
1. Introduction: Current Status and Clinical Issues in Heart Failure Device Therapy
At the joint forum channel of the 36th Great Wall Cardiology Conference and the Asian Cardiology Conference 2025, a high-level seminar focusing on innovations in heart failure (HF) device therapy (THT 2025 Highlights) gathered insights from top global experts. Professors Nir Uriel, Ulrich Jorde, and Sean Pinney from three major medical systems in New York, along with host Daniel Burkoff, systematically discussed the key challenges and technological breakthroughs in the field of heart failure treatment. As the end stage of various heart diseases, the management of heart failure is extremely complex. Despite significant advances in pharmacological treatment, many patients continue to progress, ultimately facing three typical clinical dilemmas:
-
Firstly, irreversible enlargement and remodeling of the cardiac structure lead to persistent functional deterioration;
-
Secondly, the condition progresses to end-stage, where medical treatment is ineffective, necessitating heart transplantation or long-term mechanical support;
-
Thirdly, patients may experience acute decompensation, resulting in cardiogenic shock, which poses a serious threat to life.
The content of this forum precisely addressed these three challenges, providing in-depth discussions on percutaneous left ventricular reconstruction, durable left ventricular assist devices (LVADs), and temporary mechanical circulatory support (tMCS) for acute heart failure.
2. Durable Left Ventricular Assist Devices (LVAD): Five-Year Results and Clinical Updates from the MOMENTUM 3 Study
Life support for patients with end-stage heart failure has long relied on heart transplantation, but the reality of donor shortages has spurred the development of LVAD technology. Professor Nir Uriel from Columbia University in New York reviewed the evolution of LVADs from early large devices simulating cardiac pulsation to smaller, less complicated axial flow pumps, culminating in the current mainstream choice, the fully magnetically levitated centrifugal pump—HeartMate 3.
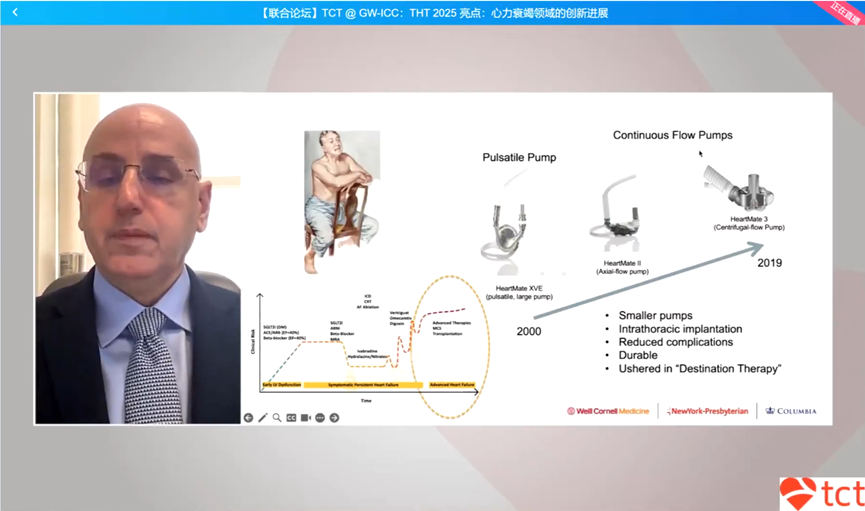
Figure 1: Evolution of LVAD Technology
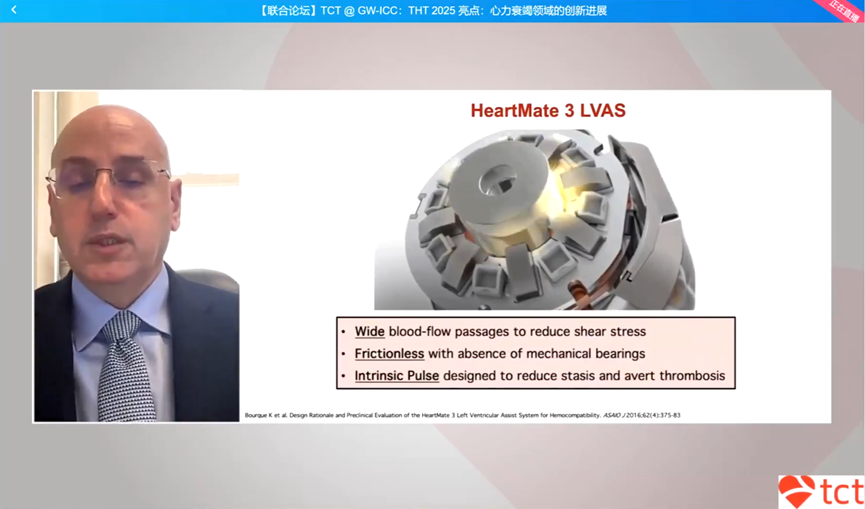
Figure 2: Technical Principle of HeartMate 3 Magnetic Levitation Pump
This device is currently the only durable LVAD product approved by the FDA in the United States, with its core technological advantage being the use of a fully magnetically levitated rotor, eliminating mechanical bearings, combined with a wide blood flow channel and built-in pulse function, aimed at minimizing blood cell damage and thrombus formation.
