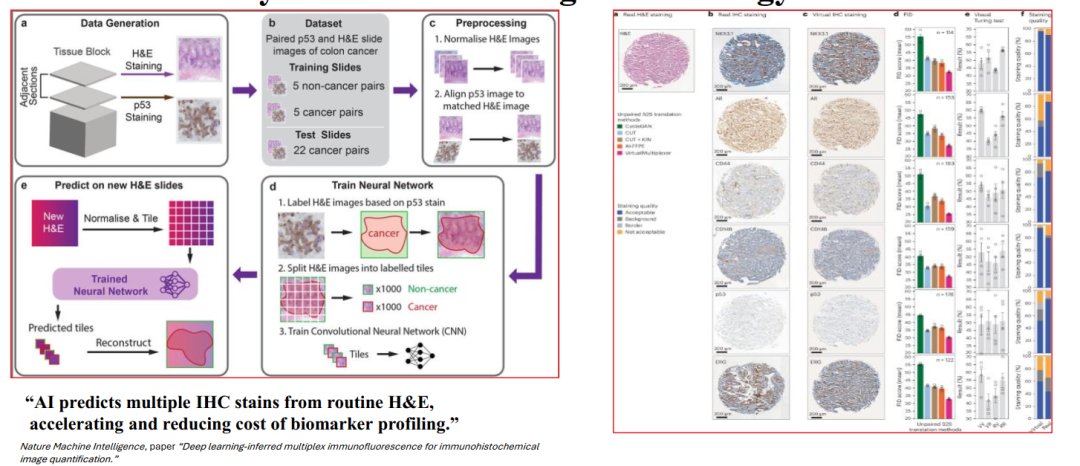 Transcriptomic biomarkers of metastatic breast cancer (MBC) efficacy and resistance to ADCs fill the limitations of IHC “only detecting protein expression.” Research design: Including MBC patients, collecting tumor biopsy samples before ADC treatment, analyzing the transcriptomic profiles of six drug efflux pump genes (ABCB1, ABCC1-4, ABCG2) — these genes encode proteins that can pump ADC payloads (e.g., MMAE, DM1) out of cancer cells, leading to insufficient drug accumulation, a key mechanism of ADC resistance. The aim of the study is to clarify the association between the expression levels of these genes and the efficacy of three core ADCs (Sacituzumab govitecan/SG, Trastuzumab deruxtecan/T-DXd, Trastuzumab emtansine/T-DM1).Core conclusions:
Transcriptomic biomarkers of metastatic breast cancer (MBC) efficacy and resistance to ADCs fill the limitations of IHC “only detecting protein expression.” Research design: Including MBC patients, collecting tumor biopsy samples before ADC treatment, analyzing the transcriptomic profiles of six drug efflux pump genes (ABCB1, ABCC1-4, ABCG2) — these genes encode proteins that can pump ADC payloads (e.g., MMAE, DM1) out of cancer cells, leading to insufficient drug accumulation, a key mechanism of ADC resistance. The aim of the study is to clarify the association between the expression levels of these genes and the efficacy of three core ADCs (Sacituzumab govitecan/SG, Trastuzumab deruxtecan/T-DXd, Trastuzumab emtansine/T-DM1).Core conclusions:
- High expression of drug efflux pump genes (e.g., high expression of ABCB1) is significantly associated with resistance to T-DM1, while having a smaller impact on T-DXd (possibly due to T-DXd’s high membrane permeability and bystander effect);
- High expression of ABCC3 is associated with resistance to SG in triple-negative breast cancer, serving as a negative predictive factor for SG efficacy;
- Transcriptomic profiles can simultaneously capture target antigen expression (e.g., HER2 mRNA levels) and downstream resistance markers (e.g., efflux pump genes), with predictive value superior to standalone IHC (e.g., HER2 IHC cannot distinguish between “HER2 positive but high efflux pump expression” resistant patients).
 Accelerating target screening and drug design for breast cancer ADCs through multi-omics integration and AI models addresses the low efficiency of traditional R&D.
