The tumor distribution of ADCs depends on many factors, includingthe dose itself, systemic clearance rate, antigen expression level, endocytosis rate, and the tumor’s surface area to volume ratio (S/V). Poor tissue permeability remains a major challenge for antibody treatments of solid tumors, and appropriately increasing the dosage can improve the drug’s tissue distribution and enhance tumor penetration. However, for ADCs, due to the dose-limiting toxicity of small molecule payloads, the administration dose is lower compared to their parent antibodies, further reducing tumor penetration. So far, the most successful ADCEnhertu has a dose of about 5.4 mpk due to its moderate toxicity payload, which is very close to its parent antibody Herceptin’s 6 mpk dose. However, for those using MMAE or other more toxic payloads, the side effects from increasing the dose become unacceptable. Adjusting the administration strategy can expand the therapeutic window of ADCs and improve their therapeutic effects, for example, the first ADC drugMylotarg reduces toxicity and improves tolerance by administering lower doses at higher frequencies, such as reducing thrombocytopenia and liver function abnormalities. Although reducing the dose and increasing the administration frequency can improve tolerance,for solid tumors, lower plasma concentrations can lead to decreased drug penetration in the tumor, thereby affecting therapeutic efficacy. Moreover, intra-tumor drug distribution remains unknown, as changing administration strategies is usually only measured from plasma, which may not reflect intra-tumor drug levels. Another administration strategy is to co-administernaked antibodies with ADCs to improve ADC distribution within the tumor.
01
Preclinical Data
In preclinical studies, when trastuzumab and therapeutic dose T-DM1 were administered to tumor mice at ratios of 0:1, 3:1, and 8:1, T-DM1 penetrated beyond the perivascular area into tumor regions further from the blood vessels, and the improved permeability also brought about better efficacy.
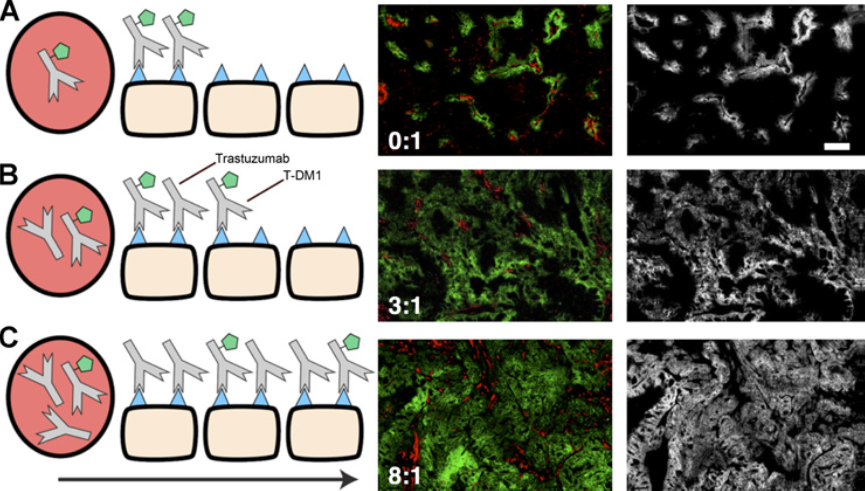
Figure 1: Tumor distribution of T-DM1 at different doses of naked antibody
As shown in Figure 1A, with a single injection of 3.6 mg/kg of T-DM1, most of the ADC was bound at the tumor surface, leading to severely insufficient tumor penetration. However, in B and C, simultaneous injection of 10.8 mg/kg or 28.8 mg/kg of trastuzumab greatly increased the distribution and uniformity of the drug within the tumor.
