
△ A grand contribution, 1 main forum, 5 sub-forums, 9 thematic forums, hundreds of industry leaders, many renowned clinical PIs and dozens of CMOs gathered, a thousand-person conference awaits you!
▼
Antibody-drug conjugates (ADCs) are currently developing rapidly, utilizing antibodies to selectively deliver cytotoxic drugs to tumor sites. As of May 2021, the U.S. Food and Drug Administration (FDA) has approved 10 types of ADCs: Adcetris®, Kadcyla®, Besponsa®, Mylotarg®, Polivy®, Padcev®, Enhertu®, Trodvy®, Blenrep®, and Zynlonta™, used alone or in combination for the treatment of breast cancer, urethral cancer, multiple myeloma, acute leukemia, and lymphoma.
In addition, there are currently over 80 ADCs under investigation in approximately 150 active clinical trials. Despite the increasing popularity of ADCs, expanding their therapeutic index (better efficacy with less toxicity) remains a challenge. However, the development of new technologies, such as site-specific conjugation, linkers, payloads, new biological platforms, and advanced analytical techniques, is helping to shape the future development of ADCs.
01
Mechanism of Action and Key Elements of ADCs
Most ADCs follow a similar mode of action, including antibody-mediated receptor binding, ADC internalization, and subsequent payload release and cytotoxicity (see the figure below), along with the bystander effect. The success of ADCs relies on several key factors.
1) Target antigens (e.g., CD30, HER2, CD22, CD33, CD79b, Nectin 4, Trop2, BCMA, CD19)
2) Types of antibodies (e.g., IgG1, IgG2, IgG4, nanobodies, bispecific antibodies).
3) Types of payloads (e.g., MMAE, DM4, calicheamicin, DM1, MMAF)
4) Types of linkers (e.g., valine-citrulline, Sulfo-SPDB, hydrazone linkers),
5) Linker platforms (e.g., lysine, cysteine, and site-specific conjugation)
6) Target indications (e.g., breast cancer, lymphoma, leukemia, uremia, lung cancer, ovarian cancer, etc).
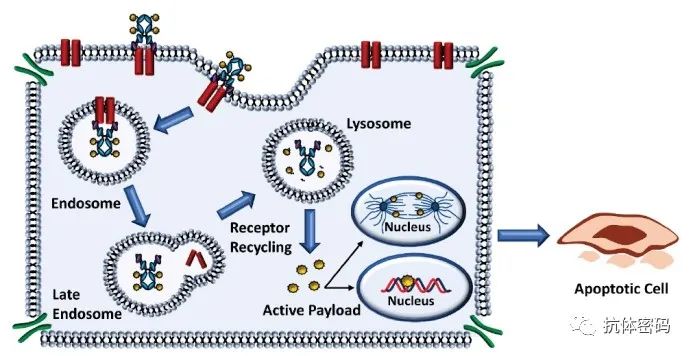
Mechanism of action of ADCs
02
Marketed ADC Drugs
Among the 10 approved ADC drugs, 6 are for the treatment of hematological malignancies (Table 1 and Figure A), which are Adcetris (Brentuximab vedotin), Besponsa (inotuzumab ozogamicin), Mylotarg (gemtuzumab ozogamicin), Polivy (polatuzumab vedotin), Blenrep (belantamab mafodotin), and Zynlonta (loncastuximab tesirine). The other 4 are used for the treatment of solid tumors (Table 1 and Figure B), which are Kadcyla (Ado-trastuzumab emtansine), Enhertu (trastuzumab deruxtecan), Trodelvy (sacituzumab govitecan), and Padcev (enfortumab vedotin)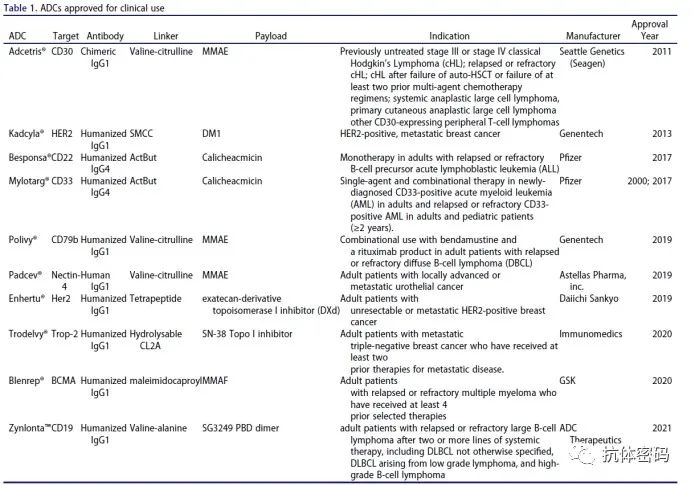
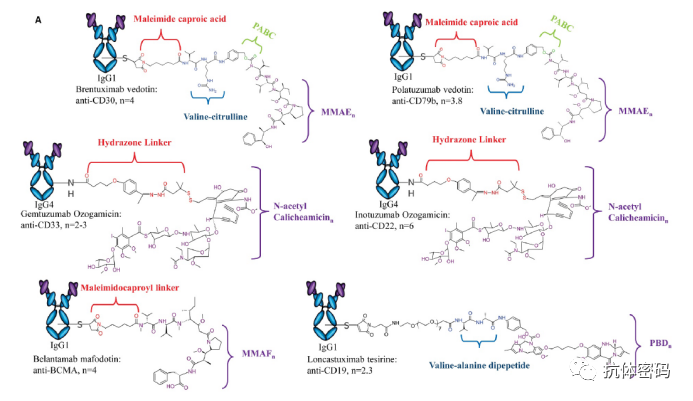 Structures and antibody subtypes of 6 ADC drugs for hematological malignancies
Structures and antibody subtypes of 6 ADC drugs for hematological malignancies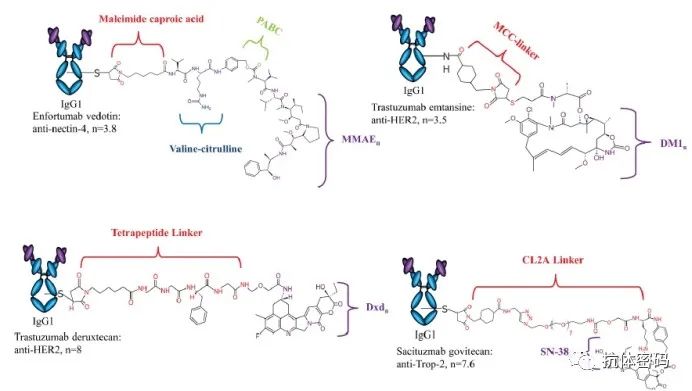 Subtypes and structures of 4 ADC drugs for solid tumors03
Subtypes and structures of 4 ADC drugs for solid tumors03
