The following article is sourced from Biotech Investment Notes, authored by Andy.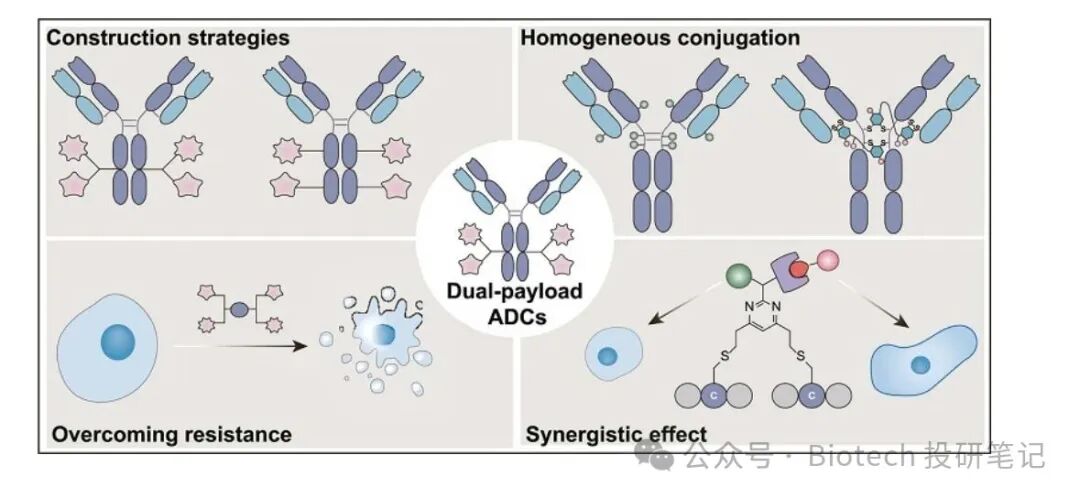
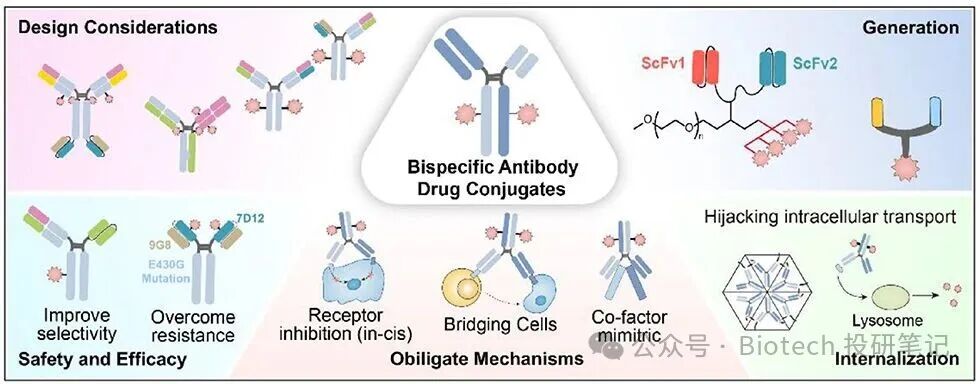
As the technology of ADCs (Antibody-Drug Conjugates) evolves from the “first generation” to the “new generation”, bispecific ADCs and dual payload ADCs have emerged as two major research directions in the industry, breaking through the traditional single-target, single-payload ADCs. Although both are designed around the core concept of “duality”, there are significant differences in their technical logic, advantageous scenarios, and clinical potential, especially in addressing the pain points of tumor treatment, showcasing different value propositions.The essential difference between the two technologies lies in their focus on different core components of the ADC: bispecific ADCs optimize “targeted delivery”, while dual payload ADCs enhance “tumor lethality”.

