Patients with cholangiocarcinoma (BTC) have a very poor prognosis. In recent years, both the incidence and mortality rates have shown a continuous upward trend. BTC mainly includes gallbladder cancer (GBC) and cholangiocarcinoma (CCA), which can be broadly divided into two subtypes: intrahepatic cholangiocarcinoma (ICC) and extrahepatic cholangiocarcinoma (ECC). It is well known that clarifying the specific molecular mechanisms of ICC and ECC is helpful for early diagnosis and precise treatment, thereby improving patient prognosis¹. To standardize the precise diagnosis and treatment of CCA, the Guidelines Working Committee of the Chinese Society of Clinical Oncology has compiled the “2022 Edition of the Chinese Society of Clinical Oncology (CSCO) Guidelines for Cholangiocarcinoma” (hereinafter referred to as the “Guidelines”), aimed at conveying the latest research progress in BTC and providing the most authoritative evidence support for the diagnosis and treatment of BTC patients.
Expert Introduction
Professor Zhou Jun
-
Deputy Chief Physician of Gastroenterology, Peking University Cancer Hospital, Doctor of Oncology
-
Member of the Pancreatic Cancer Professional Committee of the Chinese Anti-Cancer Association (CSPAC)
-
Secretary of the CSCO Gastrointestinal Stromal Tumor Expert Committee
-
Secretary of the Gastrointestinal Tumor Subcommittee of the Chinese Society of Geriatric Oncology
-
Secretary of the Chinese Clinical Research Collaboration Group for Gastrointestinal Tumors
-
Member of the Editorial Team for the “Colorectal Cancer Diagnosis and Treatment Guidelines” by the Ministry of Health
-
Focusing on standardized and individualized treatment of gastrointestinal tumors for ten years
Screening and Diagnosis of Cholangiocarcinoma
BTC patients are relatively rare, accounting for about 3% of all digestive system tumors. The vast majority of BTC are adenocarcinomas, which are highly invasive and are often diagnosed at an advanced stage, resulting in a very poor prognosis, with a 5-year survival rate of less than 5%. Currently, the global incidence of BTC is on the rise, particularly common in Asian countries.
Guidelines Recommend: Emphasize the Collection of Clinical Data, Highlighting the Importance of Imaging and Pathological Histological Auxiliary Examinations
Interpretation 1: Histopathological and/or Cytological Examination is the Gold Standard for Diagnosing BTC