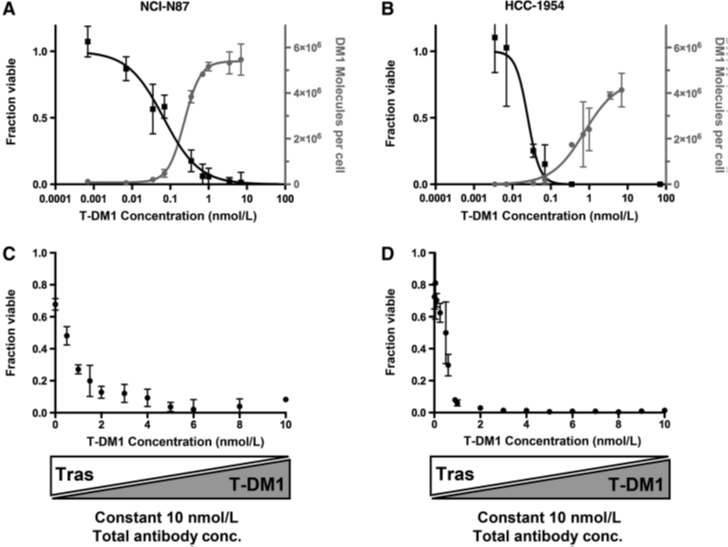
Figure 2: Cytotoxicity after mixing different doses of naked antibody with T-DM1
Increasing the dose of trastuzumab improved the permeability of T-DM1 to tumor tissue, but due to competition with HER2 receptors, it reduced the number of DM1 delivered to individual cells. The question arises, does T-DM1 mixed with naked antibody still have sufficient killing ability against tumors? Literature reports that the NCI-N87 cell line is sensitive to T-DM1, while trastuzumab has only a slight growth inhibitory effect in vitro. As shown in Figure 2, the IC50 values for the NCI-N87 and HCC1954 cell lines are 82 and 33 pmol/L, respectively, with the overall concentration of naked antibody and ADC controlled at 10 nmol/L(relative to the saturation concentration of the antigen), and after adding trastuzumab, the toxicity of T-DM1 to both cell lines remains below the antibody Kd(1.8 nmol/L), although the IC50 may be higher due to competition from trastuzumab.
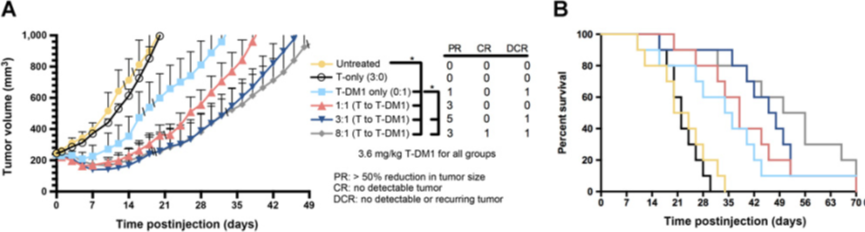
Figure 3: Mouse survival curves after mixing different doses of naked antibody with T-DM1
To study the impact ofADC tumor distribution on efficacy, a fixed dose(3.6 mg/kg) of T-DM1 and different ratios of trastuzumab were administered in an NCI-N87 tumor xenograft mouse model. The NCI-N87 cell line was chosen because it is less sensitive to T-DM1 than the HCC1954 cell line. The cell line’s sensitivity to T-DM1 in vitro and in vivo is relatively low, providing more room for detecting improvements in efficacy, and other experiments have shown that at moderate doses, such as those used in this study, trastuzumab treatment does not significantly change tumor growth. Trastuzumab treatment at higher doses(>60 mg/kg) produces moderate(but statistically significant) growth inhibition, but even at the highest dose of 280 mg/kg, no tumor reduction occurs within weeks. Adding trastuzumab to T-DM1 slows tumor growth at all dose levels compared to using T-DM1 alone, with the ratios of 3:1 and 8:1(T:T-DM1) having statistically significant effects. The 3:1 and 8:1 dose levels had several more PRs, and as the dose of trastuzumab increased, survival rates showed statistically significant increases. Moreover, animals receiving only trastuzumab were similar to the saline control group, indicating that trastuzumab had no direct effect on efficacy at these doses. During the study, the treated mice were weighed, showing comparable tolerance. The main source of toxicity comes from thepayload rather than the antibody dose. Since trastuzumab has much higher tolerance than T-DM1, and both were given the same T-DM1 dose, all treatments had consistent tolerability. During the study, the treated mice were weighed, showing comparable tolerability.02Clinical Data
Since mouse models cannot replicate the complexity of human tumors, the clinical utility of this administration strategy remains unknown. If this administration strategy works in human patients, given the dose-limiting toxicity of these drugs and the number of clinical trials for ADCs, it could have a significant impact on the development of ADCs.
