▲ Multiple benefits are coming, click to make an appointment
Surrogate endpoints (such as PFS, ORR) are significant in clinical trials for tumors, as they can accelerate the drug approval process, allowing patients to receive effective treatments more quickly.PFS has long been considered an effective surrogate endpoint for OS in chemotherapy trials for advanced solid tumors. However, with the emergence of immunotherapy such as ADC, there is limited research on whether PFS or ORR can effectively serve as surrogate endpoints for OS. Recently, clinical research teams from Europe and the United States conducted a comprehensive analysis of the currently disclosed ADC clinical trials, showing that PFS has a strong correlation with the final OS, theoretically allowing it to serve as a surrogate endpoint, while the effectiveness of ORR as a surrogate endpoint is related to the type of tumor. Importantly, in August of this year, the FDA released a draft guideline on the assessment of overall survival in cancer clinical trials, clearly stating that: where feasible, overall survival (OS) should be the primary endpoint of clinical trials. Even if OS is not the primary endpoint, pharmaceutical companies must collect and submit survival data to support the final evaluation of drug safety and efficacy. This indicates that future applications for tumor drugs will become more stringent.
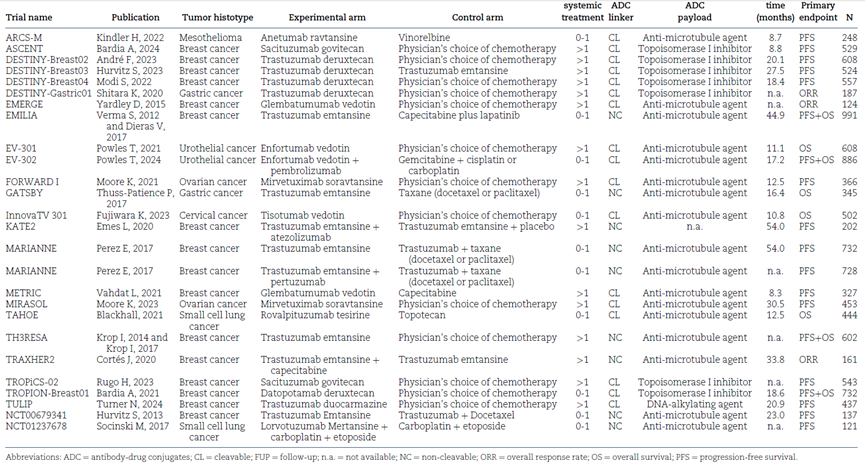
Overall, the study included a total of 25 randomized controlled trials (RCTs), with a total of 11729 patients. Tables 1 and S1 show the main characteristics of the included trials. The years of clinical result disclosures ranged from 2012 to 2024. 4 studies were conducted in the first-line treatment setting, while 21 were conducted in subsequent lines of treatment. OS was the primary endpoint in 4 clinical trials, PFS was the primary endpoint in 14 clinical trials, and ORR was the primary endpoint in 3 clinical trials. Both PFS and OS were common primary endpoints in 4 clinical trials.
The median follow-up time (FUP) ranged from 7 to 54 months, with sample sizes ranging from 121 to 991 patients. One trial had three treatment groups, resulting in a total of 26 treatment comparisons. 21 studies compared the efficacy of ADC as a monotherapy, while 5 clinical comparisons evaluated ADC in combination with the following drugs: atezolizumab for breast cancer patients, capecitabine or pertuzumab; for urothelial carcinoma patients, pembrolizumab; or for small cell lung cancer patients, carboplatin and etoposide. 16 comparisons tested ADC in advanced breast cancer patients.