Ultrasound, serum CEA and CA19-9, multi-phase enhanced CT or MRI of the abdomen and pelvis, chest CT, magnetic resonance cholangiopancreatography (MRCP), ERCP, and exfoliative cytology tests are important for the diagnosis of CCA, the formulation of treatment plans, and the evaluation of therapeutic efficacy. Histopathological and/or cytological examination is the gold standard for diagnosing BTC. Based on patient stratification, the Guidelines provide targeted diagnostic and efficacy evaluation recommendations to guide and assist clinical physicians².
Table 1 Screening and Diagnosis of CCA

Interpretation 2: For Mass-Type ICC, FGFR2 Break Probe FISH Testing and IDH1/2 First-Generation Sequencing are Recommended
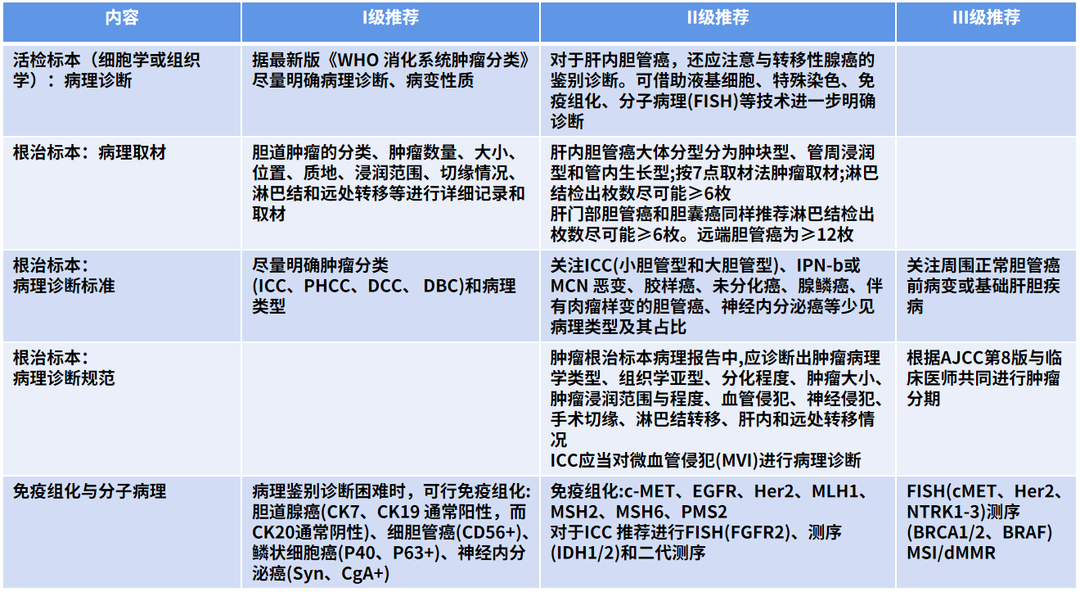
Immunohistochemistry is an indispensable test in the pathological differential diagnosis of cholangiocarcinoma, such as cholangiocarcinoma (CK7, CK19 usually positive, while CK20 usually negative), small duct carcinoma (CD56+), squamous cell carcinoma (P40, P63+), and neuroendocrine carcinoma (Syn, CgA+). Additionally, immunohistochemistry can detect some targets for targeted therapy or immunotherapy, including c-MET, EGFR, Her2, MLH1, MSH2, MSH6, PMS2, etc. Detection of MLH1, MSH2, MSH6, and PMS2 protein expression can determine MMR status and can also perform molecular tests such as MSI.For ICC, especially mass-type ICC, it is recommended to also perform FGFR2 break probe FISH testing and IDH1/2 first-generation sequencing, or to conduct second-generation sequencing tests. Patients who have not undergone second-generation sequencing can also conduct FISH testing for c-MET, Her2, NTRK1-3 and first-generation sequencing: BRCA1/2, BRAF, etc.².
Table 2 Pathological Diagnosis of BTC

First-Line Treatment for Advanced Cholangiocarcinoma
Guidelines Recommend: For Patients with Advanced Cholangiocarcinoma, Systemic Treatment Should be Administered
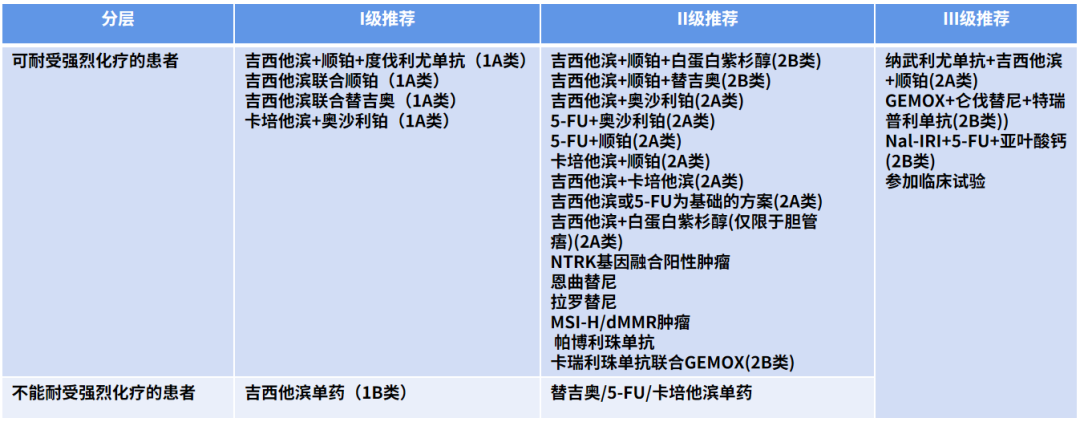
For patients who can tolerate aggressive chemotherapy, the preferred first-line treatment regimens for advanced BTC include Gemcitabine + Cisplatin + Durvalumab, Gemcitabine + Tegafur/Cisplatin, and Capecitabine + Oxaliplatin. Other first-line treatment regimens include chemotherapy regimens based on albumin-bound Paclitaxel, 5-fluorouracil (5-FU) + platinum, etc. This year’s guidelines include the addition of Gemcitabine + Cisplatin + Durvalumab regimen as a first-line treatment based on the results of the TOPAZ-1 study. It is recommended that all BTC patients who meet the criteria for precision medicine participate in clinical research, including but not limited to FGFR2 fusion mutations, IDH1/2 mutations, POLE/POLD mutations, BRCA mutations/BAP mutations/ATM mutations, BRAF mutations, etc.².