Accelerating target screening and drug design for breast cancer ADCs through multi-omics integration and AI models addresses the low efficiency of traditional R&D.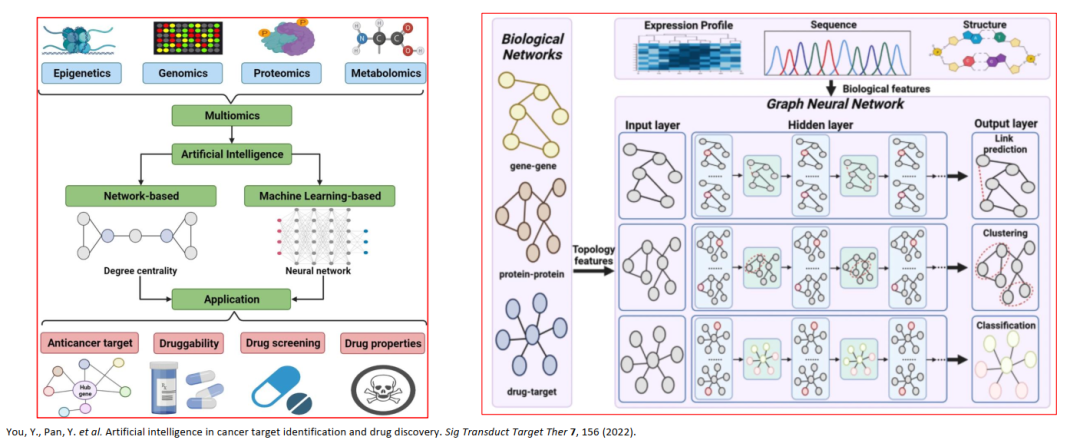 “Monitoring Treatment Response,” through a multi-dimensional strategy of “tissue detection + liquid biopsy + molecular imaging,” assesses the efficacy and resistance of breast cancer ADCs in real-time, achieving precise management of “dynamic adjustment of treatment plans.”Before treatment: ctDNA genotype-guided selection: By detecting tumor mutations (e.g., PIK3CA mutations, ESR1 mutations, BRCA1/2 mutations) through ctDNA, corresponding ADCs or combination plans can be matched — for example, HER2-positive breast cancer with PIK3CA mutations can choose T-DXd combined with PI3K inhibitors; MSI-H (microsatellite instability-high) triple-negative breast cancer can choose ADC combined with PD-1 inhibitors (e.g., Pembrolizumab).During treatment: Monitoring ctDNA dynamics combined with imaging: ctDNA dynamics: Regularly detecting the abundance of target antigen-related mutations (e.g., HER2 mutations) in ctDNA during treatment — a decrease in abundance indicates good efficacy, while an increase (e.g., a 10-fold increase in HER2 mutation abundance after two cycles of treatment) suggests resistance, requiring timely adjustments (e.g., switching to bispecific ADC); Molecular imaging: For instance, PET-CT assesses tumor metabolic activity (decrease in SUV value), supplementing changes in tumor burden that ctDNA cannot reflect (e.g., bone metastases may be radiologically stable but ctDNA has decreased, indicating that efficacy can still be maintained). Tissue detection supplementation: For patients with negative ctDNA detection or unclear efficacy, puncture biopsies can be performed for IHC/ISH (e.g., reassessing HER2 expression), NGS (detecting new resistance mutations), spatial omics (analyzing tumor microenvironment cell composition), clarifying resistance mechanisms (e.g., loss of target antigens, amplification of efflux pump genes). The text emphasizes the core advantages of liquid biopsy (ctDNA/CTCs) — real-time, minimally invasive, repeatable, overcoming the limitations of traditional tissue biopsies being “static, invasive, and unable to cover multiple lesions.” In breast cancer ADC therapy, this monitoring strategy can achieve: early detection of HER2 mutation resistance during T-DXd treatment, timely switching to B7-H3 ADC; monitoring TROP2 expression changes through ctDNA during SG treatment, avoiding ineffective treatments. This pushes breast cancer ADC therapy into a new era of “dynamic monitoring and adaptive adjustments.”
