As early as 1913, Paul Ehrlich first proposed the concept of “magic bullets” and drug targeting. However, it wasn’t until the rapid development of antibody technology in the 1970s that the first antibody-drug conjugate (ADC) — Gemtuzumab ozogamicin (GO), targeting CD33, was approved by the FDA in 2000 for the treatment of acute myeloid leukemia (AML), thus opening the advanced path of ADC drugs as “magic bullets” in the field of tumor treatment.[1]
ADC drugs are composed of humanized or human monoclonal antibodies (mAb) linked to highly cytotoxic small molecules via linkers. The high-affinity specific antibodies can precisely target cancer cells while avoiding damage to normal tissue cells. Currently, all ADC antibodies are IgG molecules, which have the advantage of high affinity for target antigens and a longer half-life in the bloodstream, leading to increased accumulation at tumor sites. The appropriate linker needs to be stable in the blood circulation but able to rapidly release the active small molecule toxic drug when localized near or within tumor cells. Instability of the linker can lead to premature release of the small molecule toxic drug, causing damage to normal tissue cells; thus, the linker must possess suitable functional groups for conjugation, strong cytotoxicity, hydrophobicity, and stability under physiological conditions.[2]
By conjugating potent small molecule toxic drugs with monoclonal antibodies through linkers, the conjugates can utilize the targeting capability of monoclonal antibodies to specifically recognize tumor cell surface antigens, enter the cells via endocytosis, and release cytotoxic agents using intracellular proteases to kill tumor cells, thereby enhancing drug efficacy and increasing the “therapeutic window”.[3]
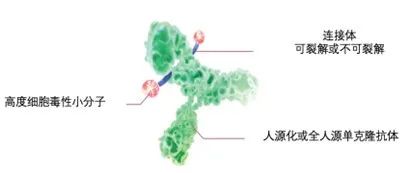 Figure 1: Structure of ADC Drugs
Figure 1: Structure of ADC DrugsCompared to traditional chemotherapy methods, ADC drugs represent a new treatment approach with tumor specificity and potency unattainable by conventional drugs. However, first-generation ADC drugs linked the lysine on the antibody to activated carboxylic acid esters via amide bonds, leading to instability in the bloodstream, thus limiting their practical clinical application.
Building on the exploration of using more effective small molecule toxic drugs (which have increased potency in killing tumor cells by hundreds of times compared to traditional cytotoxic drugs) such as Calicheamicin (also known as “Kahichamycin”), monoclonal antibody drugs have rapidly developed over the past decade, creating conditions for the emergence of second-generation ADC drugs. For ADC drugs to be effective, a threshold level of free small molecule toxic drug must be achieved within and around the tumor cells (i.e., IC50, half maximal inhibitory concentration). Factors such as target antigens, antibodies, linkers, and cytotoxic drugs can all affect this threshold, making them key to optimizing the conjugation and determining the performance of ADC drugs.[4]
Compared to the first generation, most second-generation ADC drugs have introduced more stable non-cleavable thioether linkers, improving drug plasma stability and reducing off-target toxicity, while also using more potent microtubule inhibitors or DNA-damaging agents to avoid reduced efficacy caused by low expression of target antigens and limited ADC delivery. These improvements have led to better stability and tolerability in the bloodstream, enhancing the therapeutic index of cytotoxic drugs.[5]
Currently approved second-generation ADC drugs include Inotuzumab ozogamicin (InO), Brentuximab vedotin, and Ado-trastuzumab emtansine. Among them, InO is a representative second-generation ADC drug in the treatment of hematological malignancies, having received FDA approval in 2017 for the treatment of adult relapsed/refractory precursor B-cell acute lymphoblastic leukemia.
InO consists of humanized IgG4, anti-CD22 monoclonal antibody, small molecule cytotoxic drugCalicheamicin and a cleavable linker dimethylhydrazine.