Table 3 First-Line Treatment for Advanced BTC
Interpretation: The Addition of Gemcitabine + Cisplatin + Durvalumab Regimen as a First-Line Treatment (Class 1A Evidence, Level I Recommendation)
The TOPAZ-1 study shows that Durvalumab combined with Gemcitabine and Cisplatin improved the overall survival (OS) of patients with advanced BTC from 11.5 months to 12.8 months, and progression-free survival (PFS) from 5.7 months to 7.2 months.
Second-Line Treatment for Advanced Cholangiocarcinoma
Guidelines Recommend: For Patients with Advanced Cholangiocarcinoma in the Second-Line, Provide Precision Stratified Treatment, Actively Attempt Targeted Therapy
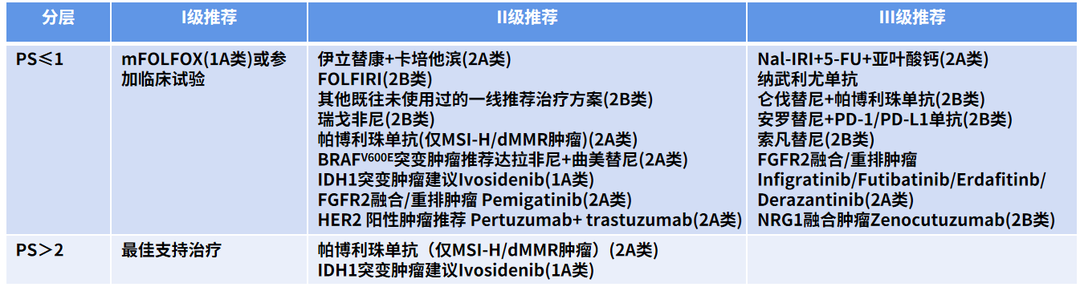
Oxaliplatin + 5-FU (mFOLFOX) is the standard second-line treatment regimen for patients with ECOG PS ≤ 1. Other second-line treatment regimens include Regorafenib, Pembrolizumab (only for MSI-H/dMMR tumors), and for BRAFV600E mutation tumors, Dabrafinib combined with Trametinib, and for patients with IDH1 mutation, Ivosidenib (lvosidenib). This year’s guidelines include the addition of Pemigatinib for the treatment of FGFR2 fusion/rearrangement tumors (Level II Recommendation); based on the MyPathway study results, the addition of Pertuzumab + Trastuzumab for HER2 positive tumors (Level II Recommendation)².
Table 4 Second-Line Treatment for Advanced BTC
Interpretation 1: Ivosidenib Included in the Second-Line Treatment Regimen for Advanced BTC with IDH1 Mutation (Class 1A Evidence, Level II Recommendation)
The ClarIDHy study is a global multicenter phase III clinical trial aimed at evaluating the efficacy and safety of Ivosidenib compared to placebo in patients with unresectable or metastatic IDH1 mutant cholangiocarcinoma. Advanced IDH1 mutant cholangiocarcinoma patients enrolled in the study were randomly assigned in a 2:1 ratio to receive either the IDH1 inhibitor Ivosidenib (500mg PO QD) or placebo treatment.
As of May 31, 2020, the study enrolled a total of 187 patients, who were randomly assigned to Ivosidenib (n=126) or placebo treatment (n=61); the results showed that the median PFS for the Ivosidenib group and placebo group were 2.7 months vs 1.4 months, and OS were 10.3 months vs 5.1 months, with the longest treatment duration in the Ivosidenib group being 34.4 months, while the placebo was 6.9 months, with median treatment durations of 2.8 months vs 1.6 months, and the differences were statistically significant.