The MOMENTUM 3 study is a landmark trial validating the performance of HeartMate 3. Five-year follow-up data from this study showed that the total survival rate for patients in the HeartMate 3 group reached 58.4%. More critically, the composite endpoint—survival without disabling stroke or the need for device replacement—was achieved in 54.0% of the HeartMate 3 group, significantly better than the 29.7% of the previous generation axial flow pump, HeartMate II. This study confirms the reliability and safety of the new generation LVAD in long-term applications.
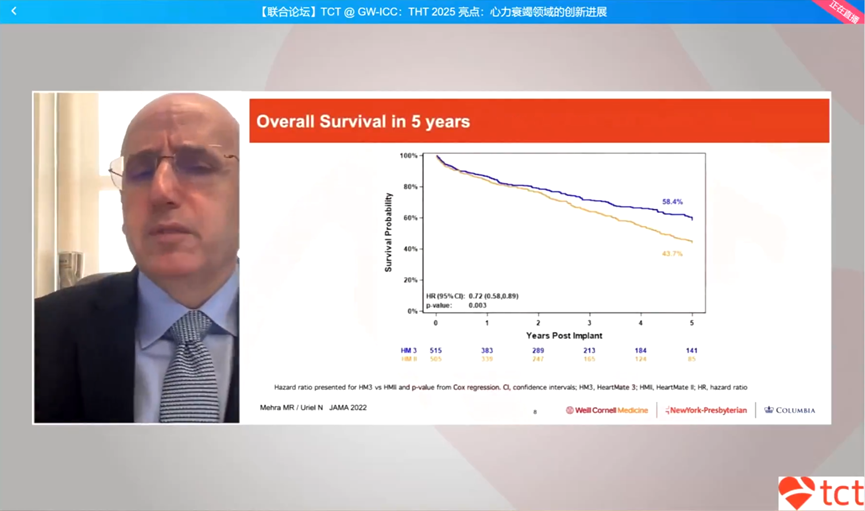
Figure 3: Five-Year Total Survival Rate Curve from the MOMENTUM 3 Study
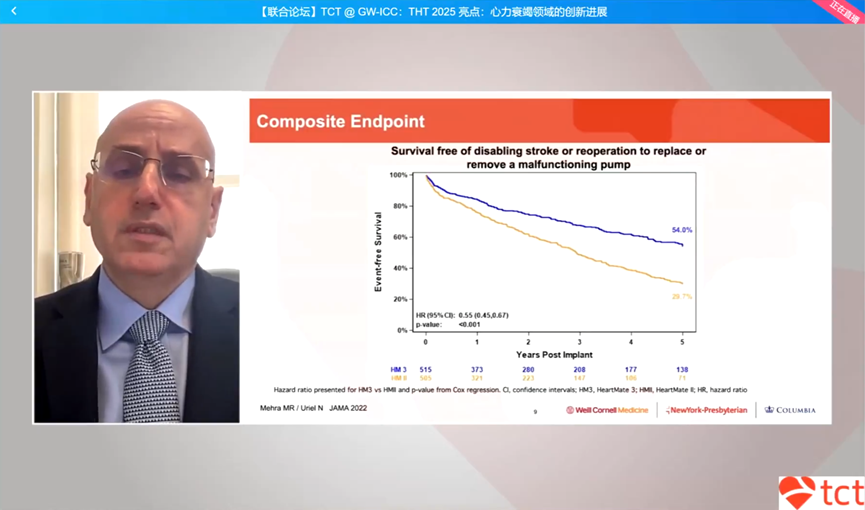
Figure 4: Five-Year Composite Endpoint Survival Curve
Despite significant progress, LVAD implantation still faces challenges with adverse events. Data shows that gastrointestinal bleeding and driveline infections are issues that require attention. To address the high bleeding risk, a randomized controlled study named ARIES explored the possibility of optimizing antithrombotic strategies. This study randomized patients into a placebo group and an aspirin group, with results showing that patients who discontinued aspirin had significantly reduced non-surgical related bleeding events. A subgroup analysis of this study further found that for high-risk patients with a history of atherosclerotic cardiovascular disease, discontinuing aspirin was also safe, and these patients benefited the most from the reduced bleeding risk.
