
Let’s take a moment to focus on the recent hot topic of Antibody–Drug Conjugates and systematically learn about the review published in Cancers: Antibody–Drug Conjugates for the Treatment of Breast Cancer.
 Abstract
Abstract
Currently, aside from endocrine therapy and targeted drugs, the common treatment method for metastatic breast cancer (BC) is chemotherapy. However, the lack of tumor specificity and toxicity related to dose exposure limits the manageability of cytotoxic drugs. Antibody-drug conjugates (ADCs) enhance the therapeutic efficacy of anti-tumor drugs by combining the specificity of monoclonal antibodies with the cytotoxicity of chemotherapy. The most studied target antigen is HER2, such as trastuzumab deruxtecan, which shows activity not only in HER2-positive patients but also in HER2-low BC patients, possibly due to the bystander effect. This characteristic of providing cytotoxic effects to non-targeted cancer cells can overcome the tumor heterogeneity of certain target antigens.
Additionally, ADCs have made breakthroughs in triple-negative BC, as evidenced by the recent approval of sacituzumab-govitecan (injectable gosituzumab). In this review, we discuss the current prospects of ADC development for BC treatment and potential limitations. Among the 9 ADCs approved by the FDA, 3 are used for treating BC (see Figures 1 and 2).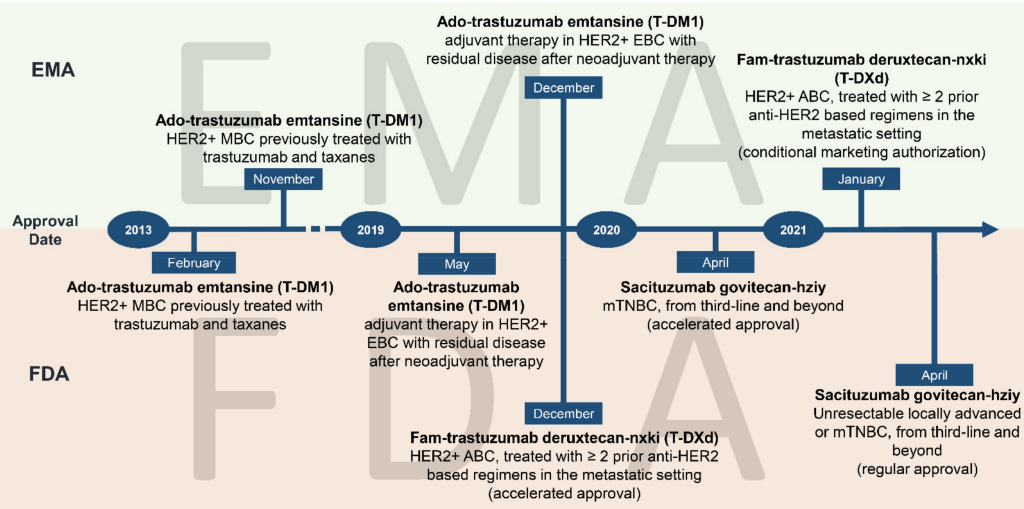 Figure 1 Milestones of ADCs approved by the FDA and EMA for BC treatment
Figure 1 Milestones of ADCs approved by the FDA and EMA for BC treatment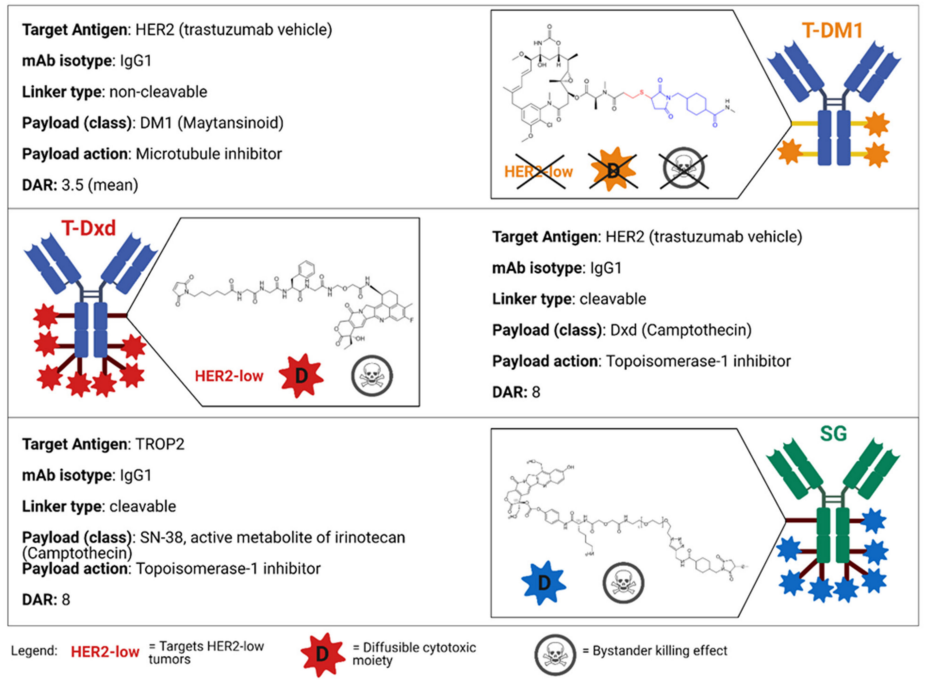
Figure 2 Main characteristics of FDA-approved ADC drugs for BC treatment
Since the discovery of HER2 from 1982 to 1984, it has triggered the characterization and research of targeted drugs for HER2-positive BC.The current summary of ADC drugs in the breast cancer field is as follows:
1. Trastuzumab Emtansine (T-DM1)
T-DM1 is the first ADC approved by the FDA. It is an anti-HER2 ADC that combines the anti-HER2 properties of trastuzumab with DM1 (a maytansinoid toxin that inhibits microtubule polymerization). The linker is an irreversible stable thioether, with a drug-to-antibody ratio (DAR) of approximately 3.5:1. PK studies show that the total serum concentration of trastuzumab (including conjugated antibody and free antibody) exceeds that of the intact ADC serum concentration by about 20%, with a lower concentration of the DM1 payload. The half-life of trastuzumab is 9-11 days, while the half-life of T-DM1 is about 4 days, possibly due to linker instability, antibody circulation, or hepatic clearance.
