* For reference by medical professionals only

What Issues Should Be Addressed During the Infusion of ADC Drugs for Breast Cancer?
ADC drugs combine the precise targeting of antibody drugs with the efficient killing advantage of cytotoxic drugs, gradually changing the treatment landscape for breast cancer. Currently, ADC drugs that have entered clinical practice in China include trastuzumab emtansine (T-DM1), trastuzumab deruxtecan (T-DXd), and sacituzumab govitecan (SG), among others. T-DM1 is the first HER2-targeted ADC approved for solid tumors, approved for second-line treatment of HER2-positive advanced breast cancer based on the Phase III EMILIA study, and later approved for adjuvant treatment of HER2-positive early breast cancer after neoadjuvant therapy for non-pCR based on the KATHERINE study[1,2]. T-DXd achieved breakthrough results in the DESTINY-Breast03 study, supporting T-DXd as a new standard regimen for second-line treatment of HER2-positive advanced breast cancer[3]. Additionally, in the DESTINY-Breast04 study, T-DXd significantly prolonged PFS and OS in HER2-low expressing breast cancer compared to chemotherapy, marking a departure from the binary classification of HER2-positive and negative breast cancer, and expanding the beneficiary population of anti-HER2 treatment[4]. SG is the first TROP2-targeted ADC drug on the market, providing an important treatment option for patients with triple-negative breast cancer[5].With the continuous launch of new drugs, there are also new requirements for healthcare personnel regarding the infusion operation specifications for ADC drugs. The Expert Group of the Breast Cancer Case Managers Branch of the Chinese Pharmaceutical Education Association has formulated the “Expert Consensus on the Management of Infusion of Antibody-Drug Conjugates for Breast Cancer” (hereinafter referred to as the “Consensus”)[6], which comprehensively elaborates on the infusion standards for breast cancer ADC drugs, early prevention of related adverse reactions, and practical guidance for timely management, using T-DM1, SG, and T-DXd as examples, for healthcare personnel to reference in intravenous infusion operations of breast cancer ADC drugs.
Standard Operating Procedures (SOP) for the Preparation and Infusion of Breast Cancer ADC Drugs
The “Consensus” emphasizes that intravenous infusion of breast cancer ADC drugs should adhere to the principles of preparation as needed and sterile preparation, with the preparation process shown in Figure 1; during the preparation process, strict adherence to verification systems is required, with double verification and confirmation followed by single and double signatures; it is recommended to implement centralized preparation and supply in the Pharmacy Intravenous Admixture Service (PIVAS), or to prepare in the ward under conditions with a biological safety cabinet or ultra-clean workbench to reduce the occupational hazards of toxic drugs to healthcare personnel. The infusion process follows the intravenous infusion flow, as shown in Figure 2.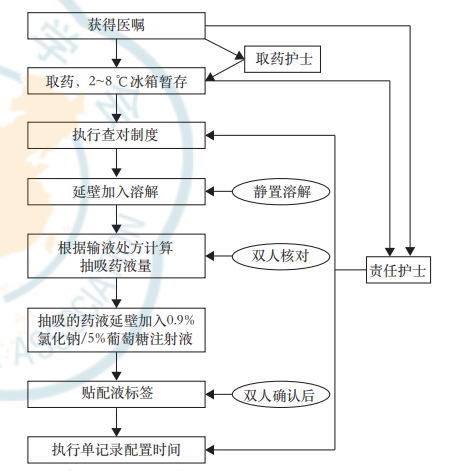 Figure 1. ADC Drug Preparation Workflow
Figure 1. ADC Drug Preparation Workflow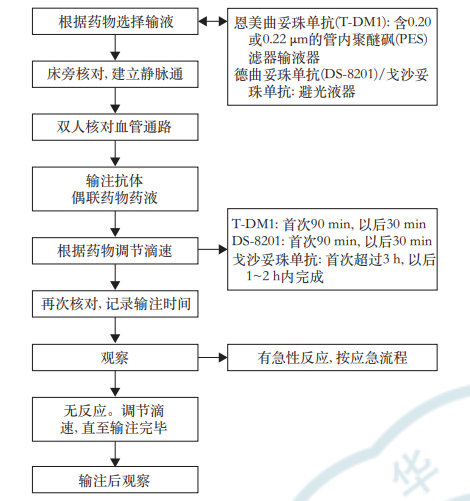 Figure 2. ADC Drug Infusion WorkflowIf infusion reactions occur during the infusion of ADC drugs, the following emergency plans should be implemented: (1) The patient should inform the nurse if they perceive any reactions, or the nurse should inquire/observe during rounds; (2) Immediately close the infusion device and call for assistance from other medical personnel; (3) Change the infusion device, withdraw the remaining drug from the indwelling needle, and the office nurse should assist in preserving the leftover drug, confirming that the physician is informed, and bringing emergency supplies to the bedside; (4) Prepare for rescue, administer medication according to physician’s orders, observe the patient, keep the patient warm if they experience chills, and monitor temperature; (5) Keep detailed records: rescue process, vital signs, start and end times, etc.; (6) Prepare for re-infusion, prohibiting re-infusion if the reaction is severe; (7) Dispose of discarded drugs according to leftover drug processing procedures (Figure 3).