“Monitoring Treatment Response,” through a multi-dimensional strategy of “tissue detection + liquid biopsy + molecular imaging,” assesses the efficacy and resistance of breast cancer ADCs in real-time, achieving precise management of “dynamic adjustment of treatment plans.”Before treatment: ctDNA genotype-guided selection: By detecting tumor mutations (e.g., PIK3CA mutations, ESR1 mutations, BRCA1/2 mutations) through ctDNA, corresponding ADCs or combination plans can be matched — for example, HER2-positive breast cancer with PIK3CA mutations can choose T-DXd combined with PI3K inhibitors; MSI-H (microsatellite instability-high) triple-negative breast cancer can choose ADC combined with PD-1 inhibitors (e.g., Pembrolizumab).During treatment: Monitoring ctDNA dynamics combined with imaging: ctDNA dynamics: Regularly detecting the abundance of target antigen-related mutations (e.g., HER2 mutations) in ctDNA during treatment — a decrease in abundance indicates good efficacy, while an increase (e.g., a 10-fold increase in HER2 mutation abundance after two cycles of treatment) suggests resistance, requiring timely adjustments (e.g., switching to bispecific ADC); Molecular imaging: For instance, PET-CT assesses tumor metabolic activity (decrease in SUV value), supplementing changes in tumor burden that ctDNA cannot reflect (e.g., bone metastases may be radiologically stable but ctDNA has decreased, indicating that efficacy can still be maintained). Tissue detection supplementation: For patients with negative ctDNA detection or unclear efficacy, puncture biopsies can be performed for IHC/ISH (e.g., reassessing HER2 expression), NGS (detecting new resistance mutations), spatial omics (analyzing tumor microenvironment cell composition), clarifying resistance mechanisms (e.g., loss of target antigens, amplification of efflux pump genes). The text emphasizes the core advantages of liquid biopsy (ctDNA/CTCs) — real-time, minimally invasive, repeatable, overcoming the limitations of traditional tissue biopsies being “static, invasive, and unable to cover multiple lesions.” In breast cancer ADC therapy, this monitoring strategy can achieve: early detection of HER2 mutation resistance during T-DXd treatment, timely switching to B7-H3 ADC; monitoring TROP2 expression changes through ctDNA during SG treatment, avoiding ineffective treatments. This pushes breast cancer ADC therapy into a new era of “dynamic monitoring and adaptive adjustments.”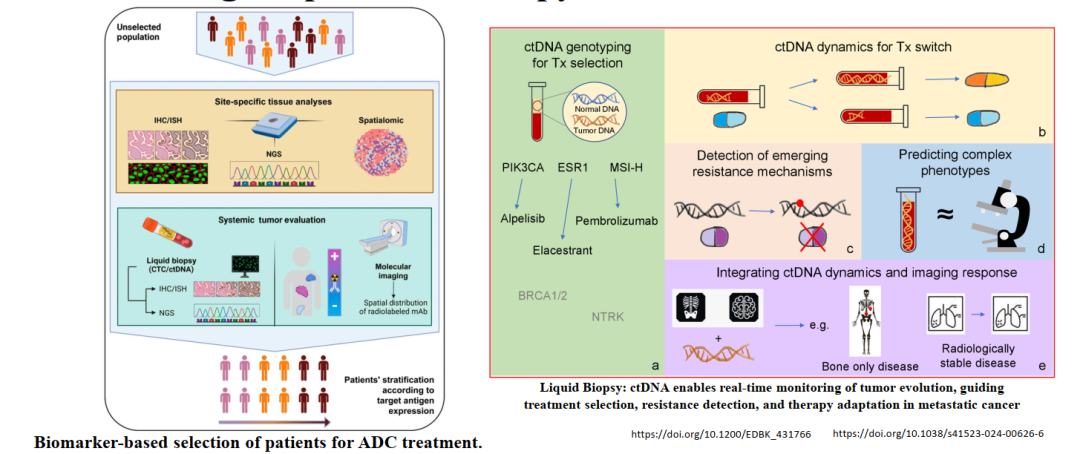 Four major challenges in the field of ADC biomarkers, which directly restrict the precise application of breast cancer ADCs, need targeted solutions.IHC Limitations: Even with the emergence of new technologies, IHC still faces two core issues — high inter-observer variability (e.g., different pathologists’ consistency in interpreting HER2 2+ is only 60%-70%) and lack of continuous quantification (only providing semi-quantitative results of 0/1+/2+/3+, unable to distinguish between “high expression in HER2 1+” and “low expression in HER2 1+”). In breast cancer, this leads to differences