The anti-CD22 monoclonal antibody rapidly internalizes after binding to the CD22 antigen on the surface of tumor cells, releasing Calicheamicin inside the tumor cells, which binds to DNA, induces double-strand DNA breaks, and ultimately leads to tumor cell apoptosis.[6][7]
Microtubule inhibitors induce death in rapidly dividing tumor cells by interfering with mitosis and altering the cytoskeletal structure but have no effect on non-dividing or static tumor cells. Calicheamicin, as a DNA-damaging agent, disrupts DNA through double-strand breaks and other mechanisms, making its action independent of cell cycle processes, thus showing significant killing effects on both non-dividing and slowly dividing tumor cells.[8]
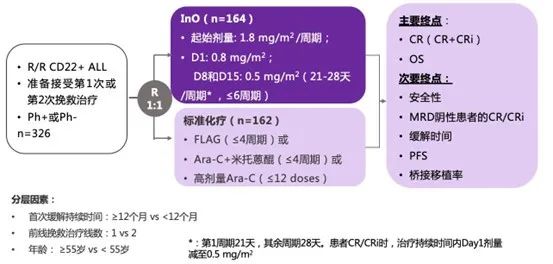 Figure 2: INO-VATE Study Design
Figure 2: INO-VATE Study Design
InO‘s target antigen is CD22, which studies have shownCD22 is an ideal target antigen for treating ALL.Because CD22 is specifically expressed in the majority (>90%) of B-cell ALL patients and not expressed in hematopoietic stem cells or other normal tissues, it greatly enhances the specificity of targeted therapy. Furthermore, CD19 is the target for BiTE and many CAR-T cell therapies, and the loss of the CD19 antigen is a common mechanism for relapse in these two treatments. However, even in cases of CD19 target loss, CD22 antigen can still be detected, allowing for the use of InO after relapse from BiTE and CD19-CAR-T therapies. CD22 does not enter the extracellular environment upon binding with ligands or antibody cross-linking but rapidly internalizes, making it an ideal target for ADC drug delivery of cytotoxic agents. The CD22-targeting InO has also shown excellent efficacy in clinical studies.[9]
INO-VATE study is the first global multicenter Phase III clinical trial evaluating the efficacy and safety of InO compared to standard chemotherapy (SoC) for R/R ALL. [10]
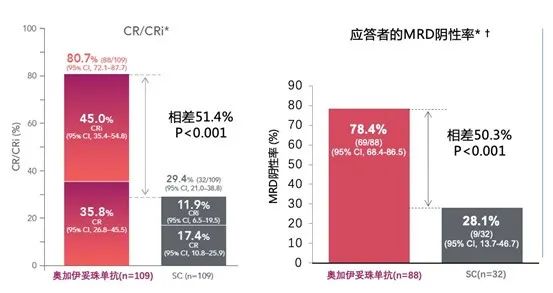
Figure 3: CR/CRi Rates and MRD Negative Rates Results of INO-VATE Study
Efficacy results show that InO compared to SoC
1. Achieved a higher CR/CRi rate (80.7% vs 29.4%; P<0.001)
2. Responding patients achieved a higher MRD negative rate (78.4% vs 28.1% P<0.001)
3. More patients received HSCT treatment (48.2% vs 22.2%)
4. Prolonged PFS (5.0 months vs 1.8 months; P<0.001)
5. Median OS extended (7.7 months vs 6.2 months; P=0.0105)
6. 2-year survival rate increased (23% vs 10%)
7. 3-year survival rate increased (20.3% vs 6.5%)
8. Significantly prolonged OS for patients regardless of tumor burden (HR 0.60; P=0.0335). Additionally, the median OS for bridging transplantation vs non-bridging transplantation was 12.6 months vs 7.1 months (P=0.0065), indicating that bridging transplantation can further enhance the survival benefits brought by InO.[10][11]
Regarding safety, the InO group had comparable safety to the SoC group, with manageable adverse events and good patient tolerability. In the Phase III INO-VATE ALL study, among the InO treatment group (n=164), 14% of patients experienced InO-related VOD; among InO group patients who did not receive SCT intervention during or after treatment, 3% (5/164) experienced VOD; among patients in the InO group who underwent subsequent SCT, 23% experienced VOD, most occurring within 3-57 days post-transplant (median time 15 days).[12][13]
However, in actual clinical practice, some preventive measures can be taken to reduce the incidence of VOD/SOS, such as considering delaying HSCT based on disease status, avoiding concomitant use of hepatotoxic drugs, prophylactic use of ursodeoxycholic acid, and reducing the intensity of allo-HSCT preconditioning for patients who have undergone multiple lines of treatment.[14]
Moreover, the incidence of ≥3 grade infections in the InO group was relatively low (InO 28% vs SoC 54%); the occurrence of ≥3 grade bone marrow suppression adverse events was also relatively low (e.g., thrombocytopenia InO 42% vs SoC 59%, anemia 24% vs 47%, leukopenia 33% vs 42%).[15]
Third generation ADC drugs utilize site-specific binding of small molecule drugs and monoclonal antibodies to produce uniform drug-antibody ratios (DARs) (with DARs of 2 or 4). Third-generation ADC drugs with consistent DARs show less off-target toxicity and better pharmacokinetic efficiency.