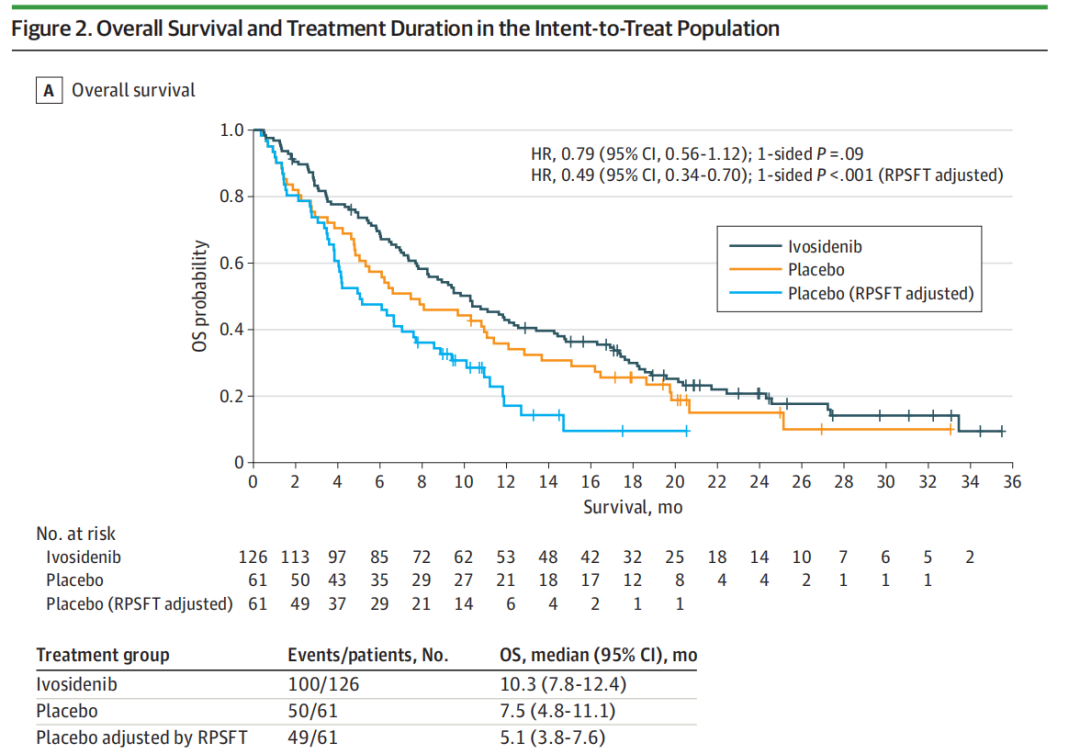
Figure 1 ClarIDHy Study OS Results
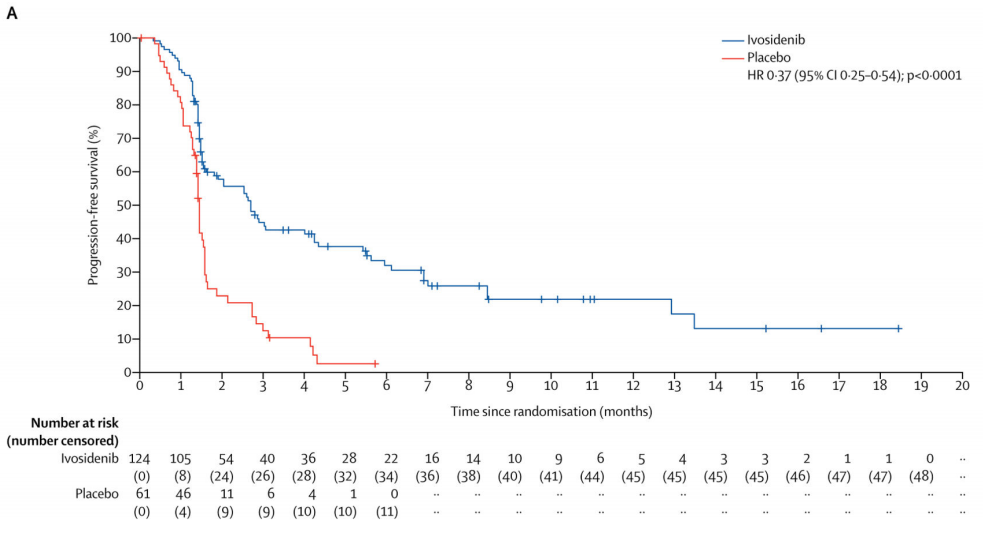
Figure 2 ClarIDHy Study PFS Results
The Ivosidenib group showed good tolerability compared to the placebo group, with ≥ Grade 3 adverse events during treatment being ascites, and no treatment-related deaths were observed. The decline in physical function in the Ivosidenib group was significantly less than that in the placebo group, proving that Ivosidenib provides better survival and is safe and controllable for patients with advanced IDH1 mutant cholangiocarcinoma³⁻⁴.
