This article is compiled from Professor Song Zhengbo of Zhejiang Provincial Cancer Hospital.“Current Status and Development Challenges of ADC Drugs”.
Song Zhengbo
Doctor of Oncology, Associate Chief Physician, Associate Professor, Master’s Supervisor

More than 100 years ago, the father of immunology, Paul Ehrlich, first proposed the concept of “magic bullet,” which refers to selectively delivering toxic drugs to target cells while avoiding damage to normal human cells.
ADC, as a new type of anti-cancer drug, is formed by conjugating small molecule cytotoxins with monoclonal antibody molecules. It has targeting and killing effects and is leading a new era of targeted cancer therapy.
ADC drugs are likely to be the next trend in the treatment of NSCLC.
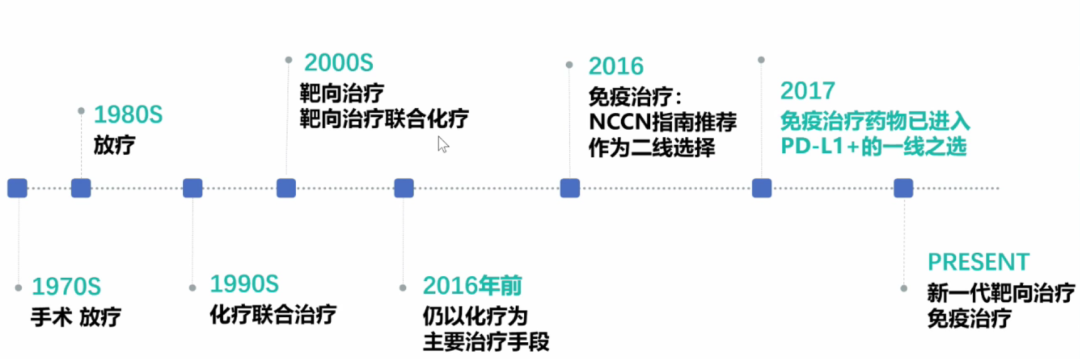
Development History of ADC Drugs
From the perspective of drug composition and technical characteristics, ADC drugs can be subdivided into three generations.
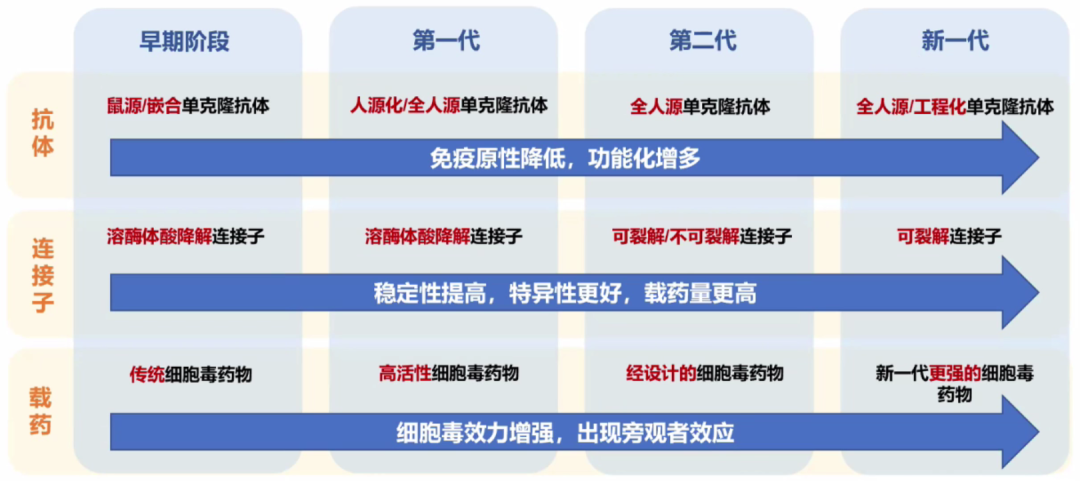
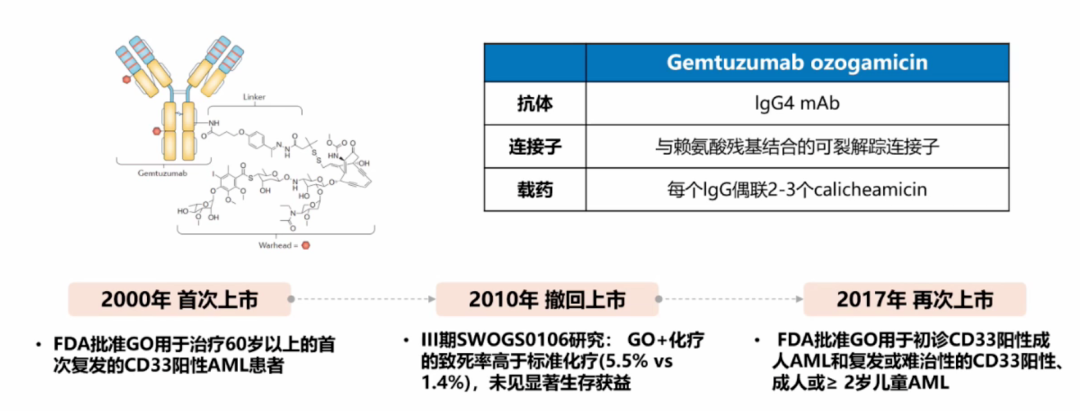
The path to market for the first generation of ADC drugs was full of twists and turns; it was first launched in 2000, withdrawn in 2010, and relaunched in 2017.
Its structure has significant limitations:
① High immunogenicity;
② The linker is unstable, leading to severe toxic reactions due to premature release of the toxin in plasma;
③ Insufficient potency of cytotoxic drugs.