Globally, several Phase III ADC-related studies are currently underway, and ADCs show great potential in the treatment of solid tumors. We look forward to more exciting data emerging to benefit clinical practice.

Beibosa Product Manual PC Version >>
Beibosa Product Manual Mobile Version>>
1. Strebhardt K, Ullrich A. Paul Ehrlich’s magic bullet concept: 100 years of progress [J]. Nat Rev Cancer 2008;8(6):473-80. DOI: 10.1038/nrc2394.
2. Tsuchikama K, An Z. Antibody-drug conjugates: recent advances in conjugation and linker chemistries [J]. Protein Cell 2018;9(1):33-46. DOI: 10.1007/s13238-016-0323-0.
3. Dan N, Setua S, Kashyap VK, et al. Antibody-Drug Conjugates for Cancer Therapy: Chemistry to Clinical Implications [J]. Pharmaceuticals (Basel) 2018;11(2) DOI: 10.3390/ph11020032.
4. Panowski S, Bhakta S, Raab H, et al. Site-specific antibody drug conjugates for cancer therapy [J]. MAbs 2014;6(1):34-45. DOI: 10.4161/mabs.27022.
5. Beck A, Goetsch L, Dumontet C, et al. Strategies and challenges for the next generation of antibody-drug conjugates [J]. Nat Rev Drug Discov 2017;16(5):315-37. DOI: 10.1038/nrd.2016.268.
6. Advani A, Coiffier B, Czuczman MS, et al. Safety, pharmacokinetics, and preliminary clinical activity of inotuzumab ozogamicin, a novel immunoconjugate for the treatment of B-cell non-Hodgkin’s lymphoma: results of a phase I study [J]. J Clin Oncol 2010;28(12):2085-93. DOI: 10.1200/JCO.2009.25.1900.
7. Jabbour E, O’Brien S, Ravandi F, et al. Monoclonal antibodies in acute lymphoblastic leukemia [J]. Blood 2015;125(26):4010-6. DOI: 10.1182/blood-2014-08-596403.
8. Shor B, Gerber HP, Sapra P. Preclinical and clinical development of inotuzumab-ozogamicin in hematological malignancies [J]. Mol Immunol 2015;67(2 Pt A):107-16. DOI: 10.1016/j.molimm.2014.09.014.
9. Yurkiewicz IR, Muffly L, Liedtke M. Inotuzumab ozogamicin: a CD22 mAb-drug conjugate for adult relapsed or refractory B-cell precursor acute lymphoblastic leukemia [J]. Drug Des Devel Ther 2018;12:2293-300. DOI: 10.2147/DDDT.S150317.
10. Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab Ozogamicin versus Standard Therapy for Acute Lymphoblastic Leukemia [J]. N Engl J Med 2016;375(8):740-53. DOI: 10.1056/NEJMoa1509277.
11. Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard of care in relapsed or refractory acute lymphoblastic leukemia: Final report and long-term survival follow-up from the randomized, phase 3 INO-VATE study [J]. Cancer 2019;125(14):2474-87. DOI: 10.1002/cncr.32116.
12. Kantarjian HM, DeAngelo DJ, Advani AS, et al. Hepatic adverse event profile of inotuzumab ozogamicin in adult patients with relapsed or refractory acute lymphoblastic leukaemia: results from the open-label, randomised, phase 3 INO-VATE study [J]. Lancet Haematol 2017;4(8):e387-e98. DOI: 10.1016/S2352-3026(17)30103-5.
13. Pfizer Inc. Inotuzumab ozogamicin Summary of Product Characteristics. 2018.
14. Mohty M, Malard F, Abecassis M, et al. Sinusoidal obstruction syndrome/veno-occlusive disease: current situation and perspectives-a position statement from the European Society for Blood and Marrow Transplantation (EBMT) [J]. Bone Marrow Transplant 2015;50(6):781-9. DOI: 10.1038/bmt.2015.52.
15. Inotuzumab ozogamicin Injection Instructions (December 20, 2021)
*For academic reference only for healthcare professionals, not for medical advice or promotion.
Approval Number: PP-INO-CHN-0360
Expiration Date: 2023/11/7
Gathering Experts, Focusing on Clinical Practice
Welcome to follow CCMTV·Hematology Channel!