Figure 2. ADC Drug Infusion WorkflowIf infusion reactions occur during the infusion of ADC drugs, the following emergency plans should be implemented: (1) The patient should inform the nurse if they perceive any reactions, or the nurse should inquire/observe during rounds; (2) Immediately close the infusion device and call for assistance from other medical personnel; (3) Change the infusion device, withdraw the remaining drug from the indwelling needle, and the office nurse should assist in preserving the leftover drug, confirming that the physician is informed, and bringing emergency supplies to the bedside; (4) Prepare for rescue, administer medication according to physician’s orders, observe the patient, keep the patient warm if they experience chills, and monitor temperature; (5) Keep detailed records: rescue process, vital signs, start and end times, etc.; (6) Prepare for re-infusion, prohibiting re-infusion if the reaction is severe; (7) Dispose of discarded drugs according to leftover drug processing procedures (Figure 3).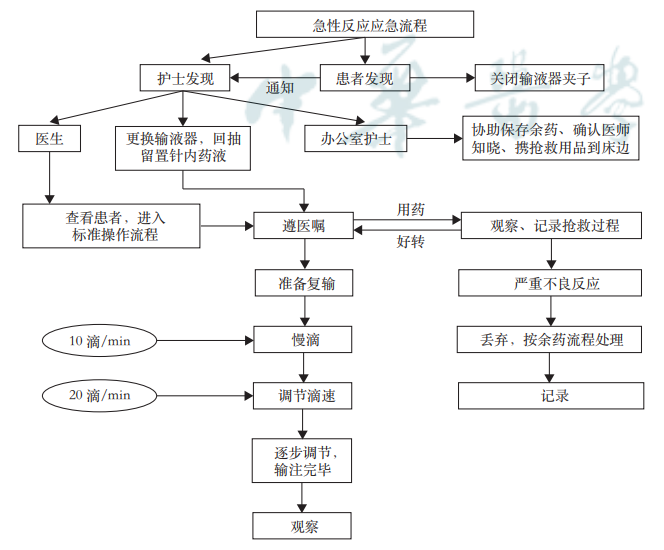 Figure 3. Emergency Procedures for Acute Reactions During ADC Drug Infusion
Figure 3. Emergency Procedures for Acute Reactions During ADC Drug Infusion
Management of Breast Cancer ADC Drug Infusion
1. Specifications and Preparation Principles of ADC Drugs
The “Consensus” points out that while T-DM1 (100 mg/vial and 160 mg/vial), T-DXd (100 mg/vial), and SG (180 mg/vial) are all ADC drugs, the molecular structural characteristics of the three drugs are different and cannot be interchanged or used together. To prevent medication errors, the vial labels should be carefully checked and verified before infusion to ensure that the drug being prepared and used is correct. The preparation and dosage of the drugs should strictly follow the physician’s orders and the instructions for use.