ADC Drugs in Clinical Trials
Currently, there are over 80 ADCs undergoing active clinical trials, most of which are in Phase I and I/II (Figure a and the table at the end). Over 80% of clinical trials are investigating the safety and efficacy of ADCs in various solid tumors, while the remaining trials involve hematological malignancies (Figure b). This indicates that following the success of early T-DM1 and the recent approvals of T-Dxd, sacituzumab govitecan, and enfortumab vedotin, there has been an increasing shift towards studying ADCs for solid tumors in recent years. The ADCs in these 80+ clinical trials target approximately 40 different targets (Figure c). Currently, HER2 is one of the most attractive targets in ADC drug development, with three anti-HER2 ADCs currently in Phase III trials. One of them, RC48, produced by RemeGen, conjugates the anti-HER2 IgG1 antibody hertuzumab with approximately four MMAE molecules through a valine-citrulline linker that can be cleaved by proteases. In preclinical studies, lower doses of RC48 demonstrated antitumor activity in xenograft models sensitive and resistant to trastuzumab and lapatinib. Compared to T-DM1, it exhibits better antitumor efficacy. Studies have shown that in multiple Phase I trials targeting HER2-positive malignancies, its safety can be effectively controlled, and in a Phase II pivotal trial (NCT03507166), it achieved encouraging results: including a total response rate (ORR) of 51.2% in pre-treated HER-2-positive locally advanced or metastatic urothelial carcinoma. In terms of small molecule drugs, most induce disruption of microtubules and arrest mitosis, while a few cause DNA damage (Figure 3d). Of course, some novel small molecule drugs are gradually being used for ADCs, such as TRL7/8 (Toll-like receptor agonists), RNA polymerase II inhibitors, and BCL-xL anti-apoptotic protein targeting, etc. Regarding conjugation methods: the method of conjugation can directly affect the quality of ADCs. The quality of ADCs, in turn, affects product safety and efficacy. Currently, there are three main conjugation methods: through the reduction of interchain disulfide bonds in cysteine, exposing lysines on the antibody surface, and site-specific conjugation techniques. Currently, most ADC drugs in clinical trials are either through traditional cysteine conjugation or site-specific conjugation techniques licensed by manufacturers. Only a small portion use traditional lysine conjugation methods, which may be due to the potential for significant heterogeneity in ADC drugs. (Figure e).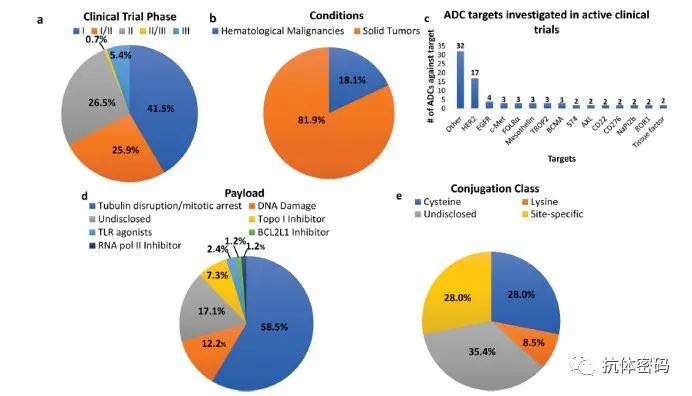 ADC drugs for tumor treatment in clinical practice04
ADC drugs for tumor treatment in clinical practice04
Challenges in ADC Development