The second generation of ADCs has undergone various structural optimizations but still has the following limitations:
① Heterogeneity of DAR, with a higher proportion of naked antibodies not conjugated to cytotoxins in circulation;
② Excessive drug-antibody conjugation can lead to antibody aggregation, accelerated clearance, and increased non-specific toxicity.
The next generation of ADCs has been comprehensively optimized, leading to improved clinical efficacy.
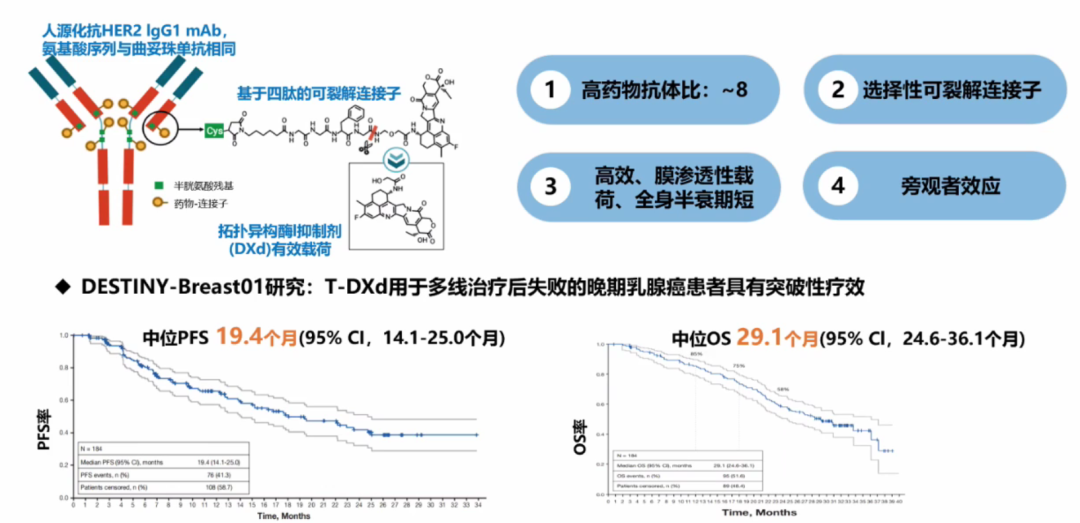
DS-8201, as a new generation star antibody-drug conjugate (ADC), demonstrated outstanding efficacy in the DESTINY-Breast01 study, making a stunning appearance at the San Antonio Breast Cancer Symposium (SABCS) twice. Its subgroup data indicate potential therapeutic benefits for patients with brain metastases, and subgroup analysis suggests that early-line treatment with DS-8201 may provide longer survival benefits for patients with HER2-positive advanced breast cancer.
Research results show mPFS of 19.4 months (95% CI, 14.1-25 months) and mOS of 29.1 months (95% CI, 24.6-36.1 months).
Currently, several ADC drugs have been approved for clinical use, involving hematological malignancies and solid tumors.

Four Core Elements of ADC Function
ADC consists of an antibody, an effective payload, and a chemical linker. An ideal ADC maintains stability in the blood circulation, accurately reaches the treatment target, and ultimately releases the cytotoxic payload near the target (e.g., cancer cells). Each element affects the final efficacy and safety of the ADC. Overall, the development of ADC requires consideration of all these key components, including targets, antibodies, cytotoxic payloads, linkers, and the choice of conjugation methods.
