Key Points
1
For patients with muscle-invasive bladder cancer (MIBC) who are not suitable for cisplatin treatment, sacituzumab govitecan and pembrolizumab show promise as alternatives to radical cystectomy, with a clinical complete response rate (cCR) of 44.4%.
2
The SURE-02 trial emphasizes bladder preservation, adjusting treatment plans based on patient preferences and treatment responses, shifting the focus from pathological complete response (pCR) to clinical complete response (cCR).
3
Preliminary biomarker data indicate that this regimen is effective in luminal subtype tumors, with TROP-2 expression associated with improved outcomes.
4
Future research aims to validate the effectiveness of clinical complete response (cCR) as a surrogate endpoint for survival, optimize patient selection using biomarkers, and refine bladder-preserving treatment strategies.
Introduction
The traditional standard treatment model for muscle-invasive bladder cancer (MIBC)—neoadjuvant chemotherapy combined with radical cystectomy—is undergoing a profound transformation. For patients who do not meet the criteria for cisplatin chemotherapy or who strongly resist cystectomy, they have long been trapped in a treatment dilemma of ‘no options available.’ While radical surgery may offer hope for a cure, it also comes with a significant decline in quality of life, such as urinary diversion, becoming a psychological and physiological barrier that many patients find hard to overcome.
Today, with the rapid development of precision medicine and immunotherapy, this deadlock is being broken. The preliminary results of the SURE-02 study, presented at the 2025 American Society of Clinical Oncology (ASCO) annual meeting, are like a stone thrown into a lake, creating ripples. This exploratory study reveals that the combination of the antibody-drug conjugate (ADC) sacituzumab govitecan and the immune checkpoint inhibitor pembrolizumab not only demonstrates exceptional antitumor activity but also pioneers a new bladder preservation strategy guided by ‘patient willingness’ and ‘treatment response,’ marking the official entry of MIBC treatment into a new era of personalization and humanization.
1. Efficacy Data Shines: The Combination Regimen Lays the Foundation for Bladder Preservation
The core of the SURE-02 study1 is to validate the efficacy of the combination regimen of sacituzumab govitecan and pembrolizumab. The reported clinical complete response (cCR) rate is as high as 44.4%, which is an exciting figure. cCR means that no signs of tumor are found through imaging and clinical biopsy. Crucially, all patients who achieved cCR and chose to preserve their bladder maintained a 100% rate of no metastatic survival during subsequent follow-ups. This means that for nearly half of the responders, this non-surgical therapy successfully controlled the systemic progression of the disease, reducing the risk of fatal metastasis to zero. Although local bladder recurrence still occasionally occurs (with 2 cases reported in the study), this provides clear direction and opportunity for subsequent local consolidation treatment. These strong preliminary data provide solid initial evidence for the effectiveness and safety of the bladder preservation strategy, giving doctors and patients confidence to explore this new path.
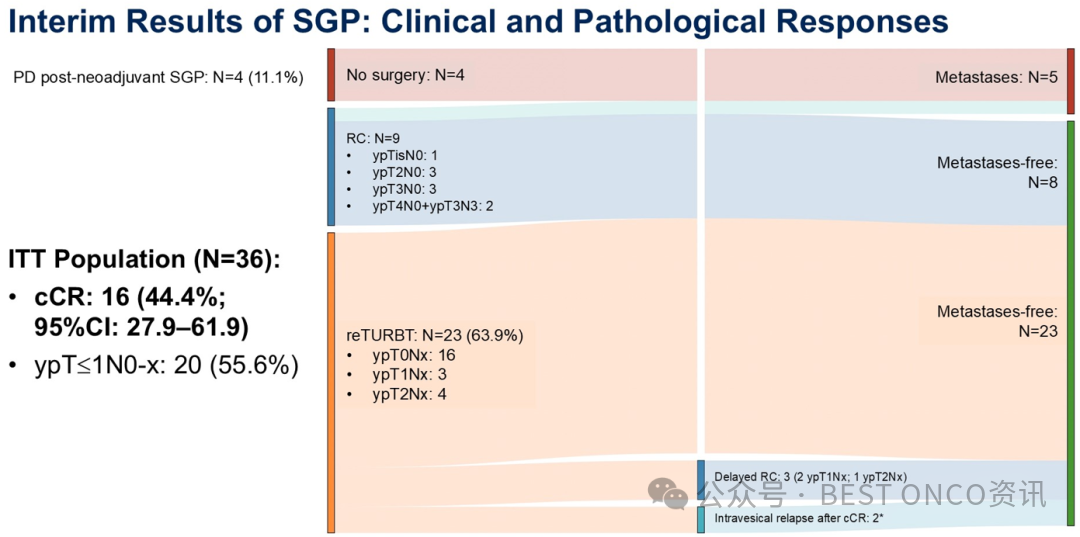
Figure 1 Mid-term results of the SURE-02 study
2. Core Strategy Shift: From ‘Pathological Gold Standard’ to ‘Clinical New Endpoint’ and ‘Shared Decision-Making’
The SURE-02 study’s other revolutionary contribution lies in its shift in treatment philosophy. The study was initially designed as the traditional ‘neoadjuvant therapy + surgery’ model. However, during the trial, researchers keenly observed that the vast majority of patients who responded well to treatment strongly questioned the necessity of continuing with radical surgery. Based on respect for patient preferences, the researchers decisively modified the trial protocol, introducing a ‘response-adaptive bladder preservation’ strategy. That is, after neoadjuvant combination therapy, a multidisciplinary team (MDT) evaluates and provides patients with full informed consent. If patients achieve cCR (imaging negative + biopsy negative) and wish to preserve their bladder, they can forgo immediate cystectomy and instead receive re-TURBT and subsequent pembrolizumab maintenance therapy.