Core Advantage Comparison: Precise Delivery vs. Efficient LethalityThe advantages of the two correspond to different pain points in tumor treatment, with clear distinctions in clinical application scenarios.The core advantage of bispecific ADCs: Precision first, addressing the issue of “imprecise targeting”.1. Reducing off-target toxicity while enhancing on-target toxicity: The dual-target binding requires both targets to be expressed, which can reduce binding to normal cells that only express a single target, thereby lowering off-target toxicity while simultaneously increasing on-target toxicity.2. Covering heterogeneous tumors: Some tumors exhibit uneven target expression (e.g., some cells express target A while others express target B), and bispecific ADCs can bind to both targets simultaneously, covering more tumor cells and avoiding “missed kills”.3. Enhancing endocytosis efficiency: Some dual-target bindings (e.g., HER3/EGFR) can trigger stronger receptor dimerization, promoting faster internalization of the ADC by tumor cells and improving payload release efficiency.The core advantage of dual payload ADCs: Lethality first, addressing the issue of “inability to kill or penetrate”.1. Overcoming resistance to single payloads: Tumors can easily develop resistance to single mechanism payloads (e.g., only Topo1 inhibitors), while two different mechanism payloads (e.g., Topo1 inhibitor + microtubule inhibitor) require the tumor to escape both killing pathways, significantly raising the resistance threshold.2. Synergistically enhancing killing activity: Two payloads can act on different pathways of tumor cells (e.g., DNA damage + cell cycle arrest), producing a synergistic effect of “1+1>2”, achieving stronger anti-tumor effects even at lower doses of each payload.3. Adapting to a wider range of resistance scenarios: For patients who have developed resistance to traditional single payload ADCs (e.g., DS-8201, Sacituzumab govitecan), dual payload ADCs can provide new treatment options through a novel killing combination—this is one of the core unmet clinical needs today.Clinical Demand Adaptation: Dual Payload ADCs are more aligned with the core pain points of “resistant and difficult-to-treat tumors”.“Payload is the ultimate executor of ADC’s killing action,” and the biggest bottleneck in current tumor treatment is precisely “insufficient payload killing” or “resistance”—this gives dual payload ADCs a greater advantage in clinical demand matching, particularly reflected in the following two points:1. Clinical limitations of bispecific ADCs: Need to break through the “dose ceiling”.The core value of bispecific ADCs relies on the “targeting function of the bispecific antibody”, but this function has a key prerequisite: the bispecific must reach an effective therapeutic dose (RP2D).Due to the more complex production process and higher immunogenicity risk of bispecific antibodies, clinical practice often requires dose control to avoid toxicity from the antibodies themselves, leading to some bispecific ADCs not achieving the effective concentration for “dual-target synergistic binding”, thus failing to fully leverage their targeting advantages.2. Clinical irreplaceability of dual payload ADCs: Directly addressing the core pain point of “killing”.The ultimate goal of tumor treatment is to “effectively kill tumor cells”, and payloads are the direct tools to achieve this goal:• No alternative for resistance issues: For patients who have developed resistance to a single payload, bispecific ADCs cannot solve the fundamental problem of “payload failure” (no matter how precise the targeting, if the delivered payload is ineffective, it remains meaningless), while dual payload ADCs can directly bypass resistance pathways through complementary mechanisms.• Broader indications: Regardless of whether tumor target expression is uniform, as long as the payload can act on the core pathways of tumor cells (e.g., DNA repair, microtubule polymerization), dual payload ADCs can be effective without relying on the strict condition of “dual-target expression”, adapting to more difficult-to-treat solid tumors (e.g., advanced colorectal cancer, pancreatic cancer, etc.).Competitive Landscape and Future Directions: Complementary rather than adversarial, focusing on clinical value realization.Currently, both technologies are in the early stages of development, with no products approved for market yet, but the focus of research and development has shown differentiation:• Bispecific ADCs: More focused on scenarios of “target scarcity”, such as tumors with low expression or heterogeneous expression of both targets, attempting to open treatment windows through precise targeting, with representative companies including Amgen, BeiGene, and Antibody Biologics.• Dual Payload ADCs: More focused on “resistance” scenarios, especially targeting populations resistant to marketed single payload ADCs (e.g., HER2-positive breast cancer resistant to DS-8201), with representative companies including Chengdu Kanghong (KH815), Innovent Biologics (IBI3020), and Araris (three payload ADC). Below is the competitive landscape of bispecific dual payload ADCs.

In the future, the two will not be in a “this or that” competitive relationship, but may form a combination of “precise targeting + efficient lethality” (e.g., bispecific carrier + dual payload). However, given the current urgency of clinical needs, dual payload ADCs are more likely to achieve clinical breakthroughs in difficult-to-treat tumors by directly addressing the unmet core pain point of “resistance”—after all, for patients, “being able to kill resistant tumors” is more practically significant than “delivering ineffective drugs more precisely”.