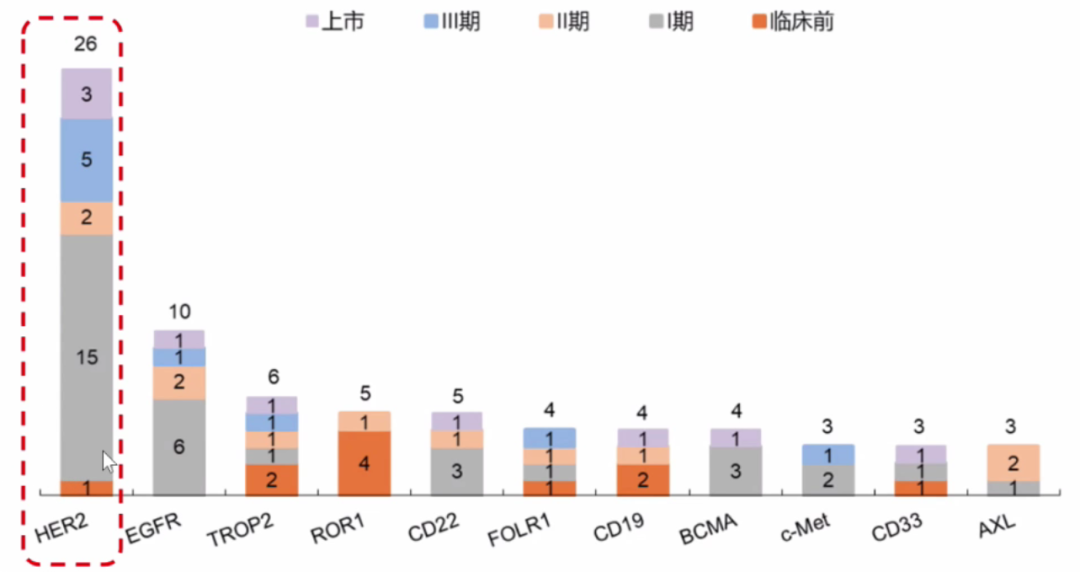
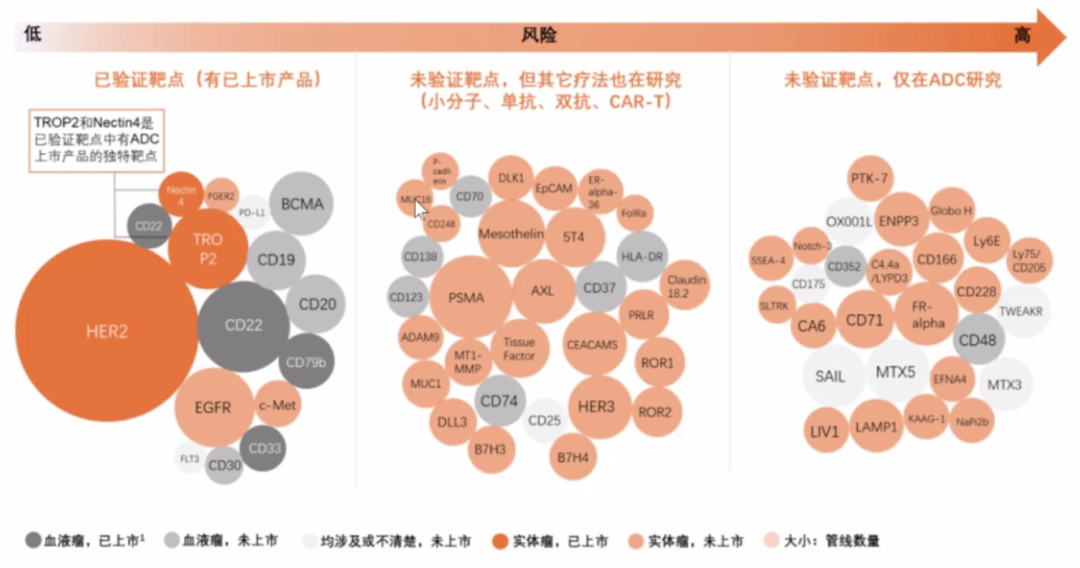
1. Suitable Target Antigen
High expression on the surface of tumor cells, relatively low or absent expression in normal tissues, such as CD138; avoid detachment from the target cell surface to prevent ADC from binding to antigens in circulation, reducing efficacy; upon binding with antibodies, it can trigger preferential ADC internalization, initiating the internalization pathway of the antibody-antigen complex into the cell.
Data shows that the most ADC drugs approved and in development target HER2, with a total of 26 products.
2. Highly Specific Antibodies
How to achieve an effect where 1+1>2 with antibodies is a basic requirement:
① High specificity for the antigen;
② High affinity between the antibody and the target antigen;
③ Minimal immunogenicity;
④ The antibody induces inherent anti-tumor activity by directly modulating the biological activity of the antigen.
3. Ideal Linker
The ADC linker connects the antibody and the effective payload and is key to the success of ADC development.
An ideal linker must possess three elements:
① After ADC is internalized into the target cell, the linker can effectively cleave and rapidly release the payload, which is a necessary condition for the drug to have a bystander effect;
② It must remain stable in plasma to avoid premature release of the payload that could damage normal tissues or cells;
③ Precise conjugation sites can control the location and DAR of high molecular weight drug molecules on the antibody, ensuring anti-tumor efficacy while maintaining drug homogeneity.