There are many challenges to face in the development of ADC drugs, the first being to demonstrate the efficacy of the drug. Many drugs have been forced to terminate due to their inability to prove efficacy in clinical settings, such as MM-302 and Rova-T. Additionally, the toxicity associated with ADC drugs is also a challenge that must be faced. For example, using calicheamicin as a payload is associated with increased incidence of liver damage and hepatotoxicity. Issues such as increased incidence of venous occlusive disease (also known as sinusoidal obstruction syndrome) and the occurrence of drug-induced liver injury have been observed. During the clinical trial and post-approval use of gemtuzumab ozogamicin, increases in venous occlusive disease (also known as sinusoidal obstruction syndrome) and drug-induced liver injury were noted. At the same time, there have also been reports of peripheral neuropathy and neutropenia caused by MMAE, ocular side effects caused by MMAF, and neutropenia caused by topoisomerase I inhibitors.Development of Resistance: Over time, tumors can develop mechanisms to overcome drug efficacy, leading to reduced or lost effectiveness. Since ADCs exert their effects through multiple pathways, resistance can occur at any stage of drug action (see the figure). A potential mechanism of resistance may arise from the modulation of antibody recognition of the antigen. This may be due to downregulation of the target’s expression on the cell surface. Some preclinical studies have shown that cells treated continuously with ADCs eventually develop acquired resistance models over time, resulting in reduced expression of target antigen proteins. To combat such resistance mechanisms, some bispecific antibody ADCs targeting dual epitopes are already in clinical development, such as ZW49 (targeting different epitopes of Her2) and M1231 (targeting EGFR and UC1). Another common resistance mechanism is the efflux of effective payloads via ATP-binding cassette transporters. Many cytotoxic payloads used for ADCs may be substrates for these pumps, which can lead to drug efflux from target cells and reduced efficacy. Clinical data suggest that efflux pumps are one of the reasons for the reduced efficacy of gemtuzumab ozogamicin. Of course, any step in the action of ADC drugs can potentially lead to resistance: 1) defects in antibody internalization, transport, and recycling, 2) lysosomal degradation leading to drug release barriers, 3) alterations in cell death pathways (see the figure)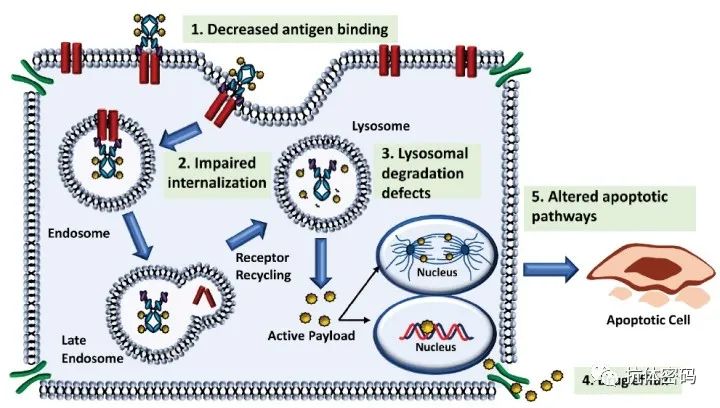 ADC resistance mechanisms05
ADC resistance mechanisms05
Important Considerations in ADC Design
1. Target Antigens Improving the safety and efficacy of ADCs largely depends on the selection of target antigens and their interactions. Two key parameters are involved in the selection of target antigens: tumor specificity and expression level. Ideally, the selected target should exhibit high tumor specificity or disease-specific expression, with minimal or no expression in normal tissues. The specificity of the target is crucial for reducing the toxicity of ADCs, thus playing an important