An early-phase clinical trial(NCT02415881) provided a suitable dataset to test the preclinical hypothesis, that the dose of naked antibody can improve the antibody-dye (this clinical trial used dye for tracing) conjugate’s micro-distribution in a clinical environment. The primary outcome of this trial was predefined as the safety of panitumumab-IRDye800CW. In this, a retrospective analysis of the clinical trial was conducted to evaluate the combination therapy strategy in clinical settings. It was hypothesized that fluorescently labeled antibodies could be used as alternatives to measure ADCs’ intra-tumor distribution. The rationale is that as long as the fluorescent moiety or cytotoxic drug is appropriately conjugated(without significantly altering binding sites or physicochemical properties), it has minimal impact on the pharmacokinetics and tissue permeability of the antibody. This study indicates thatwhen co-administered with naked antibodies, the antibody-dye conjugate’s intra-tumor distribution is improved, while uptake in healthy tissues is lower, supporting the potential application of co-administration strategies for ADCs to expand their therapeutic window in clinical solid tumors.
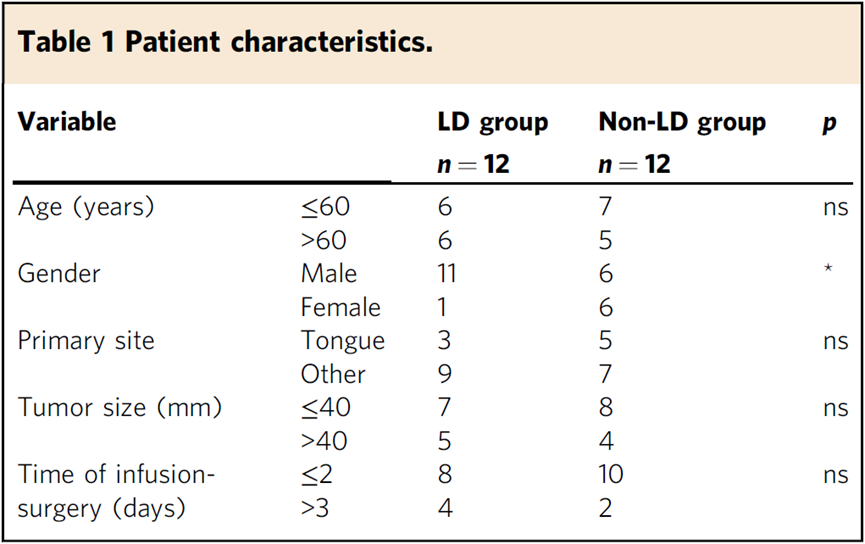
Table 1
Summary of study design. A single-center, non-randomized phase I study was conducted in 24 patients with head and neck squamous cell carcinoma (HNSCC), where the total dose of antibody received ranged from 0.3 mg kg-1 to 2.6 mg kg-1. Half of the patients received a loading dose of 100 mg unlabelled antibody. The table above summarizes patient characteristics. Patients’ ages at diagnosis ranged from 32 to 85 years(mean: 62 years), with most presenting with oral squamous cell carcinoma(88%). The average time from infusion to surgery was 2.5 days(range 1-5). There were no significant differences in age, primary tumor site, tumor size, and infusion-surgery time between patients receiving the loading dose(LD group) and those not receiving the loading dose(non-LD group). Fresh tumor samples, thick tissue sections(5 mm), and histological slices(5 microns) were used to measure Panitumab-IRDye800CW in the primary tumors. After surgical resection, fresh tissue samples were obtained from each patient, if available, to quantify antibody concentrations in these tissue samples. After formalin fixation, primary tumor specimens were sliced into 5 mm thick tissue sections for imaging using a closed-field fluorescence imaging system. Subsequently, thick tissue sections were paraffin-embedded into tissue blocks and then sliced into 5 microns thick sections(histological slices) for near-infrared microscopy imaging and histopathological evaluation(Hematoxylin and Eosin (H&E) slices). The antibody-dye absorption and distribution measured by fluorescence intensity and distribution were quantified fromthick tissue sections(macro imaging) andthin histological slices (microscopic imaging).