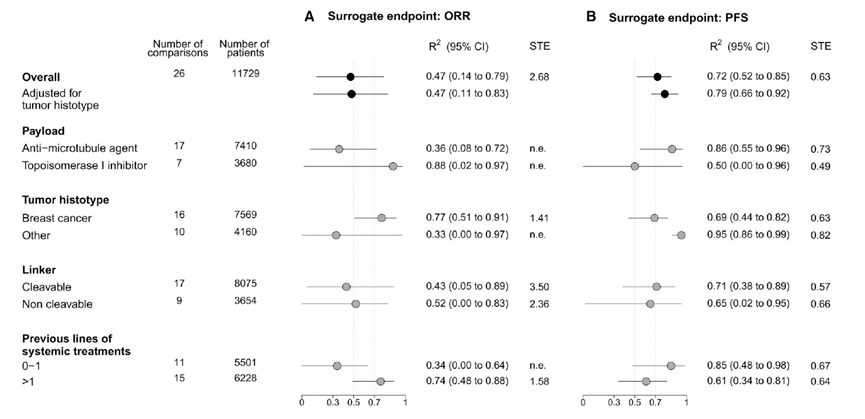
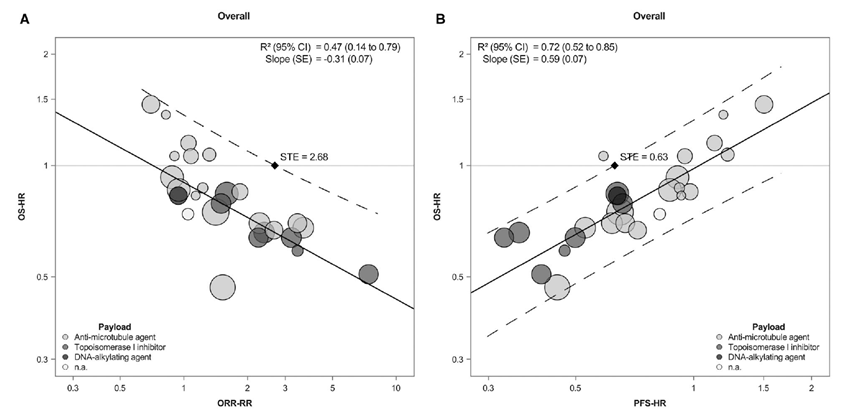
Researchers estimated regression equations based on all comparison data to assess the impact of treatment on OS and the association with the surrogate endpoint ORR. The relative risk (RR) of ORR and the hazard ratio (HR) for OS showed a slight to moderate association: R² was 0.47 (95% CI = 0.14 to 0.79), with a slope of the regression line of -0.31. After adjusting for tumor type, the association between the two treatment effects did not change substantially (adjusted R² = 0.47; 95% CI = 0.11 to 0.83;).
In subgroup analyses, the strength of the association between ORR-RR and OS-HR varied from poor to moderate in most explored subgroups, but there was a notable exception in the trial testing ADC for breast cancer, where R² was 0.77 (95% CI = 0.51 to 0.91, indicating a potentially strong association.
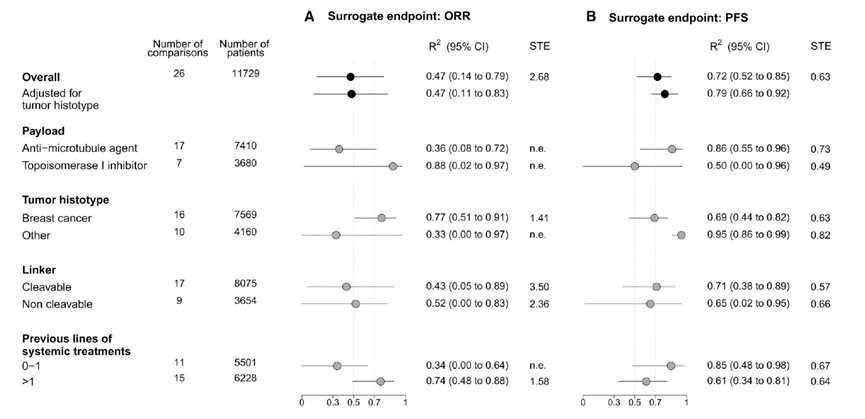
PFS-HR and OS-HR showed a strong association: R² was 0.72 (95% CI = 0.52 to 0.85, with a slope of the regression line of 0.59 (Figures 1 and 2, B). In the tumor type-adjusted model, R² was higher at 0.79 (95% CI = 0.66 to 0.92; Figure 1).LOOCV analysis confirmed this result, providing a cross-validated adjusted R² value of 0.69 (Figure S2, B). In subgroup analyses, the strength of the association between PFS-HR and OS-HR varied from moderate to strong (Figure 1 and Figures S3-S6).