Preclinical data indicate that the anti-tumor properties of T-DM1 are (a) inhibiting HER2 signaling produced by trastuzumab by blocking ligand-independent HER2 dimerization; (b) in IgG1 backbone-induced ADCC; (c) in the cytotoxicity of HER2-expressing cells during internalization. The most common adverse reactions occur in up to 40% of patients, including nausea, fatigue, thrombocytopenia, diarrhea, and elevated liver levels. Especially with prolonged drug exposure, patients may also experience neuropathy. T-DM1 was initially approved by the FDA in 2013 for HER2-positive metastatic BC patients previously treated with trastuzumab and paclitaxel based on the results of the EMILIA trial. The results showed that patients treated with T-DM1 had improved progression-free survival (PFS) and overall survival (OS) compared to those treated with lapatinib and capecitabine. In later lines, T-DM1 significantly improved PFS and OS compared to physician’s choice treatment (TPC) (TH3RESA). Recently, T-DM1 has become the standard treatment for HER2-positive residual disease after neoadjuvant therapy (KATHERINE trial). As a first-line treatment, T-DM1 with or without pertuzumab is not inferior in terms of PFS compared to treatment with trastuzumab and paclitaxel for metastatic HER2-positive patients (MARIANNE trial). In this context, adding pertuzumab to trastuzumab and paclitaxel can extend PFS and OS, making T-DM1 still a second-line option. In neoadjuvant therapy, compared to T-DM1 with pertuzumab, docetaxel, carboplatin, and trastuzumab with pertuzumab increased the pathological complete response (pCR) rate. In summary, the development of T-DM1 as first-line treatment or neoadjuvant therapy for HER2-positive metastatic BC has not been satisfactory. The combination of HER2-targeted T-DM1 is under investigation in the CompassHER2-RD trial (NCT04457596) and HER2CLIMB-02 trial (NCT03975647), assessing the advantages of T-DM1 combined with tucatinib in the adjuvant and metastatic settings for previously treated patients. Regarding HER2-low metastatic BC, retrospective and exploratory studies have shown that T-DM1 has poor clinical efficacy in patients who have received at least trastuzumab treatment in two phase II trials. However, a prospective study of T-DM1 in the same environment of HER2-positive but heterogeneous BC was conducted. In a neoadjuvant phase II study of T-DM1 with pertuzumab, 10% of patients showed HER2 heterogeneity, with patients without HER2 heterogeneity achieving pCR, while 55% of HER2-homogeneous tumor patients achieved pCR.2. Fam-Trastuzumab Deruxtecan-Nxki (T-DXd)
T-DXd (DS-8201) is an ADC composed of anti-HER2 mAb trastuzumab and a cleavable linker based on a tetrapeptide. The payload is a topoisomerase I inhibitor (an exatecan derivative), with a DAR of 8:1, capable of delivering a high concentration of cytotoxic drugs.