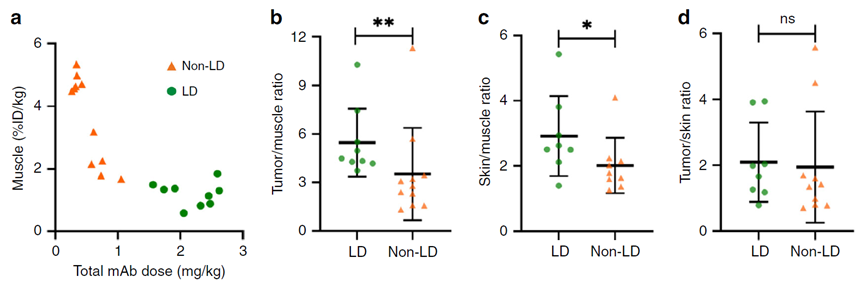
Figure 4: Co-administration with naked antibodies reduces muscle uptake while maintaining overall tumor uptake
As the total antibody dose increased from 0.3 mg kg-1 to 2.6 mg kg-1, muscle uptake of the antibody-dye conjugate showed a downward trend(Figure 4a), indicating that co-administered unlabelled antibodies saturate binding sites in muscle, thus reducing target-mediated uptake in healthy tissues. To avoid confounding influences from patient variability, the authors normalized muscle uptake against tumor and skin uptake, finding that patients receiving the loading dose had significantly increased tumor and skin uptake of the antibody dye(Figure 4b,c). When tumor uptake was normalized against skin uptake, no significant differences were observed between groups(Figure 4d). In summary, EGFR receptors were not saturated in either skin or tumor.
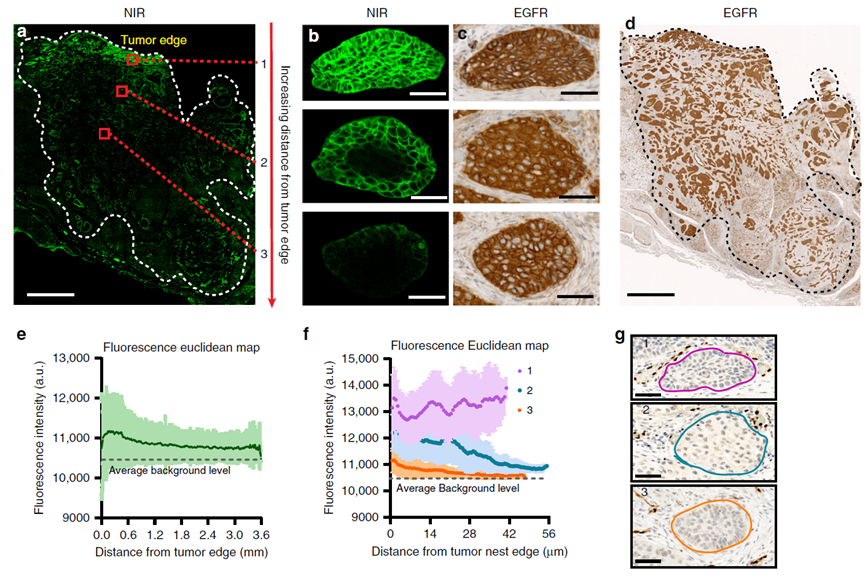
Figure 5: Antibody-dye conjugate distribution shows macro and micro heterogeneity within solid tumors
Sub-saturating doses of antibodies lead to heterogeneous distribution of antibody-dye conjugates throughout the tumor and within tumor nests under microscopy(Figure 5). In large tumors, although EGFR expression is uniform throughout the tumor(Figure 5d), the distribution of antibodies within the tumor is significantly lower than at the periphery(Figure 5a). The fluorescence intensity map(Figure 5e) shows that as tumor cells move further away from the edge of the tumor mass, the fluorescence intensity gradually decreases, which has previously been shown to correlate with higher vascular density and lower stromal density at the tumor periphery, as well as increased interstitial pressure within. Under microscopy, despite consistent EGFR expression, the distribution of antibodies within tumor nests is inconsistent(Figure 5b,c). The saturation of tumor nests depends on their position relative to the tumor edge. At sub-saturating doses(consistent with ADC doses), peripheral tumor nests show constant fluorescence intensity, while those located more centrally gradually weaken in fluorescence as the distance from the tumor edge increases(Figure 5f). On both micro and macro levels, the negative correlation between drug delivery and distance from the tumor edge indicates that antibodies first saturate receptors located at the periphery. Although the distribution is evidently heterogeneous, antibodies form a stagnation saturation zone in the tumor, commonly referred to as the “binding site barrier”.