2. ADC Drug Injection Solution Preparation and Administration Protocol
The “Consensus” elaborates on the injection solution preparation process and administration protocol for T-DM1, T-DXd, and SG. It is important to emphasize that T-DM1 should not be diluted with glucose (5%) solution, as it can cause protein aggregation; it should not be mixed or diluted with other drugs. T-DXd should not be diluted with 0.9% sodium chloride solution, as it may lead to particle formation. SG can only be prepared using 0.9% sodium chloride solution, and SG should not be replaced with other drugs containing irinotecan or its active metabolite SN-38, or used in combination with such drugs. Additionally, blood routine, blood biochemistry, and other indicators should be monitored before the infusion of ADC drugs, and close observation should be made during the infusion for any infusion reactions such as fever or chills, and adverse reactions should be monitored based on observation time after the infusion.
▌Injection Solution Preparation and Administration Protocol for T-DM1
(1) Preparation of Reconstitution Solution: ① Using a sterile syringe, slowly inject 5 ml of sterile water for injection into the 100 mg T-DM1 vial, or inject 8 ml of sterile water for injection into the 160 mg T-DM1 vial. ② Gently rotate the vial until fully dissolved, do not shake vigorously. ③ Store the reconstituted T-DM1 solution at 2~8 °C; discard any unused T-DM1 solution after 24 hours (the reconstituted preparation is for single use only, and any unused portion should be discarded promptly). ④ Before using the reconstituted solution, perform a visual inspection to ensure there are no particulate matter or discoloration. Typically, the reconstituted solution should be clear to slightly milky. The color of the reconstituted solution should be colorless to light brown. If the reconstituted solution contains visible particles, is cloudy, or discolored, do not use.(2) Dilution Instructions for Reconstituted Solution: ① Take an appropriate amount of solution from the vial, then add it to an infusion bag containing 250 ml of 0.45% sodium chloride or 0.9% sodium chloride. ② Once ready for infusion, the drug should be administered immediately. ③ If not used immediately, the infusion solution can be stored in the refrigerator at 2~8 °C for up to 24 hours. ④ During storage, do not freeze or shake the infusion bag.(3) Administration Protocol: ① The recommended dose of T-DM1 is 3.6 mg/kg, once every 3 weeks (21 days is one cycle). The initial dose should be administered as an intravenous infusion over 90 minutes, and the patient should be observed during the infusion and for at least 90 minutes after the initial dose for fever, chills, or other infusion-related reactions. During administration, closely monitor the infusion site to prevent potential subcutaneous extravasation. If the patient has tolerated previous infusions well, subsequent doses of T-DM1 can be infused over 30 minutes. If the patient experiences infusion-related symptoms, the infusion rate of this product should be slowed or the administration should be interrupted. In the case of life-threatening infusion reactions, treatment should be terminated. ② Typical adverse reaction dose adjustments for T-DM1: dose adjustments for thrombocytopenia adverse events caused by T-DM1 are shown in Table 1.Table 1. Dose Adjustments for Thrombocytopenia Adverse Events Caused by T-DM1