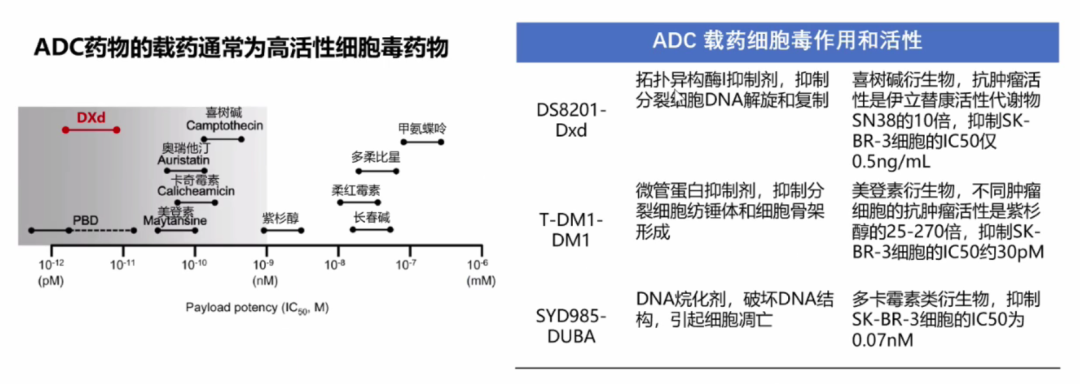
4. Highly Effective Cytotoxins
Clinical Applications of ADC
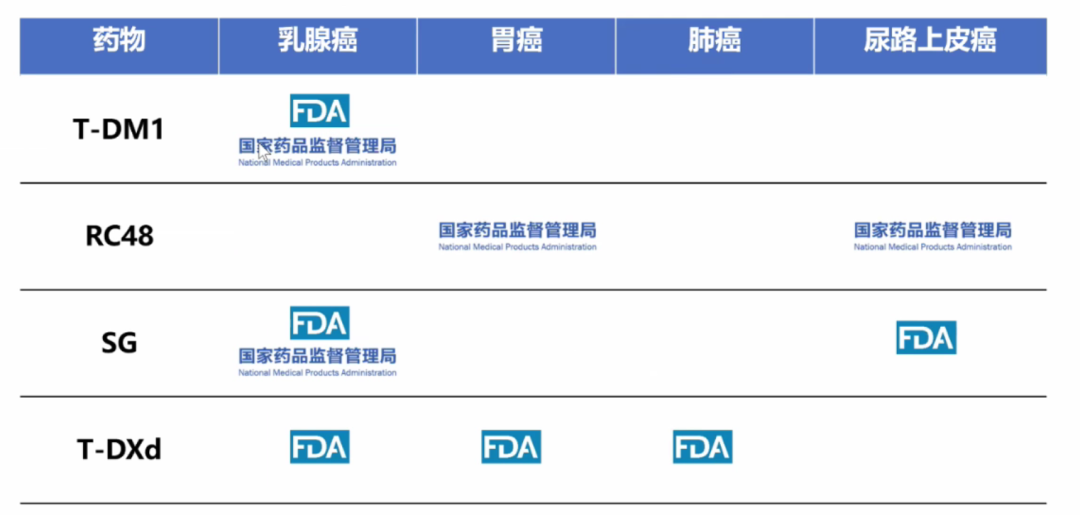
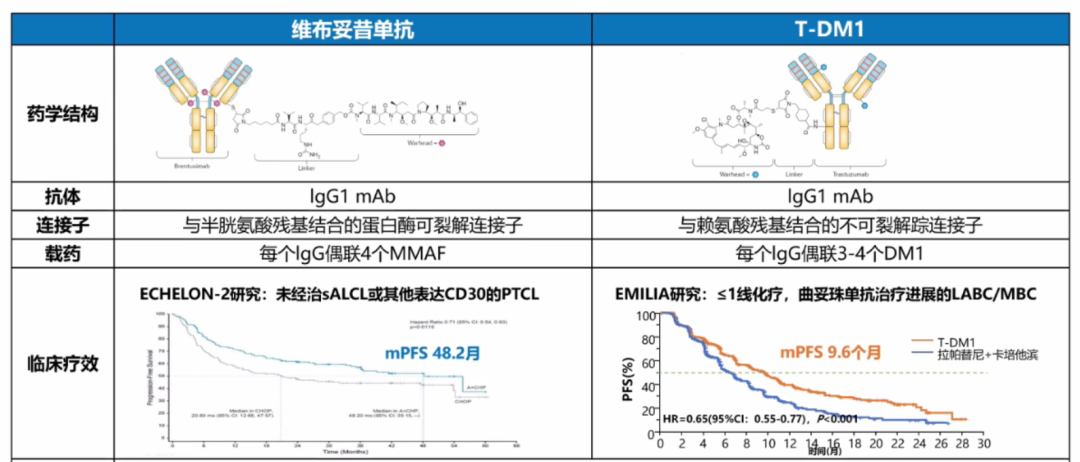
TDM1——EMILIA Study: T-DM1 Becomes Standard Second-Line Treatment for Advanced HER2 Cancer
The EMILIA study is an international multicenter, randomized, open-label phase III clinical trial comparing T-DM1 with lapatinib (anti-HER2 drug) + capecitabine (chemotherapy drug) for HER2-positive advanced breast cancer patients previously treated with trastuzumab in combination with paclitaxel, enrolling a total of 991 patients. The primary endpoints are PFS (assessed by independent review), OS, and safety. Secondary endpoints include PFS (investigator assessment), ORR, and symptom progression time. Results showed that compared to the lapatinib plus capecitabine group, the T-DM1 group significantly improved median PFS (9.6 months vs 6.4 months, HR=0.65, P<0.001) and median OS was also significantly extended (30.9 months vs 25.1 months, HR=0.68, P<0.001).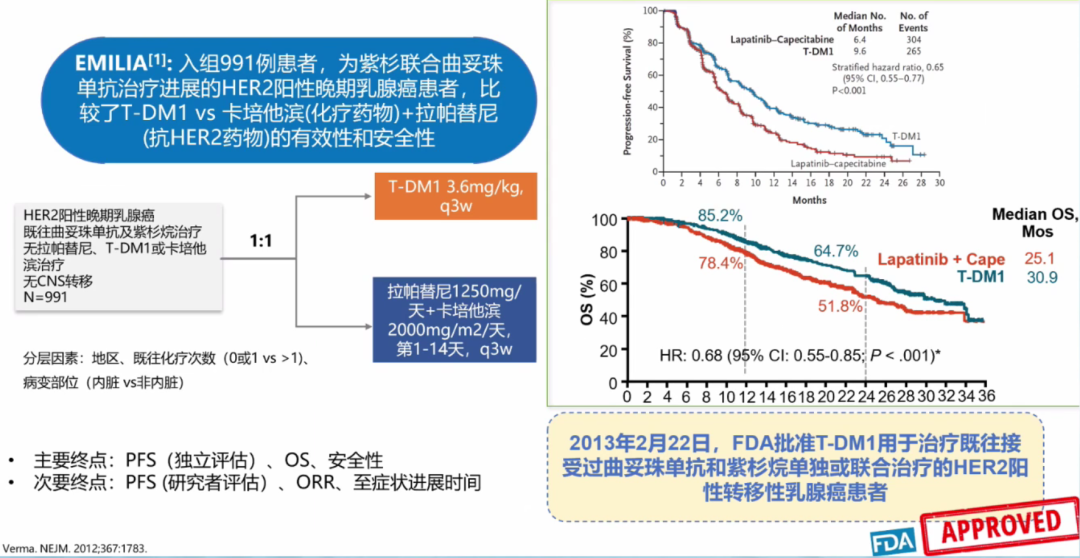 RC48——C008 Study: NMPA Approves Vedicimab for HER2-Positive Advanced Gastric Cancer TreatmentThe C008 study is a single-arm, open-label, multicenter phase II clinical trial of vedicimab in patients with gastric cancer/gastroesophageal junction adenocarcinoma, which included HER2-overexpressing (IHC 2+ or IHC 3+) patients who had previously received ≥2 lines of chemotherapy, achieving an ORR of 24.8%, disease control rate (DCR) of 42.4%, mPFS of 4.1 months, and mOS of 7.9 months.