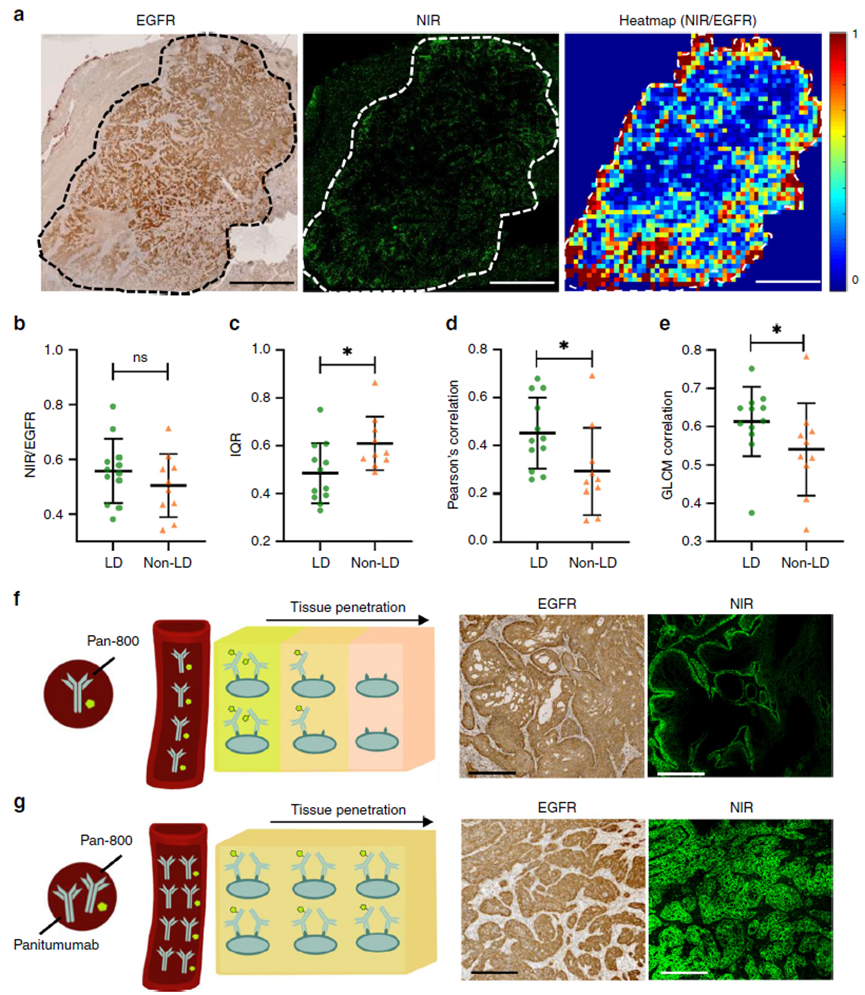
Figure 6: When used together with unlabelled antibodies, the spatial distribution of antibody-dye conjugates throughout the tumor is more uniform.