▌Injection Solution Preparation and Administration Protocol for T-DXd
(1) Preparation of Reconstitution Solution for T-DXd: ① Retrieve the required number of T-DXd vials needed for the planned dosage from storage, and keep the outer packaging until T-DXd solution preparation is completed. ② Remove the cap of the sterile water for injection and wipe the top with alcohol. ③ Using a sterile syringe, slowly inject 5 ml of sterile water for injection into each T-DXd vial. ④ Rotate and invert the vial to fully dissolve the powder, do not shake. ⑤ The prepared solution should be a clear liquid that is colorless to pale yellow, with a final concentration of 20 mg/ml. ⑥ If the reconstituted solution is not used immediately, it can be stored in the refrigerator at 2~8 °C for up to 24 hours, do not freeze. ⑦ The reconstituted preparation does not contain preservatives and is for single use only.(2) Dilution of Reconstituted Solution for T-DXd: ① Using a sterile syringe, take the calculated volume of the reconstituted solution. Check the reconstituted solution for particles and discoloration. The solution should be clear and colorless to pale yellow. If visible particles or cloudiness or discoloration are observed, do not use. ② Add the calculated volume of the reconstituted product to an infusion bag containing 100 ml of 5% glucose solution for dilution, do not use sodium chloride solution. It is recommended to use infusion bags made of polyvinyl chloride or polyolefin (copolymer of ethylene and polypropylene). ③ Gently invert the infusion bag to thoroughly mix the solution, do not shake. During the preparation and administration of T-DXd, the prepared infusion bag must be protected from light. ④ Discard all unused portions in the vial.(3) Administration Protocol for T-DXd: ① The recommended dose of T-DXd is 5.4 mg/kg, administered via intravenous infusion (do not push or inject rapidly intravenously under light protection). Once every 3 weeks (each cycle is 21 days) intravenous infusion, until disease progression or intolerable toxicity. For the first infusion: the first infusion should last no less than 90 minutes; for subsequent infusions: if tolerance is good, the second infusion should last no less than 30 minutes. If the patient experiences infusion-related symptoms, the infusion rate of this product should be slowed or the administration should be interrupted. In the case of severe infusion reactions, this product should be permanently discontinued. ② Typical adverse reaction dose adjustments for T-DXd: if infusion-related adverse reactions occur, it may be necessary to temporarily discontinue, reduce the dose, or permanently discontinue the drug. The recommended dose reduction for T-DXd is the starting dose of 5.4 mg/kg, the first dose reduction adjustment to 4.4 mg/kg, the second dose reduction adjustment to 3.2 mg/kg, and if further dose reduction is needed, treatment should be terminated. T-DXd dose and adverse reactions are shown in Table 2.Table 2. Dose Adjustments for Adverse Reactions of T-DXd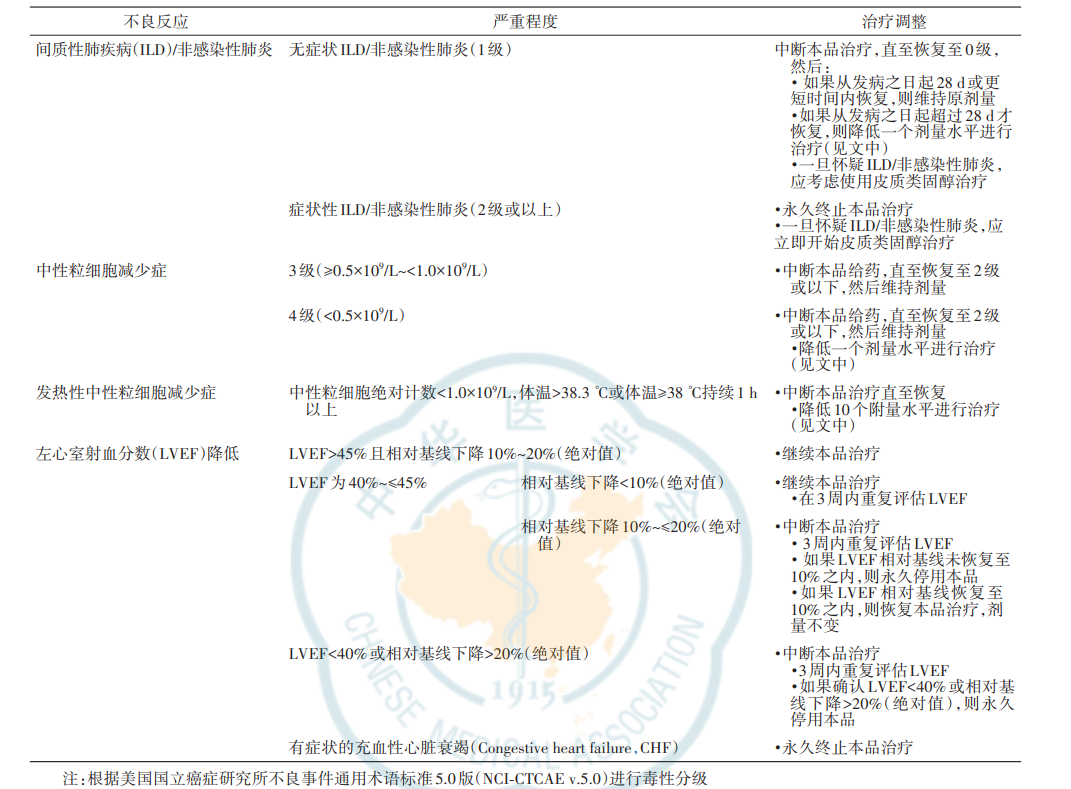
▌Injection Solution Preparation and Administration Protocol for SG