RC48——C008 Study: NMPA Approves Vedicimab for HER2-Positive Advanced Gastric Cancer TreatmentThe C008 study is a single-arm, open-label, multicenter phase II clinical trial of vedicimab in patients with gastric cancer/gastroesophageal junction adenocarcinoma, which included HER2-overexpressing (IHC 2+ or IHC 3+) patients who had previously received ≥2 lines of chemotherapy, achieving an ORR of 24.8%, disease control rate (DCR) of 42.4%, mPFS of 4.1 months, and mOS of 7.9 months.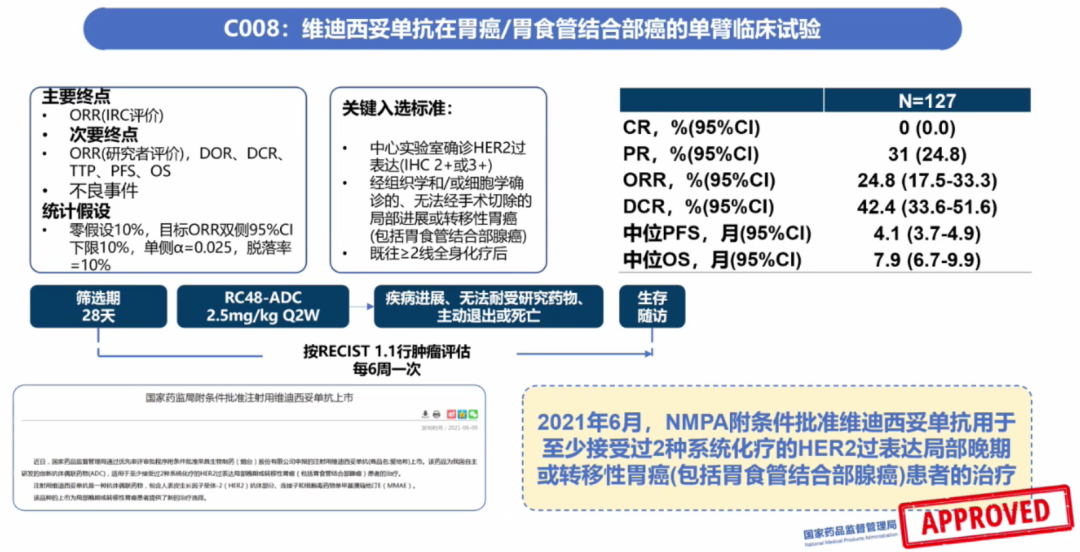 Based on the DESTINY-Lung01 Study, FDA Approves T-DXd for HER2-Positive Non-Small Cell Lung Cancer TreatmentThe DESTINY-Lung01 study is an open-label, multicenter, phase II clinical study aimed at evaluating the efficacy and safety of T-DXd in patients with HER2-overexpressing or HER2-mutated NSCLC who have failed standard treatments, with the primary endpoint being ORR confirmed by ICR. Results showed that T-DXd had an ORR as high as 54.9%, mPFS of 8.2 months (95% CI, 6.0-11.9), and mOS of 17.8 months (95% CI, 13.8-22.1).
Based on the DESTINY-Lung01 Study, FDA Approves T-DXd for HER2-Positive Non-Small Cell Lung Cancer TreatmentThe DESTINY-Lung01 study is an open-label, multicenter, phase II clinical study aimed at evaluating the efficacy and safety of T-DXd in patients with HER2-overexpressing or HER2-mutated NSCLC who have failed standard treatments, with the primary endpoint being ORR confirmed by ICR. Results showed that T-DXd had an ORR as high as 54.9%, mPFS of 8.2 months (95% CI, 6.0-11.9), and mOS of 17.8 months (95% CI, 13.8-22.1).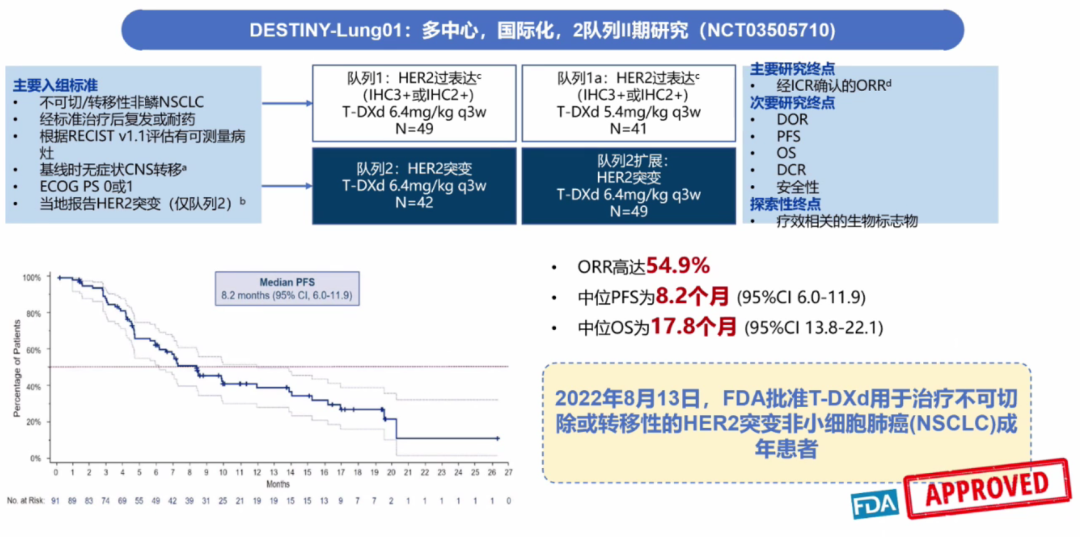