This shift has changed the primary focus of the study from the traditional pathological complete response (pCR)—which means no tumor cells in the surgically removed bladder specimen—to clinical complete response (cCR). While pCR is the gold standard, achieving it requires sacrificing the bladder. cCR, as a non-invasive or minimally invasive assessment method, makes it possible to evaluate efficacy in vivo and develop strategies for organ preservation accordingly. This truly realizes a transformation in treatment decision-making from ‘physician-led’ to ‘shared decision-making’ and even ‘patient preference-driven.’
3. Dawn of Precision Medicine: Biomarkers Guide Optimal Beneficiary Population
No outstanding treatment regimen can benefit all patients, so identifying the population most likely to benefit is crucial. The preliminary biomarker analysis of the SURE-02 study has provided valuable insights. The study found that patients with luminal subtype bladder cancer seem to respond better to this combination regimen. This finding is significant because this subtype typically responds poorly or is resistant to simple immune checkpoint inhibitors (such as pembrolizumab). This strongly suggests that sacituzumab govitecan plays a key role in overcoming immune resistance.
Further analysis confirmed that high expression of TROP-2 is associated with better event-free survival, and high TROP-2 expression is enriched in luminal tumors that achieve cCR. Additionally, classic immunotherapy-related biomarkers such as high tumor mutation burden (TMB) and ARID1A gene mutations also indicate a good response to this combination regimen. These data reveal potential biomarkers associated with the efficacy of TROP-2 directed ADC for the first time, laying a scientific foundation for future precise patient selection and achieving ‘advantageous population’ precision treatment. In the future, we may be able to simply determine whether an MIBC patient is suitable for this bladder preservation regimen based on tumor molecular typing or TROP-2 expression levels.
4. The Road Ahead: Optimizing Strategies and Validation Exploration
Despite the bright prospects, the SURE-02 study is still in its early stages, and there is a long road ahead to explore. Future research directions will focus on several aspects: ① validating the surrogate endpoint status of cCR: larger studies and longer follow-up times are needed to confirm whether the bladder preservation strategy based on cCR can ultimately translate into long-term survival rates comparable to radical surgery, thereby establishing the effectiveness of cCR as a surrogate endpoint. ② optimizing treatment regimens and patient selection: how to further increase the cCR rate from 44% to 50% or even higher? The answer lies in more refined patient screening (relying on the aforementioned biomarkers) and optimization of treatment regimens, including treatment cycles, duration of maintenance therapy, and whether it is safe to de-escalate treatment for those who respond well. ③ strengthening local control: addressing the ‘shortcoming’ of local recurrence in the bladder, research needs to explore the addition of local consolidation treatments, such as new bladder instillation systems. This ‘systemic + local’ combination model is expected to further consolidate efficacy and completely eliminate concerns about local recurrence. ④ introducing more sensitive monitoring tools: such as circulating tumor DNA (ctDNA) dynamic monitoring, which is expected to provide earlier warnings of recurrence risk before abnormalities are detected by imaging or cystoscopy, thus achieving ultra-early intervention.
Conclusion
The significance of the SURE-02 study goes far beyond proposing a new drug combination. It represents a fundamental shift in treatment paradigms: from the past ‘one-size-fits-all’ mandatory surgery to a highly individualized and humanized medical model centered on patient quality of life, personal willingness, and treatment response. It proves that for a portion of precisely selected MIBC patients, ‘cure’ and ‘bladder preservation’ are no longer a binary choice. The powerful combination of ADC and immunotherapy has successfully opened the door to bladder preservation treatment. Meanwhile, the in-depth study of biomarkers provides us with a compass to guide the direction.
Although the current results are still preliminary, they undoubtedly ignite a new ray of hope. Future research will continue to focus on ‘how to do better, more precisely, and more steadily,’ with the ultimate goal of allowing every MIBC patient to have the right to choose a higher quality of life while ensuring survival, truly achieving a win-win of ‘life’ and ‘living.’ This is not only a technological advancement but also a return to the humanistic spirit of medicine.
References:
1. Necchi A, Jong J, Raggi D, et al. First results of SURE-02: A phase 2 study of neoadjuvant sacituzumab govitecan (SG) plus pembrolizumab (Pembro), followed by response-adapted bladder sparing and adjuvant pembro, in patients with muscle-invasive bladder cancer (MIBC). J Clin Oncol. 2025;43(suppl 16):45.
*This material is for the reference of healthcare professionals only and should not be distributed to non-healthcare professionals.
Copyright Statement: All articles signed as original are copyrighted by BEST ONCO. Personal forwarding and sharing are welcome. Any other media or website wishing to reproduce or quote content owned by this website must prominently indicate ‘Reprinted from BEST ONCO.’ This platform aims to help healthcare professionals better understand the latest developments in related disease fields. The information is for healthcare professionals to understand and cannot replace professional medical guidance, nor should it be considered as medical advice. If this information is used for purposes other than understanding, this platform and the author bear no related responsibility.