The surrogate threshold effect (STE) for PFS or ORR for OS was calculated. For PFS-HR, the overall STE was 0.63, ranging from 0.49 to 0.82 in different exploratory subgroups. For ORR-RR, due to the observed weak association between ORR and OS, the overall STE reached as high as 2.68, and could not be estimated in all exploratory subgroups, except in comparisons testing ADC for breast cancer, using cleavable linker (CL), using non-cleavable linker (NC) or previously treated with >1 lines of systemic therapy, where the STE were 1.41, 3.50, 2.36 and 1.58.
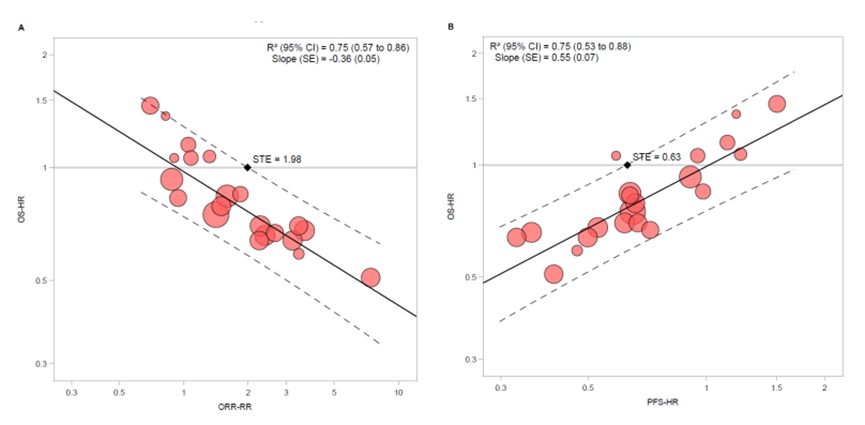
At the same time, the researchers conducted a sensitivity analysis, retaining only the 21 comparisons where ADC was administered as a monotherapy. The results showed that ORR-RR (R² = 0.75; 95% CI = 0.57 to 0.86) and PFS-HR (R² = 0.75; 95% CI = 0.53 to 0.88) both showed strong substitutability.
Summary
PFS is a strong surrogate endpoint for OS: The study confirms that in ADC clinical trials, progression-free survival (PFS) is a very reliable surrogate endpoint for overall survival (OS). Its coefficient of determination R² = 0.79 meets the strong correlation standard recommended by international guidelines (>0.7), and the results are consistent across various subgroup analyses of different patient populations and ADC drug characteristics. In contrast, the association of objective response rate (ORR) with OS is weaker (R² = 0.47), indicating that tumor shrinkage alone is insufficient to reliably predict survival benefits. The only exception is in the breast cancer subgroup, where ORR shows a strong substitutability (R² = 0.77). This study provides strong evidence to support regulatory agencies in accelerating the approval of new drugs based on positive PFS results for ADC. It also raises warnings against accelerating approvals based solely on high ORR (such as trastuzumab deruxtecan for all HER2 positive tumors).
Scan the WeChat QR code to add the Antibody Circle editor, and eligible individuals can join the Antibody Circle WeChat group!Please indicate: Name + Research Direction!

All articles reproduced by this public account are for the purpose of conveying more information, and the source and author are clearly indicated. Media or individuals who do not wish to be reproduced can contact us ([email protected]), and we will immediately delete the content. All articles represent the author’s views and do not represent the position of this site.