Current Issues with ADC
1. Potential Synergistic Effects of ADC with Immune Checkpoint Inhibitors.
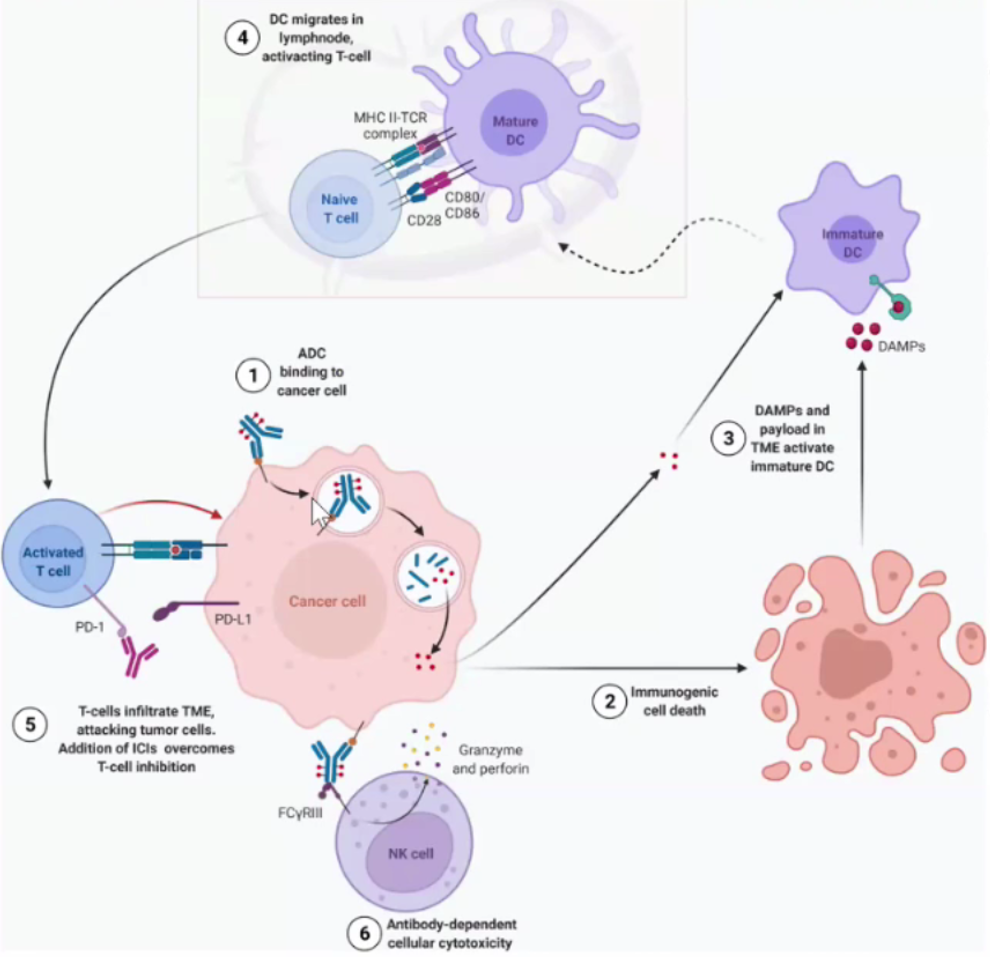
- ADC binds to tumor cell antigens and kills tumor cells
- During the process of ADC killing tumor cells, it promotes the maturation of dendritic cells (DCs), and cytotoxic drugs (DAMP) are released in the tumor microenvironment (TME), recognized by Toll-like receptors to stimulate DC maturation
- Mature dendritic cells activate immature T cells
- Activated T cells recognize and kill tumor cells
- PD-L1 antibody anti-tumor mechanism; in addition, ADC can exert antibody-dependent cellular cytotoxicity (ADCC)
- Antibody-dependent cellular phagocytosis and/or complement-dependent cytotoxicity
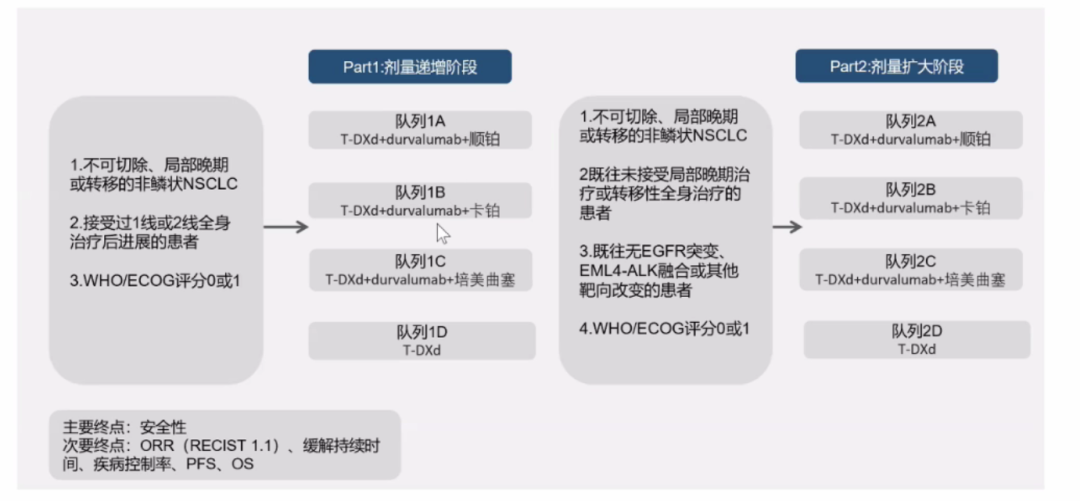
DESTINY-Lung03 Study: Evaluating the Safety and Tolerability of T-DXd Combined with Durvalumab and Chemotherapy in Advanced or Metastatic HER2-Positive Non-Squamous NSCLC Patients.