in screening HER2-low patients, with some patients who may benefit from T-DXd missing opportunities due to IHC misclassification.Validation Gaps: Many new biomarkers (e.g., drug efflux pump genes, AI digital pathology scores) perform better than traditional IHC in small-scale pilot studies but lack large-scale prospective validation — for example, an AI model predicted T-DXd efficacy in single-center HER2-low breast cancer with an AUC of 0.85, but in multi-center trials, the AUC dropped to 0.72, indicating the need for harmonization validation across tumor types (e.g., different breast cancer subtypes) and populations (e.g., different ethnicities) to ensure the universality of biomarkers.Complex Biology and Pharmacokinetics (PK): ADCs exist in three forms in the body — intact ADCs, naked antibodies (antibodies separated from payloads), and free payloads, with dynamic changes in the proportions of these three forms, and their different impacts on the biomarker-efficacy relationship (e.g., excessively high concentrations of free payloads may lead to toxicity, unrelated to target antigen expression). This heterogeneity leads to: inability to fully explain efficacy differences through a single biomarker (e.g., HER2 expression); difficulties in dose selection (e.g., some patients may need to reduce doses to minimize free payload toxicity, but this may affect the efficacy of intact ADCs).Clinical Translation Speed: The regulatory approval of AI-derived biomarkers (e.g., AI digital pathology scores) lags behind technological innovation — for instance, an AI model published clinical data in 2022 but still has not received FDA/EMA approval for clinical practice by 2025, mainly due to strict requirements from regulatory agencies regarding the “explainability” and “stability” of AI models, leading to lengthy approval processes. This delays breast cancer clinicians from timely applying new biomarkers to guide ADC therapy, hindering the implementation of precision medicine. These challenges outline clear targets for subsequent “future directions,” promoting the development of ADC biomarkers towards “standardization, verifiability, and rapid translation.” “2025 WCLC / Global Latest Data: Redefining Biomarkers for New ADCs,” although the conference focuses on lung cancer, the design concepts and clinical data of new ADCs have significant implications for the field of breast cancer ADCs, especially in “target expansion,” “mechanism innovation,” and “resistance response.”New ADC Targets and Drugs: ADCs announced at the 2025 WCLC include DLL3 target (IDE849), B7-H3 target (Ifinatamab deruxtecan, HS-20093), PD-L1 target (HLX43), EGFR/HER3 dual targets (Izalontamab brengitecan, DB-1310), and multi-target/dual payload ADCs. Among them, B7-H3 is highly expressed in breast cancer (especially triple-negative breast cancer), and Ifinatamab deruxtecan (B7-H3 ADC) shows anti-tumor activity (ORR about 40%) in small cell lung cancer/non-small cell lung cancer, indicating its potential in breast cancer; PD-L1 ADC HLX43 combines “immune checkpoint blockade (PD-L1 inhibition)” with “cytotoxic payload,” achieving an ORR of 35% in lung cancer patients resistant to PD-1/L1 monoclonal antibodies, which can be transferred to PD-1/L1 resistant triple-negative breast cancer, addressing the issue of immune therapy resistance.Breakthroughs in Bispecific ADCs: DLL3×B7-H3 bispecific ADC targets two antigens simultaneously, addressing tumor heterogeneity — for instance, some lesions in lung cancer highly express DLL3, while others highly express B7-H3, and bispecific ADCs can cover both; this idea can be directly applied to breast cancer, such as HER2×TROP2 bispecific ADC covering HER2-low and TROP2 high-expressing breast cancer, expanding the treatment population.Redefining Biomarkers: Clinical data from these new ADCs indicate that biomarkers are no longer limited to “single antigen expression,” but extend to “target combinations (e.g., co-expression of DLL3+B7-H3),” “immune status (e.g., PD-L1 expression + TMB),” and “resistance mutations (e.g., PD-L1 mutations),” for example, the efficacy of HLX43 is related to PD-L1 expression levels (TC≥1%) and the absence of PD-L1 resistance mutations. This provides a new direction for the development of breast cancer ADC biomarkers — for instance, the selection of ADCs for triple-negative breast cancer needs to assess B7-H3 expression, PD-L1 status, and ctDNA resistance mutations simultaneously. “Future Directions for ADC Biomarkers and Treatment,” revolves around four core aspects: “precision, real-time, standardization, and collaboration.”Multimodal Predictive Strategies: Integrating traditional IHC (e.g., HER2 expression), AI/digital pathology (e.g., TROP2 quantitative scoring), molecular profiles (e.g., drug efflux pump gene expression), and advanced imaging (e.g., PET-CT target antigen probes) to construct multi-dimensional predictive models.Real-time Adaptive Monitoring: Utilizing ctDNA, CTCs, and digital biomarkers (e.g., concentration of free ADC payloads in blood) to dynamically monitor tumor evolution.Standardization and Automation: Developing AI-driven biomarker scoring systems (e.g., globally unified HER2-low AI scoring standards) and computational models (e.g., ADC dose prediction models) to address detection differences between laboratories.Collaborative Paradigm Shift: Promoting multidisciplinary collaboration among pathology (interpreting IHC/digital pathology), bioinformatics (analyzing multi-omics data), oncology (developing treatment plans), and pharmacy (optimizing ADC doses), establishing a closed loop from biomarker detection to treatment implementation.
Four major challenges in the field of ADC biomarkers, which directly restrict the precise application of breast cancer ADCs, need targeted solutions.IHC Limitations: Even with the emergence of new technologies, IHC still faces two core issues — high inter-observer variability (e.g., different pathologists’ consistency in interpreting HER2 2+ is only 60%-70%) and lack of continuous quantification (only providing semi-quantitative results of 0/1+/2+/3+, unable to distinguish between “high expression in HER2 1+” and “low