role in the overall success of ADCs. The specificity of the target is crucial for reducing ADC toxicity and plays an important role in their overall success. From an oncology perspective, antigens can be expressed as surface receptors on tumor cells, tumor stem cells, or in the tumor vasculature and microenvironment. Ideally, antigens are uniformly expressed at similar levels across all tumor-associated cells. This allows ADC drugs to fully exploit the bystander effect and overcome tumor heterogeneity.2. Monoclonal Antibodies After selecting target antigens, antibodies need to be screened based on their ability to penetrate tumors and other factors. The ADCs currently under development and approval belong to IgG1, IgG2, or IgG4 subclasses. These subclasses differ in their cross-linking capabilities and biological activities, including ADCC and complement-dependent cytotoxicity (CDC). Compared to IgG2 and IgG4, IgG1 is used the most due to its stronger delivery capability and greater effector functions. However, when considering target characteristics or different mechanisms, in some cases, the effector functions of IgG1 such as ADCC and CDC need to be avoided, making IgG2 and IgG4 antibodies the preferred choice. Additionally, the choice of subclass significantly impacts conjugation, especially when considering the use of cysteine for conjugation.2.1. Size of Monoclonal Antibodies After selecting the antigen and antibody subtype, the size of the antibodies needs to be considered. Historically, full-length IgG antibodies were preferred, but these antibodies have certain limitations in cellular uptake and tumor penetration. To address this issue, new forms of antibodies have emerged, such as Fab-ADC and ScFv-ADC. These smaller antibodies have better permeability, but they lack Fc, resulting in a shorter half-life.2.2 Antibody Modifications Antibodies, like other proteins, can undergo modifications during production or storage (PTMs), such as deamidation, sialylation, or cleavage of C-terminal lysines. These modifications can affect the stability of antibodies, thereby influencing the stability and effectiveness of ADCs.2.3. Internalization of ADCs Most ADCs are designed to target antigens that show efficient internalization through receptor-mediated endocytosis, facilitating the entry of ADCs into cells after recognition. For a long time, receptor internalization has been a requirement for effective ADC design to minimize the impact of cytotoxic payload release on healthy cells. To design a successful internalizing ADC, the accessibility, density, internalization rate, and intracellular transport of the ADC must be evaluated. Generally, ADCs targeting antigens expressed on solid tumors face more physical barriers to overcome after administration compared to those targeting hematological malignancies. In hematological malignancies, targets are easily exposed to circulating ADCs. Additionally, targets can sometimes