T-DXd is currently approved in the United States and Japan for advanced or metastatic HER2-positive BC patients who have undergone at least two previous anti-HER2-based regimens, and it has also received conditional approval in Europe. (Recently, this product has achieved success, with FDA approval for adult breast cancer patients with low HER2 expression (IHC 1+ or IHC 2+/ISH-), detailed clinical developments can be found in the literature).3. Trastuzumab–Duocarmazine (SYD985)
Trastuzumab duocarmazine is a humanized anti-HER2 mAb (trastuzumab) linked to a duocarmycin payload via a cleavable linker (DAR, 2.8:1).
In fact, the cytotoxicity is a cell-permeable prodrug (seco-duocarmycin-hydroxy benzamide-azaindole, seco-DUBA), which is cleaved into an active toxin (DUBA) in the intracellular lysosome after internalization. The payload then alkylates DNA, causing DNA damage and cell death, also through bystander killing effects, possibly due to secreted tissue protease B from malignant cell stroma cleaving SYD985, generating free DUBA. Despite its lower DAR compared to T-DM1, SYD985 has shown higher activity than T-DM1 in HER2-low, patient-derived xenograft BC models. In a phase I study conducted on patients with refractory locally advanced or metastatic solid tumors and variable HER2 status, 47 low HER2 BC patients were included in the BC dose expansion cohort. Exploratory ADC showed ORR of 33%, 28%, and 40% for HER2-positive BC, HR-positive low-expressing HER2 BC, and HR-negative low-expressing HER2 BC, respectively, with encouraging results. Regarding safety, the most common treatment-related AEs are fatigue (33%), conjunctivitis (31%), and dry eye (31%, with 7% of patients experiencing grade 3 events). Notably, ocular toxicity predominates in the safety profile of SYD985 (Figure 3). In addition to the most common ocular AEs mentioned above, keratitis and blurred vision have also been reported. In the dose expansion cohort, 4 patients (3%) experienced grade 3 conjunctivitis. Reducing the dose, decreasing the administration frequency, or prophylactic use of eye drops does not seem to affect these AEs. Nevertheless, most patients were able to continue with SYD985, and most ocular issues improved, indicating that these AEs are manageable. In the SYD985 phase I study, a decrease in left ventricular ejection fraction (LVEF) was detected: 10 patients (7%) had grades 1-2, and 1 patient (3%) had grade 3. In 8 patients (5%), a report of an absolute decrease of at least 10% from baseline to below 50% was noted.
Figure 3 Toxicity profile observed in clinical trials of novel ADCs
SYD985 is also undergoing a phase III study (TULIP trial), in which it is compared with TPC in HER2-positive metastatic BC patients who have undergone at least two anti-HER2 regimens or progressed on T-DM1 (TULIP trial, NCT03262935).