expression in HER2 1+”). In breast cancer, this leads to differences in screening HER2-low patients, with some patients who may benefit from T-DXd missing opportunities due to IHC misclassification.Validation Gaps: Many new biomarkers (e.g., drug efflux pump genes, AI digital pathology scores) perform better than traditional IHC in small-scale pilot studies but lack large-scale prospective validation — for example, an AI model predicted T-DXd efficacy in single-center HER2-low breast cancer with an AUC of 0.85, but in multi-center trials, the AUC dropped to 0.72, indicating the need for harmonization validation across tumor types (e.g., different breast cancer subtypes) and populations (e.g., different ethnicities) to ensure the universality of biomarkers.Complex Biology and Pharmacokinetics (PK): ADCs exist in three forms in the body — intact ADCs, naked antibodies (antibodies separated from payloads), and free payloads, with dynamic changes in the proportions of these three forms, and their different impacts on the biomarker-efficacy relationship (e.g., excessively high concentrations of free payloads may lead to toxicity, unrelated to target antigen expression). This heterogeneity leads to: inability to fully explain efficacy differences through a single biomarker (e.g., HER2 expression); difficulties in dose selection (e.g., some patients may need to reduce doses to minimize free payload toxicity, but this may affect the efficacy of intact ADCs).Clinical Translation Speed: The regulatory approval of AI-derived biomarkers (e.g., AI digital pathology scores) lags behind technological innovation — for instance, an AI model published clinical data in 2022 but still has not received FDA/EMA approval for clinical practice by 2025, mainly due to strict requirements from regulatory agencies regarding the “explainability” and “stability” of AI models, leading to lengthy approval processes. This delays breast cancer clinicians from timely applying new biomarkers to guide ADC therapy, hindering the implementation of precision medicine. These challenges outline clear targets for subsequent “future directions,” promoting the development of ADC biomarkers towards “standardization, verifiability, and rapid translation.” “2025 WCLC / Global Latest Data: Redefining Biomarkers for New ADCs,” although the conference focuses on lung cancer, the design concepts and clinical data of new ADCs have significant implications for the field of breast cancer ADCs, especially in “target expansion,” “mechanism innovation,” and “resistance response.”New ADC Targets and Drugs: ADCs announced at the 2025 WCLC include DLL3 target (IDE849), B7-H3 target (Ifinatamab deruxtecan, HS-20093), PD-L1 target (HLX43), EGFR/HER3 dual targets (Izalontamab brengitecan, DB-1310), and multi-target/dual payload ADCs. Among them, B7-H3 is highly expressed in breast cancer (especially triple-negative breast cancer), and Ifinatamab deruxtecan (B7-H3 ADC) shows anti-tumor activity (ORR about 40%) in small cell lung cancer/non-small cell lung cancer, indicating its potential in breast cancer; PD-L1 