(1) Preparation of Reconstitution Solution for SG: ① Using a sterile syringe, slowly inject 20 ml of 0.9% sodium chloride injection into the 180 mg SG vial to obtain a solution with a concentration of 10 mg/ml. ② Gently rotate the vial to dissolve for 15 minutes, do not shake vigorously. ③ The prepared reconstitution solution should be diluted immediately. ④ Before administering the reconstitution solution, visually inspect the injection drug for particulate matter and discoloration. The solution should be clear yellow. If the reconstitution solution is cloudy or discolored, do not use. ⑤ After reconstitution, prepare the dilution solution for infusion immediately.(2) Dilution Instructions for SG Reconstitution Solution: ① Using a syringe, take an appropriate amount of the solution from the vial, and adjust the volume in the infusion bag with 0.9% sodium chloride infusion to achieve a concentration of 1.1~3.4 mg/ml (the total volume should not exceed 500 ml), only 0.9% sodium chloride may be used for dilution for infusion. ② If the patient weighs over 170 kg, the total dose of SG should be divided into two 500 ml infusion bags and infused sequentially. The reconstituted preparation is for single use only, and any unused portion should be discarded promptly. ③ Once ready for infusion, the diluted solution in the infusion bag should be used immediately, the infusion bag should be protected from light. ④ If not used immediately, the diluted solution can be stored in the refrigerator at 2~8 °C for 4 hours. After refrigeration, the diluted solution should be used within 6 hours (including infusion time). ⑤ During storage, do not freeze or shake the infusion bag, and it must be protected from light.(3) Administration Protocol for SG: The recommended dose for SG is 10 mg/kg, and the administration dose should not exceed 10 mg/kg. Every 21 days is one treatment cycle, with intravenous infusion on days 1 and 8. Treatment should continue until disease progression or unacceptable toxicity. For the first infusion: the infusion time should last more than 3 hours, and during and after the infusion, the patient should be observed for at least 30 minutes for any infusion reactions. For subsequent infusions: if the previous infusion was tolerated, the infusion time can be 1-2 hours or longer. During the infusion, observe the patient for any infusion reactions, and after the infusion, observe for at least 30 minutes. If the patient experiences infusion reactions, the infusion rate of this product should be slowed or the infusion should be interrupted. In the case of life-threatening infusion reactions, the product should be permanently discontinued. After dose reduction due to adverse reactions, do not increase the dose again. Dose adjustments for pausing or permanently discontinuing SG are shown in Table 3.Table 3. Dose Adjustments for Adverse Reactions of SG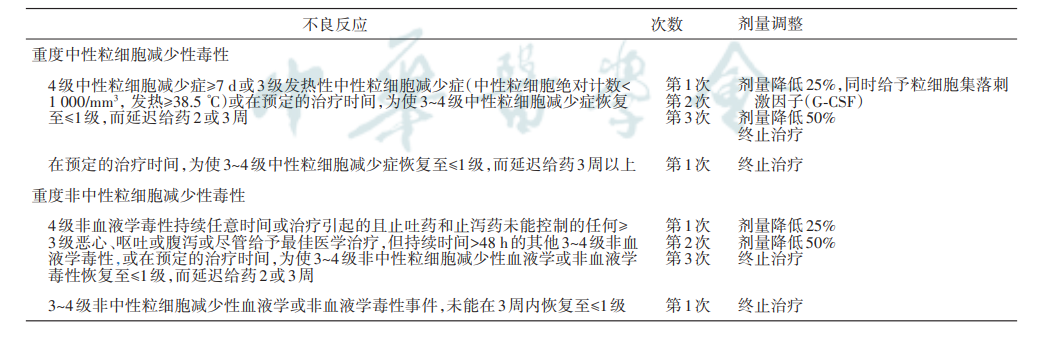
3. Selection of Infusion Devices and Infusion Pathways, and Storage of ADC Drugs
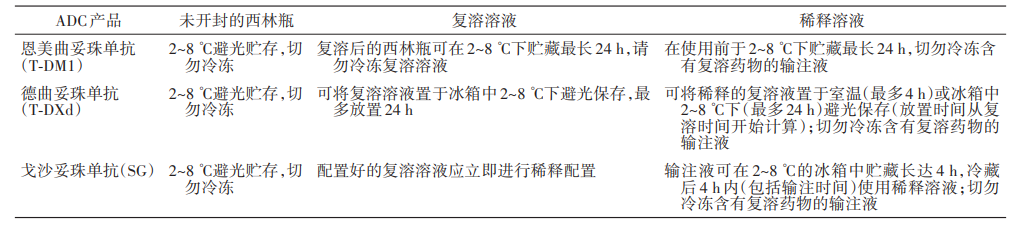
The “Consensus” recommends that ADC drugs should preferably be infused using a centrally inserted peripheral catheter (PICC) or infusion port. Different ADC drugs require different infusion devices: T-DM1 requires a 0.20 or 0.22 μm in-line polyethersulfone (PES) filter if infused with 0.9% sodium chloride; T-DXd infusion bags can use materials such as polyvinyl chloride, polyethylene, or polypropylene, with filters only being 0.20 or 0.22 μm PES or polysulfone (PS) filters; SG can use standard infusion devices.During preparation and infusion, the infusion bags and devices for T-DXd and SG must be protected from light. If the prepared T-DXd infusion is stored in the refrigerator (2~8 °C), it should be warmed to room temperature under light protection before administration. The “Consensus” details the storage conditions for the three ADC drugs under different states, as shown in Table 4.