4. Disitamab Vedotin (RC48-ADC)RC48-ADC is an ADC composed of anti-HER2 humanized mAb (disitamab) linked to four molecules of (DAR, 4:1) monomethyl auristatin E (MMAE) via a protease-cleavable linker. In a phase I study on HER2-positive metastatic BC patients, safety aspects included grade 3 neutropenia (10%), leukopenia (6.7%), and elevated transaminases (3.3%), with no grade 4 AEs (Figure 3).
Currently, a phase II study is elucidating the efficacy of RC48-ADC combined with capecitabine and lapatinib at a dose of 2 mg/kg every 2 weeks in HER2-positive metastatic BC (NCT03500380). A phase III randomized trial aims to evaluate the efficacy of RC48-ADC compared to TPC in HER2-low metastatic BC patients in first-line treatment or after progression (NCT04400695).
5. XMT-1522 (TAK-522)
XMT-1522 is an ADC targeting HER2 through mAb HT-19, which binds to a different HER2 epitope than trastuzumab. HT-19 is linked to the payload (an auristatin derivative) via a degradable cysteine bond, with a DAR of 12:1. XMT-1522 appears to trigger bystander killing effects and is more active than T-DM1 in HER2-positive and HER2-low expressing patient-derived xenografts and early clinical trials, although the development of this drug has been partially shelved due to safety concerns leading to an FDA clinical hold.
6. MM-302MM-302 mediates HER2-targeted release of high-dose anthracycline drugs while reducing exposure to healthy tissues (such as cardiomyocytes). The binding site of this drug is a different HER2 domain than that of trastuzumab.
Notably, preclinical evidence suggests a synergistic effect with the latter. Although phase I trials confirmed the activity of this ADC in pre-treated metastatic BC, unfortunately, the phase II HERMIONE trial has ended due to the lack of significant activity of MM-302 in combination with trastuzumab compared to TPC.
7. MEDI-4276This drug is a bispecific ADC targeting two different epitopes of HER2. The bispecificity may enhance internalization, thereby increasing payload release and enhancing killing of cancer cells. In MEDI-4276, the mAb is linked to a microtubule inhibitor (AZ13599185) via a cleavable linker (DAR, 4:1). Based on the activity observed in preclinical models, a phase I dose-escalation clinical trial is elucidating the role of this ADC in HER2-positive metastatic BC and gastric cancer.
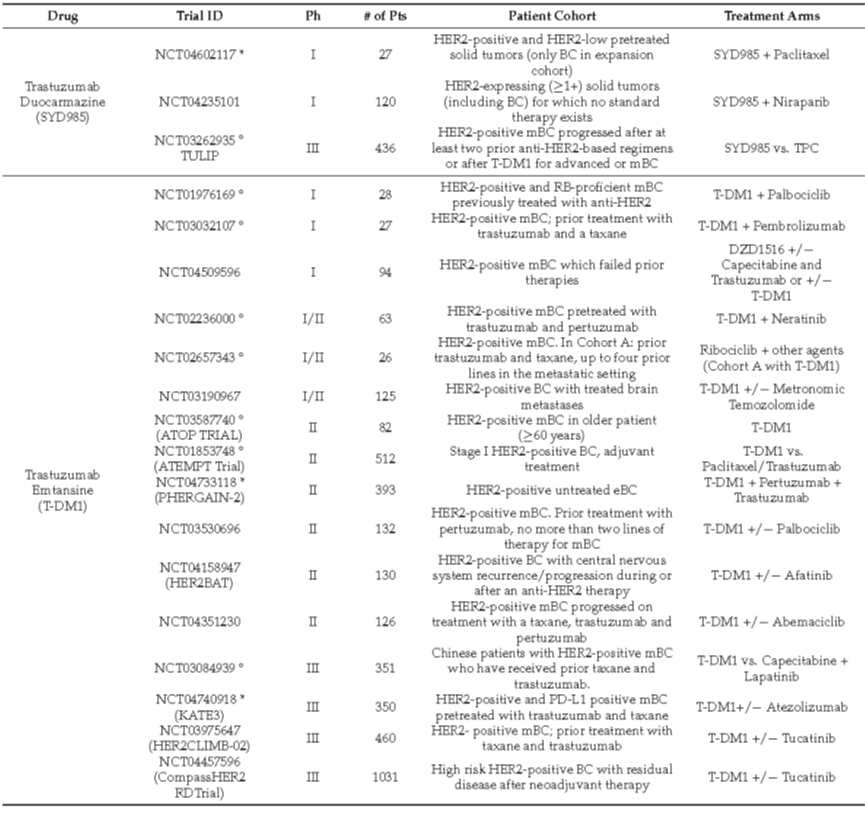
Notably, several other anti-HER2 ADCs are currently under investigation, including A166, ARX788, BAT8001, and PF-06804103, as shown in Table 1.