ADC HLX43 combines “immune checkpoint blockade (PD-L1 inhibition)” with “cytotoxic payload,” achieving an ORR of 35% in lung cancer patients resistant to PD-1/L1 monoclonal antibodies, which can be transferred to PD-1/L1 resistant triple-negative breast cancer, addressing the issue of immune therapy resistance.Breakthroughs in Bispecific ADCs: DLL3×B7-H3 bispecific ADC targets two antigens simultaneously, addressing tumor heterogeneity — for instance, some lesions in lung cancer highly express DLL3, while others highly express B7-H3, and bispecific ADCs can cover both; this idea can be directly applied to breast cancer, such as HER2×TROP2 bispecific ADC covering HER2-low and TROP2 high-expressing breast cancer, expanding the treatment population.Redefining Biomarkers: Clinical data from these new ADCs indicate that biomarkers are no longer limited to “single antigen expression,” but extend to “target combinations (e.g., co-expression of DLL3+B7-H3),” “immune status (e.g., PD-L1 expression + TMB),” and “resistance mutations (e.g., PD-L1 mutations),” for example, the efficacy of HLX43 is related to PD-L1 expression levels (TC≥1%) and the absence of PD-L1 resistance mutations. This provides a new direction for the development of breast cancer ADC biomarkers — for instance, the selection of ADCs for triple-negative breast cancer needs to assess B7-H3 expression, PD-L1 status, and ctDNA resistance mutations simultaneously. “Future Directions for ADC Biomarkers and Treatment,” revolves around four core aspects: “precision, real-time, standardization, and collaboration.”Multimodal Predictive Strategies: Integrating traditional IHC (e.g., HER2 expression), AI/digital pathology (e.g., TROP2 quantitative scoring), molecular profiles (e.g., drug efflux pump gene expression), and advanced imaging (e.g., PET-CT target antigen probes) to construct multi-dimensional predictive models.Real-time Adaptive Monitoring: Utilizing ctDNA, CTCs, and digital biomarkers (e.g., concentration of free ADC payloads in blood) to dynamically monitor tumor evolution.Standardization and Automation: Developing AI-driven biomarker scoring systems (e.g., globally unified HER2-low AI scoring standards) and computational models (e.g., ADC dose prediction models) to address detection differences between laboratories.Collaborative Paradigm Shift: Promoting multidisciplinary collaboration among pathology (interpreting IHC/digital pathology), bioinformatics (analyzing multi-omics data), oncology (developing treatment plans), and pharmacy (optimizing ADC doses), establishing a closed loop from biomarker detection to treatment implementation.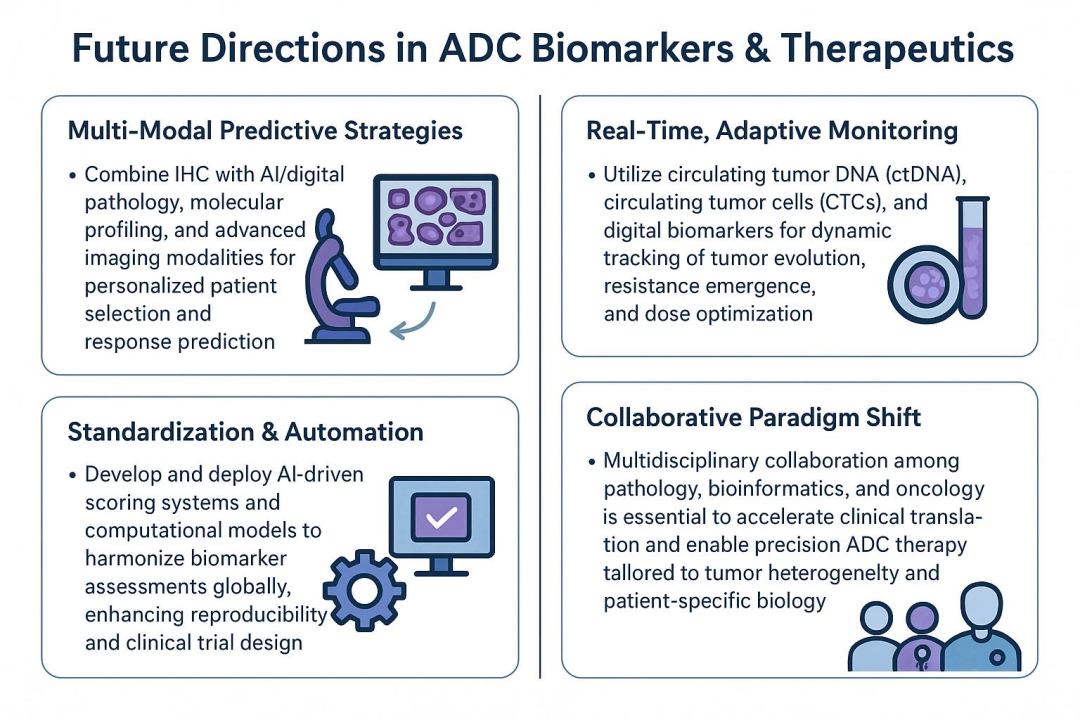 Clinical Case 1 (Case 1), “Biomarker Assessment Before and After T-DXd Treatment”Treatment of Lung Cancer with ERBB Mutations
Clinical Case 1 (Case 1), “Biomarker Assessment Before and After T-DXd Treatment”Treatment of Lung Cancer with ERBB Mutations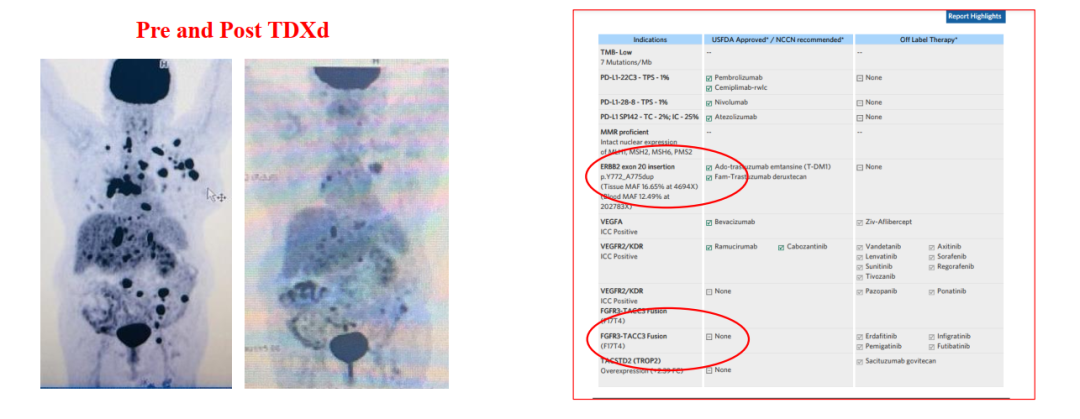 Case 2: Biomarker testing results clearly identify B7-H3 as a core target, recommending clinical trials targeting B7-H3.