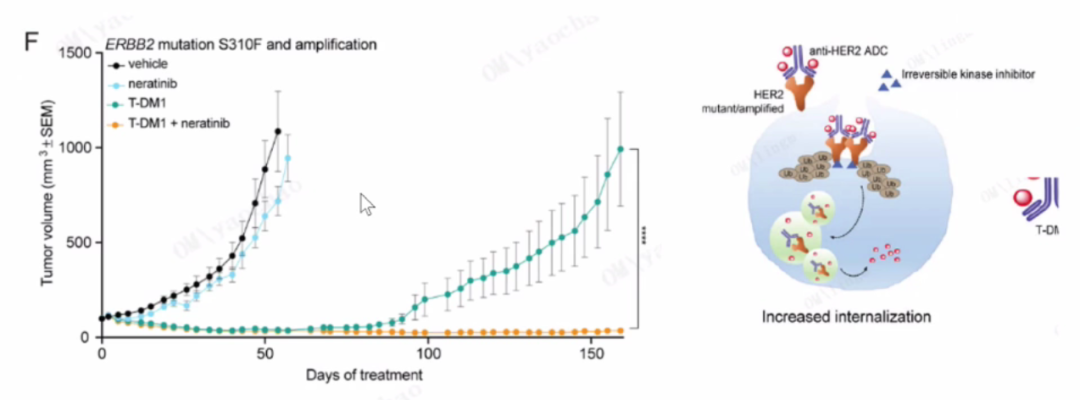
2. Optimizing ADC Efficacy: HER Irreversible Inhibitors Enhance Receptor Internalization
In PDX models, both T-DM1 and T-DM1 combined with lorlatinib can induce significant tumor regression, but the combined treatment has a more lasting effect; in HER2-mutated or amplified lung tumors, pan-HER irreversible inhibitors can enhance receptor ubiquitination and internalization, further improving efficacy.
3. Different ADCs Have Different Safety Event Profiles
Due to the differences in antibodies and cytotoxic drugs, the adverse reactions of different ADCs also vary. Adverse reactions that need special attention are categorized by the affected organ tissues, including hematological adverse reactions, infusion-related reactions, neurotoxicity, hepatotoxicity, gastrointestinal diseases, cardiac toxicity, infections, skin and subcutaneous tissue diseases, tumor lysis syndrome, metabolic toxicity, ocular diseases, and central toxicity. During treatment, relevant adverse reactions should be closely monitored, and serious adverse reactions should be actively prevented or treated supportively.

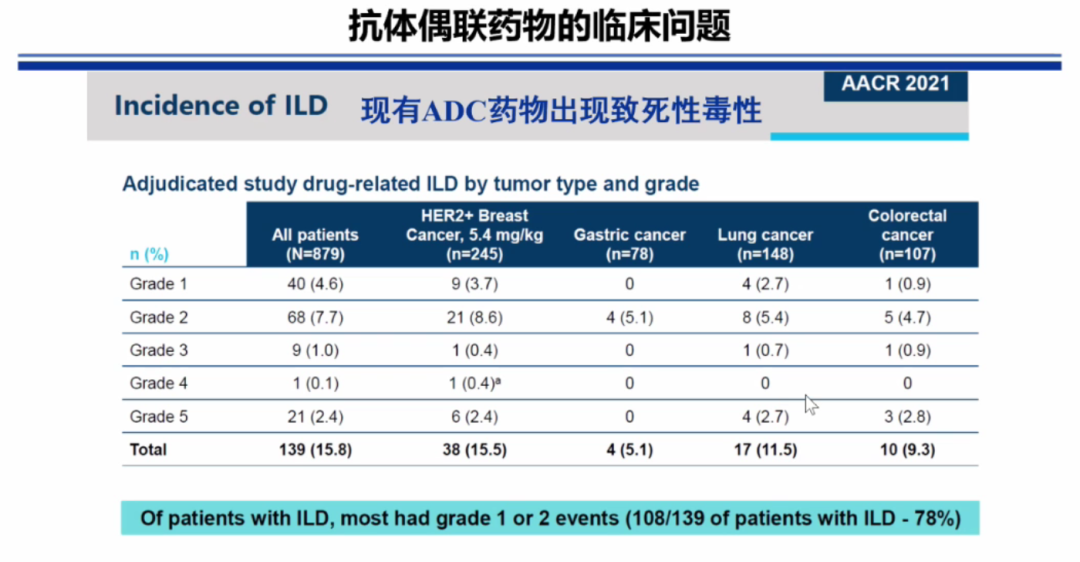
4. Clinical Issues of Antibody-Drug Conjugates
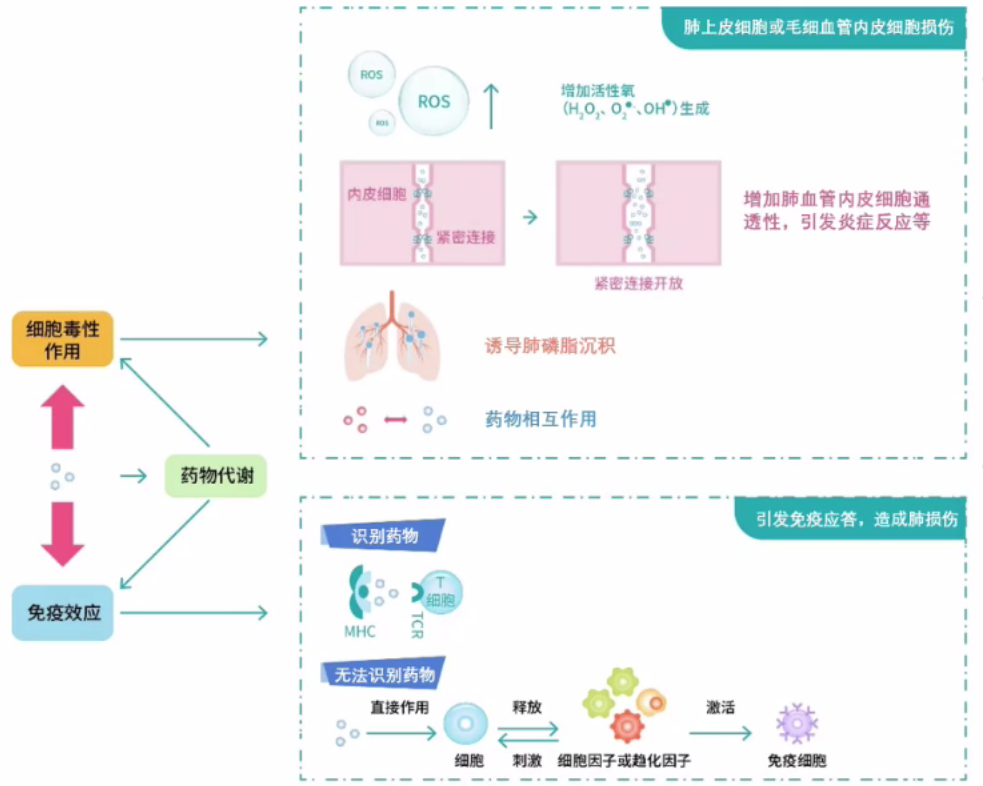
5. Direct Cytotoxic Effects and Immune-Mediated Effects May Contribute to the Pathogenesis of ILD
Cytotoxicity-mediated lung injury directly or indirectly damages alveolar epithelial cells, pulmonary vascular endothelial cells, and epithelial cells; reducing the repair capacity of alveolar epithelium.