Table 4. Storage Conditions for Unopened, Reconstituted, and Diluted Solutions of Breast Cancer ADC Drugs
4. Preventive Medications Before ADC Drug Infusion
The “Consensus” recommends the following measures to prevent the occurrence of adverse reactions related to ADC drugs:
- T-DXd:has emetogenic potential [including delayed nausea and/or vomiting], and a combination of two or three drugs [for example, dexamethasone with 5-HT3 receptor antagonists and/or NK1 receptor antagonists, along with other applicable medications] should be pre-administered before each use to prevent chemotherapy-induced nausea and vomiting.
- SG:Before each SG infusion, it is recommended to pre-administer antipyretics, H1 and H2 blockers, and patients with a history of infusion reactions may use corticosteroids to prevent “infusion reactions”;pre-administer a combination treatment regimen of two or three drugs (for example: dexamethasone with 5-HT3) to prevent nausea and vomiting.
- T-DM1:No preventive medication is required before infusion.
In terms of disposal of unused/expired drugs, handling of delayed or missed doses, the “Consensus” also provides detailed recommendations. Additionally, to ensure patient safety, patients should be educated on their condition assessment, adherence to physician’s orders for regular check-ups, and awareness and observation of common adverse reactions, advising patients to report any discomfort promptly. Patient health education on common adverse reactions during breast cancer ADC drug infusion, including hematologic adverse reactions, infusion reactions, peripheral neuropathy, pulmonary toxicity, gastrointestinal adverse reactions, and cardiac toxicity, is also part of the nursing responsibilities.
Conclusion
The “Expert Consensus on the Management of Infusion of Antibody-Drug Conjugates for Breast Cancer” effectively addresses the main issues faced by healthcare personnel during the infusion process of breast cancer ADC drugs, providing comprehensive and detailed guidance through 16 recommendations, which contributes to improving the safety and therapeutic efficacy of breast cancer patients during ADC drug infusion.Appendix: 16 Recommendations from the “Expert Consensus on the Management of Infusion of Antibody-Drug Conjugates for Breast Cancer”:
Recommendation 1: Infusion of breast cancer ADC drugs should adhere to the principles of preparation as needed and sterile preparation, with strict adherence to verification systems during the preparation process, including double verification, confirmation, and signatures (Consensus degree: 100%).
Recommendation 2: According to clinical needs, it is recommended to implement centralized preparation and supply of breast cancer ADC drugs in the Pharmacy Intravenous Admixture Service (PIVAS), or to prepare in the ward under conditions with a biological safety cabinet or ultra-clean workbench to reduce the occupational hazards of toxic drugs to healthcare personnel (Consensus degree: 98%).
Recommendation 3: The ADC drug infusion SOP should follow the intravenous infusion process (Consensus degree: 100%).