Case 2: Biomarker testing results clearly identify B7-H3 as a core target, recommending clinical trials targeting B7-H3.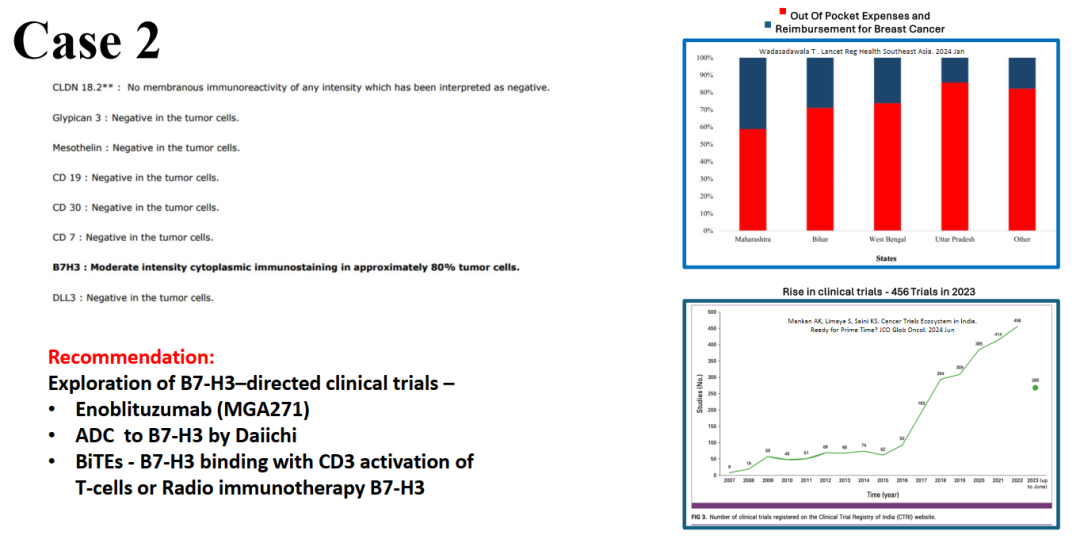 Finally, a comprehensive conclusion was made using the speaker’s hospital’s precision treatment.
Finally, a comprehensive conclusion was made using the speaker’s hospital’s precision treatment.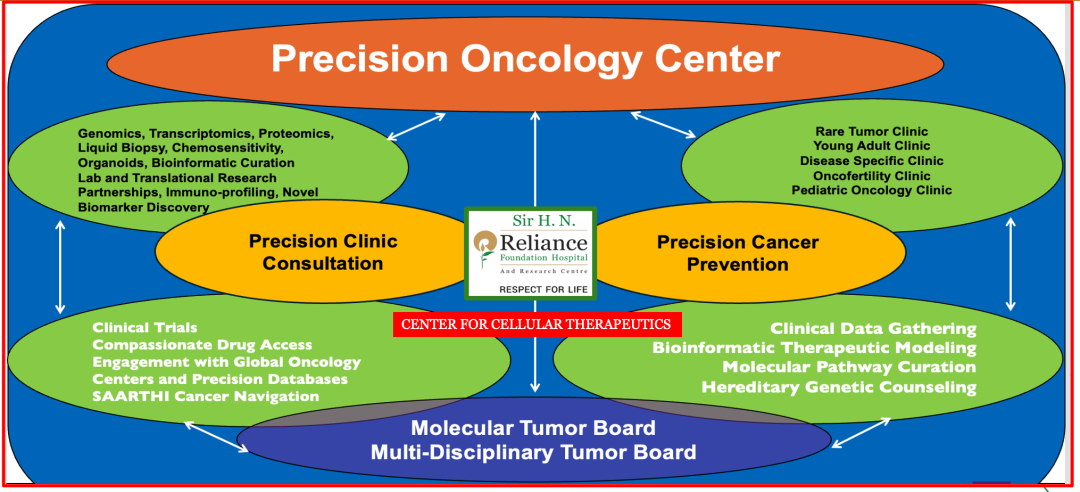 Since the chemotherapy era, biomarkers have been very important in tumor treatment, but since the chemotherapy era, there have been almost no biomarkers that can predict efficacy with 100% certainty, making patient treatment somewhat like opening a blind box. With the development of technological means and the improvement of big data processing capabilities, patient information is being used in a multidimensional way to judge subsequent efficacy and prognosis.Source:https://wclc.iaslc.org/
Since the chemotherapy era, biomarkers have been very important in tumor treatment, but since the chemotherapy era, there have been almost no biomarkers that can predict efficacy with 100% certainty, making patient treatment somewhat like opening a blind box. With the development of technological means and the improvement of big data processing capabilities, patient information is being used in a multidimensional way to judge subsequent efficacy and prognosis.Source:https://wclc.iaslc.org/