Table 1: Summary of current clinical trials of antibody-drug conjugates targeting HER2
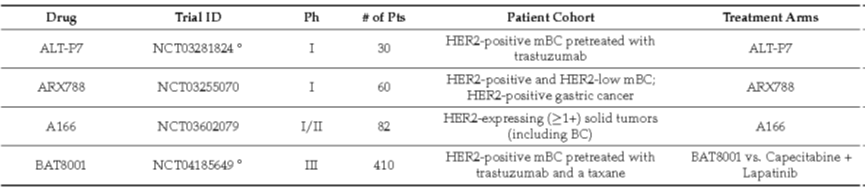
Table 1: Summary of current clinical trials of antibody-drug conjugates targeting HER2 (continued)
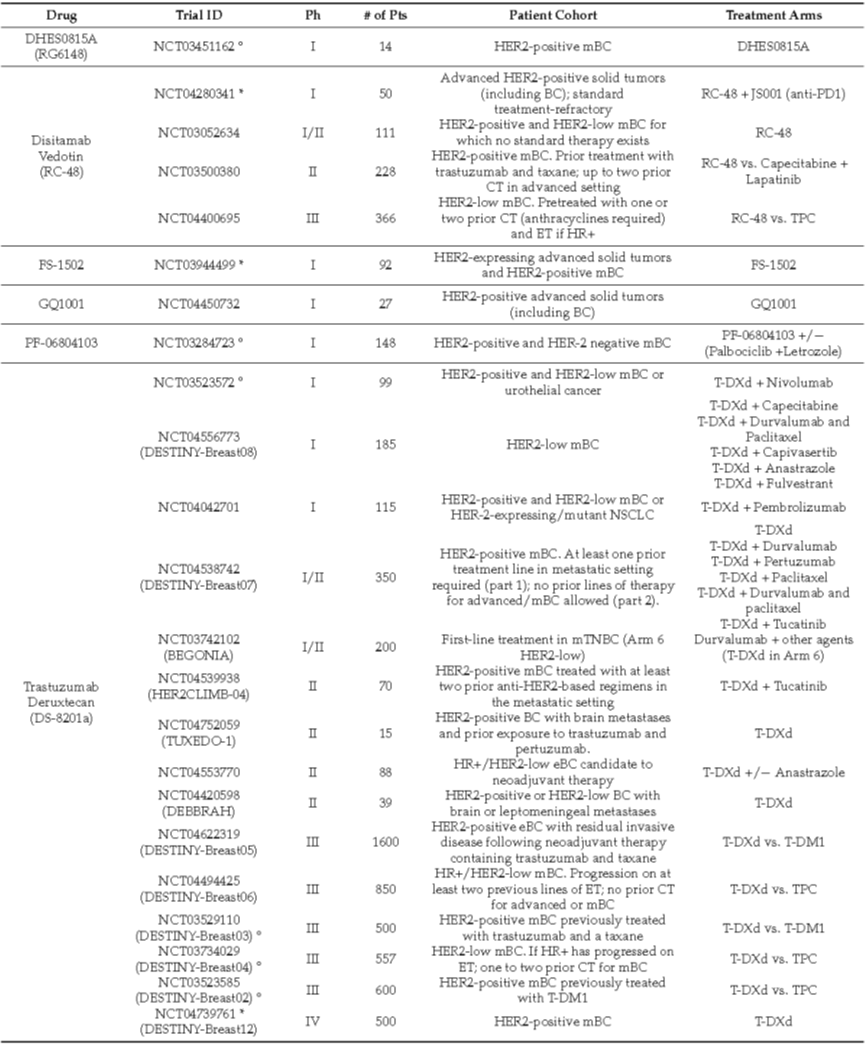
Table 1: Summary of current clinical trials of antibody-drug conjugates targeting HER2 (continued)
Other Targeted ADCs for BCTrop2Trop2 is encoded by the TACSTD2 gene, a transmembrane glycoprotein that serves as an intracellular calcium signaling transducer. Trop2 is expressed in many normal tissues, such as the uterus, skin, esophagus, bladder, oral mucosa, nasopharynx, and lungs.Trop2 is overexpressed in several epithelial tumors, including urothelial carcinoma, breast cancer, gynecological cancers, lung cancer, and gastrointestinal cancers, and is associated with poor prognosis. Although the exact role of Trop2 in cell signaling has not been elucidated, the major pathways associated with Trop2 are extracellular signal-regulated kinase/mitogen-activated protein kinase (ERK/MAPK) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB).Sacituzumab Govitecan (IMMU-132)Through a cleavable linker, ADC SG combines the humanized anti-Trop-2 mAb hRS7 IgG1k with the cytotoxic payload SN-38 (the active metabolite of topoisomerase I inhibitor) irinotecan (DAR, 7.6–8:1) (Figure 2). After antigen binding, the free or conjugated form of the mAb is internalized into the target cells and then transported to the lysosome.
The low pH found in the lysosome promotes the hydrolysis of the linker and the subsequent release of the payload. Due to the membrane permeability of SN-38, some drug molecules are also released into the tumor microenvironment, contributing to the killing of adjacent tumor cells (bystander effect).