Recommendation 4: If a patient experiences an infusion reaction during the drug infusion process, immediate implementation of the acute reaction emergency procedures should be taken (Consensus degree: 99%).
Recommendation 5: It is recommended that T-DXd and SG be prepared protected from light (Consensus degree: 97%).
Recommendation 6: The three ADC drugs, T-DM1, T-DXd, and SG, must be strictly prepared and diluted according to sterile techniques, and cannot be interchanged or used together. To prevent medication errors, the vial labels should be carefully checked and verified before infusion to ensure that the drug being prepared and used is correct; the preparation and dosage of the drugs should strictly follow the physician’s orders and instructions for use (Consensus degree: 100%).
Recommendation 7: It is recommended to prioritize the use of PICC/infusion ports for ADC drug infusion (Consensus degree 98%).
Recommendation 8: If using 0.9% sodium chloride for T-DM1 infusion, a 0.20 or 0.22 μm in-line PES filter is required; T-DXd filters may only use 0.20 or 0.22 μm PES or PS filters; SG infusion can use standard infusion devices (Consensus degree: 99%).
Recommendation 9: The infusion bags for T-DXd and SG must be protected from light; it is recommended that infusion devices also be light-protected, and curtains and lights should be closed during infusion (Consensus degree: 98%).
Recommendation 10: T-DM1 and T-DXd infusion solutions can be stored in the refrigerator at 2~8 °C for up to 24 hours; SG infusion solutions can be stored in the refrigerator at 2~8 °C for a maximum of 4 hours, and after refrigeration, should be used within 6 hours (including infusion time) (Consensus degree: 98%).
Recommendation 11: T-DXd and SG have emetogenic potential [including delayed nausea and/or vomiting], and pre-medication should be administered before each use (Consensus degree: 100%).
Recommendation 12: T-DM1 should not be diluted with glucose (5%) solution, as it can cause protein aggregation; it should not be mixed or diluted with other drugs. T-DXd should not be diluted with 0.9% sodium chloride solution, as it may lead to particle formation; SG can only be prepared using 0.9% sodium chloride solution, and SG should not be replaced with other drugs containing irinotecan or its active metabolite SN-38, or used in combination with such drugs (Consensus degree: 100%).
Recommendation 13: If there is a plan to delay or miss a dose, the drug should be administered as soon as possible without waiting for the next scheduled cycle; adjust the administration schedule for the next dose to maintain a 3-week interval between doses, using the dose and rate tolerated by the patient in the most recent infusion (Consensus degree: 97%).
Recommendation 14: Before ADC drug infusion, blood routine, blood biochemistry, and other indicators should be monitored, and close observation should be made during the infusion for any infusion reactions such as fever or chills, and adverse reactions should be monitored based on observation time after the infusion (Consensus degree: 98%).
Recommendation 15: To ensure patient safety, patients should be educated on their condition assessment, adherence to physician’s orders for regular check-ups, and awareness and observation of common adverse reactions, advising patients to report any discomfort promptly (Consensus degree: 100%).
Recommendation 16: Patients should be educated on common adverse reactions during infusion, including hematologic adverse reactions, infusion reactions, peripheral neuropathy, pulmonary toxicity, gastrointestinal adverse reactions, cardiac toxicity, etc. (Consensus degree: 97%).
References:
[1] Sunil Verma et al. N Engl J Med 2012;367:1783-91.
[2] G. von Minckwitz et al. N Engl J Med 2019;380:617-28.
[3] Sara A Hurvitz et al. Lancet 2023; 401: 105–17
[4] S. Modi et al. N Engl J Med 2022;387:9-20.
[5] A. Bardia et al. N Engl J Med 2021;384:1529-41.
[6] Chinese Pharmaceutical Education Association Breast Cancer Case Managers Branch. Expert Consensus on the Management of Infusion of Antibody-Drug Conjugates for Breast Cancer [J]. Chinese Medical Journal, 2023, 103(34): 2704-2712.
This material is supported by AstraZeneca and is for reference by healthcare professionals only.Approval Number: CN-124518 Valid until: 2024-11-21* This article is intended to provide scientific information to medical professionals and does not represent the views of this platform.
 For more medical information, click “Read Original” to view
For more medical information, click “Read Original” to view