Immune mechanism-mediated lung injury acts as a hapten or mimetic antigen component, inducing immune responses in the body.
Drug-related ILD caused by cytotoxicity occurs early, and its incidence is related to cumulative drug dosage, age, and whether other drugs are used. In contrast, the onset time of allergic mechanism-related diseases is unpredictable, and the incidence does not follow a linear relationship with the drug dose; upon re-exposure after a sensitization event, pneumonia can occur immediately.
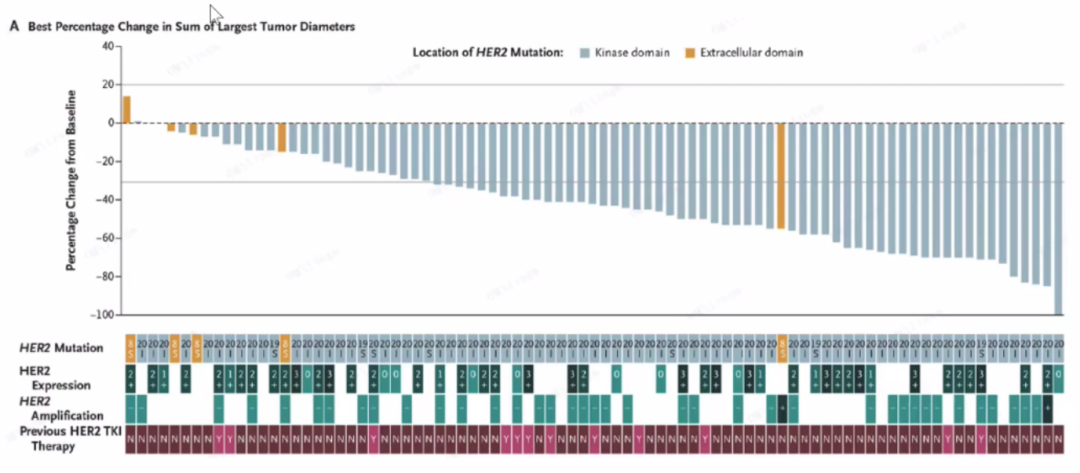
6. Correlation Between HER2 Mutations and T-DXd Efficacy
Three types of HER2 mutations have been found in NSCLC: HER2 mutations, HER2 amplifications, and HER2 overexpression.

HER2 expression/amplification is not related to T-DXd efficacy; different HER2 mutations are effective against T-DXd.
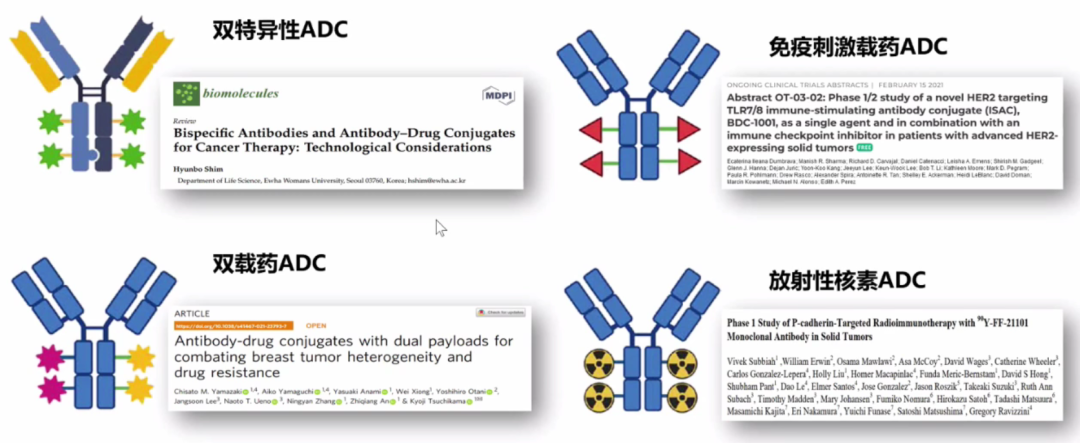
Future Development Trends of ADC Drugs
Actively expanding target selection and seeking differentiated development is a necessary path for ADC drug research and development.
In the future, leveraging the ADC concept, platform, and technology, there is hope to further precisely upgrade drug structure design.
Editor | Chen Sushu

 Forward, Like, Watch, Arrange
Forward, Like, Watch, Arrange