Datopotamab Deruxtecan (Dato-DXd, DS-1062)
Dato-DXd is an ADC composed of humanized Trop-2 directed mAb, a tetrapeptide-based cleavable linker, and a topoisomerase I inhibitor payload (exatecan derivative). The first human phase I study, TROPIONPanTumor01 (NCT03401385), investigated its efficacy in patients with advanced solid tumors, including metastatic TNBC. Safety features included grade 3 AEs, including fatigue, mucosal inflammation such as stomatitis, decreased appetite, nausea, vomiting, constipation, infusion-related reactions, anemia, and cough. Notably, 14 patients in the lung cancer cohort experienced ILD, with 3 grade 5 events.
LIV1LIV-1 belongs to the family of transmembrane zinc transporters, part of the ZIP superfamily. In normal tissues, the expression of LIV-1 family is heterogeneous. Among this protein family, LIV1 (ZIP6) is typically present in hormone-regulated tissues, such as the breast, and its expression appears to be sensitive to estrogen levels.
In fact, LIV1 was first identified as an estrogen-induced gene in BC cell lines. It is then associated with node involvement in HR-positive BC. Besides BC, LIV1 has been detected in cervical and uterine tumors, prostate cancer, and pancreatic cancer, as well as melanoma.
Ladiratuzumab Vedotin (SGN-LIV1A)
Anti-LIV1 humanized mAb and MMAE payload linked via a cleavable linker constitute the ADC. This compound binds to the extracellular domain of LIV1 and is transported to the lysosome after internalization, releasing the cytotoxic payload through proteolysis. Apoptosis of cancer cells is achieved by inhibiting microtubule protein polymerization. Based on preclinical models, SGN-LIV1A may induce effective immunogenic cell death (ICD) in TNBC, thereby potentially enhancing the benefits of immunotherapy.