Interpretation 2: Regorafenib Included in the BTC Second-Line Treatment Regimen (Class 2B Evidence, Level II Recommendation)
The REACHIN study enrolled patients with advanced cholangiocarcinoma who progressed after first-line Gemcitabine combined with platinum chemotherapy, randomly assigning them to Regorafenib or placebo groups. The results showed that the median PFS for the Regorafenib group and placebo group were 3.0 months vs 1.5 months, with statistically significant differences, but there was no significant difference in OS between the two groups, thus making it a Level II recommendation.
Interpretation 3: Dabrafinib Combined with Trametinib Included in the Second-Line Treatment Regimen for Advanced BTC with BRAFV600E Mutation (Class 2A Evidence, Level II Recommendation)
A phase II single-arm multicenter study enrolled patients with advanced or recurrent cholangiocarcinoma with BRAFV600E mutation who had failed systemic treatment, all patients received Dabrafinib and Trametinib treatment until disease progression or treatment intolerance. Among the 43 enrolled patients, 22 achieved disease remission, with an ORR of 51%.
Interpretation 4: Addition of Pemigatinib Included in the Second-Line Treatment Regimen for Advanced BTC with FGFR2 Fusion/Rearrangement (Class 2A Evidence, Level II Recommendation)
In intrahepatic cholangiocarcinoma, 13%-20% of patients have FGFR2 fusion mutations, with Pemigatinib/Infigratinib/Futibatinib being three representative drugs targeting FGFR2 fusion mutations.
Interpretation 5: Addition of Pertuzumab + Trastuzumab Included in the Second-Line Treatment Regimen for HER2 Positive Advanced BTC (Class 2A Evidence, Level II Recommendation)
The MyPathway study enrolled 39 patients with HER2 positive cholangiocarcinoma, using Pertuzumab + Trastuzumab, with 9 out of 39 patients achieving disease remission. The ORR was 23%. Additionally, the HERB study is a phase II, single-arm multicenter study that enrolled patients with HER2 positive cholangiocarcinoma who failed Gemcitabine treatment, using Trastuzumab deruxtecan (T-DXd, DS-8201), with 8 out of 22 enrolled patients achieving disease remission, with an ORR of 36.4%, but 2 patients died due to severe lung injury.
Delivering the Strongest Voice of CSCOChinese Wisdom Changing Chinese Practice
In recent years, significant progress has been made in the basic and clinical research of cholangiocarcinoma, and the improvement of systemic anti-tumor regimens such as targeted therapy and immunotherapy has provided more treatment options for cholangiocarcinoma patients. With the advancement of clinical research in China, the updates to the guidelines are increasingly based on Chinese research and the disease characteristics of Chinese patients, and the CSCO guidelines truly reflect the strength of China in international clinical advances. It is hoped that with the emergence of new drugs and the development of clinical trials, higher quality evidence-based medical evidence can be provided to help Chinese cholangiocarcinoma patients achieve a better tomorrow!
References:
1. Wang Yingzhen, Zeng Yeting, Wang Xinrui, et al. Molecular Changes and Targeted Therapy of Intrahepatic and Extrahepatic Cholangiocarcinoma [J]. Clinical and Experimental Pathology Journal, 2022(038-001).
2. Guidelines Working Committee of the Chinese Society of Clinical Oncology. Chinese Society of Clinical Oncology (CSCO) Guidelines for Cholangiocarcinoma (2021) [M]. People’s Health Publishing House.
3. Andrew X. Zhu; Teresa Macarulla, MD; Milind M. Javle, MD, et al., Final Overall Survival Efficacy Results of Ivosidenib for Patients With Advanced Cholangiocarcinoma With IDH1, JAMA Oncology.
4. Prof Ghassan K Abou-Alfa, Teresa Macarulla, Prof Milind M Javle, et al., Ivosidenib in IDH1-mutant, chemotherapy-refractory cholangiocarcinoma (ClarIDHy): a multicenter, randomized, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2020 June; 21(6): 796–807.
Editor: Candy
Reviewer: Dayuan
Typesetter: Youshi
Execution: Youshi
This platform aims to convey more medical information to healthcare professionals. The content published on this platform cannot replace professional medical guidance in any way and should not be regarded as diagnostic or treatment advice. If such information is used for purposes other than understanding medical information, this platform does not bear related responsibilities. The platform does not endorse the descriptions and viewpoints of the published content. If there are copyright issues, please contact us, and we will handle them as soon as possible.
END