To quantitatively compare the antibody permeability of the two administration groups, each tumor was divided into small square regions, and the antibody permeability of each square region was measured, i.e., the ratio of near-infrared fluorescence positive areas to EGFR positive areas. The antibody permeability of the region, i.e., the ratio of near-infrared fluorescence positive areas to EGFR positive areas, was plotted in a heatmap to show its distribution(Figure 6a). When quantifying the overall antibody permeability, using the NIR to EGFR ratio of the entire tumor region, no differences were found between the LD and non-LD administration groups(Figure 6b). However, when considering micro-regional variations using square regions, patients receiving the loading dose had significantly lower interquartile ranges of region-based antibody permeability across the entire tumor compared to those in the non-LD group. The Pearson correlation between fluorescence and EGFR expression in square regions of each tumor was significantly higher in the LD group compared to the non-LD group(Figure 6c). Moreover, the antibody permeability in adjacent regions of tumors receiving the LD dose was significantly more correlated compared to those in the non-LD dose group(Figure 6e). All these indicators suggest a reduction in the heterogeneity of antibody distribution in the LD group. In Figure 6f, when only the antibody-dye conjugate was administered systemically: the antibody-dye leaks out from the blood vessels and diffuses into the extracellular space, binding to and saturating the cells outside. To the outer layer of cells in the tumor nests, saturating them, thus forming a stagnation saturation zone(i.e., “binding site barrier”). However, in Figure 6g, when the parent antibody is co-administered with the antibody-dye conjugate, the parent antibody dilutes the antibody-dye conjugate and competes for binding sites in the outer layer of tumor cells. Therefore, the antibody-dye conjugate can penetrate deeper into the tumor, overcoming the “binding site barrier”, leading to improved distribution of the antibody at the microscopic level.
Conclusion In a specific tumor area,the absorption of antibodies is driven by their vascular or permeable surfaces, while microscopic distribution depends onthe number of available binding sites for specific antibodies. Since the rate at which antibodies bind to targets is much faster than the rate of diffusion, their penetration into tumor tissue is severely limited(e.g., binding site barrier). This limits drug penetration into the tumor interior before antibodies reach saturation doses. Moreover, due to the toxicity brought by the toxins carried by ADCs(toxin shedding, non-specific endocytosis, or on-target, off-tumor toxicity), the doses are relatively lower compared to naked antibodies. By adding naked antibodies or more directly reducing DAR to increase the dose of ADC, using the “antibody sea tactics” to overcome the binding site barrier and enhance the tumor penetration of antibody drugs. Theoretically, if the antibody dose is large enough, antibodies will saturate all(accessible) binding sites within the tumor, achieving saturation both internally and externally.
For Roche’s two MUC16-targeting ADC’s phase I data, the first DMUC5754A has a DAR of about 3.5, with a phase I ORR of 17% at a dose of 2.4 mpk, while the Thiomab site-specific conjugated DMUC4064A achieved 5.2 mpk under DAR2 conditions(calculating that the delivered amount of MMAE does not change significantly), and the ORR also increased to 45%. Of course, different clinical data are not very suitable for direct comparison, and this is just a circumstantial evidence indicating that changes in drug distribution within the tumor due to antibody dosage may enhance the therapeutic effect and window of ADCs, especially when using relatively more toxic toxins like MMAE or even PBD, whether adopting methods to reduce DAR or incorporating naked antibodies in the indications for solid tumors can bring tangible clinical benefits is a question worth pondering.
References: Cornelius Cilliers, Bruna Menezes, et al. Improved Tumor Penetration and Single-Cell Targeting of Antibody–Drug Conjugates Increases Anticancer Efficacy and Host Survival. doi: 10.1158/0008-5472.CAN-17-1638
Guolan Lu, Naoki Nishio, et al. Co-administered antibody improves penetration of antibody–dye conjugate into human cancers with implications for antibody–drug conjugates. doi: 10.1038/s41467-020-19498-y
J. F. Liu, K. N. Moore, et al. Phase I study of safety and pharmacokinetics of the anti-MUC16 antibody–drug conjugate DMUC5754A in patients with platinum-resistant ovarian cancer or unresectable pancreatic cancer. doi:10.1093/annonc/mdw401
Disclaimer
“YaoDu” public account reprints articles from other public account platforms, mainly to share industry-related knowledge and convey the latest information. The images and articles are copyrighted by the original authors. If there is any infringement, please inform us in a timely manner, and we will delete the relevant information within 24 hours.