HER3 (ErbB3)
HER3 is a member of the HER family characterized by weak tyrosine kinase activity. To transduce signals downstream, HER3 must undergo heterodimerization. In this case, HER2 is the most important partner for dimerization. Other high-affinity ligands of HER3 are represented by neuregulin proteins (NRG-1 and NRG-2). Various cancer histologies overexpress HER3, including head and neck cancer, colorectal cancer, bladder cancer, melanoma, lung cancer, ovarian cancer, prostate cancer, and breast cancer. HER3 is thought to be associated with resistance to targeted therapies, not only against other receptors of the HER family but also against hormonal drugs and PI3K inhibitors. Finally, ERBB3 somatic mutations also show some oncogenic potential.
Patritumab Deruxtecan (U3-1402, HER3-DXd)Patritumab deruxtecan is a novel anti-HER3 ADC composed of humanized mAb patritumumab and deruxtecan mAb linked to the payload via a peptide-based cleavable linker.
This experimental compound has been studied in a phase I/II clinical trial that recruited heavily pre-treated HER3-positive metastatic BC patients and achieved promising results (NCT02980341) (Table 2). Patients with HER3-high/HR-positive/HER2-negative tumors were included in two cohorts receiving drug treatment at doses of 4.8 mg/kg or 6.4 mg/kg. In contrast, HER3-low/HR-positive/HER2-negative metastatic BC patients and HER3-high metastatic TNBC patients received 6.4 mg/kg of the ADC. At the cutoff date, the drug activity of 64 HER3-high/HR-positive/HER2-negative metastatic BC patients was assessable. In this group, the ORR was 30%, with 13% of patients receiving 6.4 mg/kg and 4.8 mg/kg treatment. In 31 HER3-low/HR-positive/HER2-negative metastatic BC patients and 31 HER3-high metastatic TNBC patients, the ORR was 33% and 16%, respectively (6.4 mg/kg).
The most common all-grade AEs are gastrointestinal (nausea, 85.7%; decreased appetite, 66.7%; vomiting, 54.8%; AST/ALT elevation, 47.6% and 45.2%, respectively) and hematologic toxicity (thrombocytopenia, 71.4%; neutropenia, 64.3%; leukopenia, 59.5%; anemia, 38.1%). Grade 3 AEs (15%) include thrombocytopenia (35.7%), neutropenia (28.6%), leukopenia (21.4%), and anemia (16.7%).
- Conclusion and Future Prospects
The advancements in ADC engineering and technology platforms have unlocked the production of new effective payloads and novel linkers, allowing for a new generation of ADCs with high DAR and strong bystander effects. In fact, membrane-permeable payloads combined with new cleavable linkers amplify the efficacy of bystander effects, potentially extending efficacy to heterogeneous tumors or those with homogeneous but low target expression. However, transitioning these drugs to early stages requires caution due to the potential risks of severe AEs, including ILD from trastuzumab deruxtecan and neutropenia or diarrhea from SG.
As for future prospects, new potential targets are being evaluated, such as proteins expressed in the tumor microenvironment or cancer stem cells. In this regard, prodrug conjugates have emerged as a new class of recombinant ADC prodrugs. They can circulate in an inactive form, typically activated by proteolytic cleavage by proteases. This optimization of payload delivery to tumor sites is believed to reduce off-target/toxicities. Delivery systems that substitute mAb scaffolds are also of interest. For example, centyrins, small cysteine-free scaffolds, exhibit excellent biophysical properties. They can be effectively internalized by cancer cells and allow binding in various locations. Overall, considering that several novel ADCs are in the final stages of clinical development, as phase III clinical trials progress, we may witness a shift from the current standard treatment based on systemic chemotherapy to targeted anti-cancer treatments based on ADCs, whether as monotherapy or in combination with other drugs. Nevertheless, the development of ADCs still faces “old” challenges, such as patient selection and biomarker assessment. Future research needs to address all these aspects to best utilize these drugs.
References:
Corti C, Giugliano F, Nicolò E, et al. Antibody–drug conjugates for the treatment of breast cancer[J]. Cancers, 2021, 13(12): 2898.
Disclaimer
“YaoDu” WeChat public account reprints the source from other public account platforms, and the main purpose is to share industry-related knowledge and convey the latest information. The copyright of images and articles belongs to the original author. If there is any infringement, please notify us in time, and we will delete the relevant information within 24 hours.