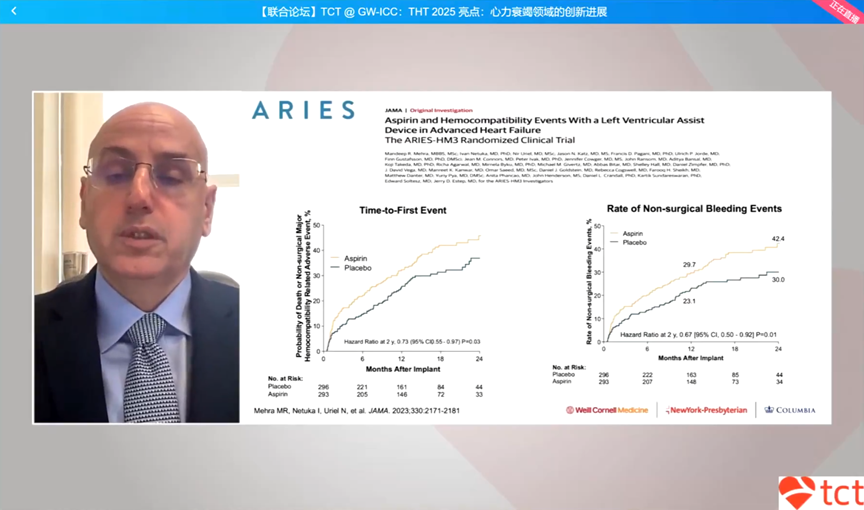
Figure 5: Primary Endpoint of the ARIES Study (First Non-Surgical Bleeding Event)
With the improvement in LVAD performance, an important clinical question arises: how to choose between LVAD and heart transplantation for suitable patients?
Professor Uriel’s team compared data from younger patients in the MOMENTUM 3 study with concurrent heart transplantation data from the United Network for Organ Sharing (UNOS). The results showed that after propensity score matching, the two groups’ two-year survival rate curves nearly overlapped.
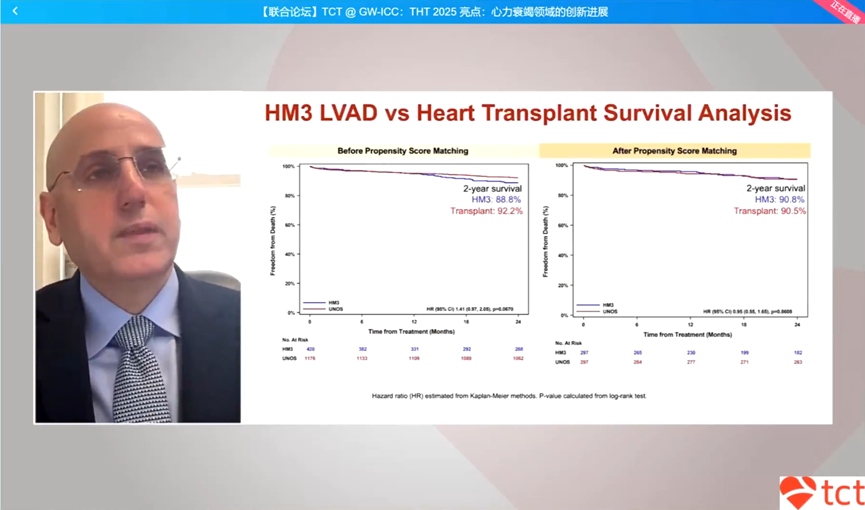
Figure 6: Comparison of Two-Year Survival Rates between HM3 LVAD and Heart Transplantation
If the waiting time for transplantation is also considered, starting from the time patients enter the transplant waiting list, the survival benefit of the LVAD group becomes even more apparent.
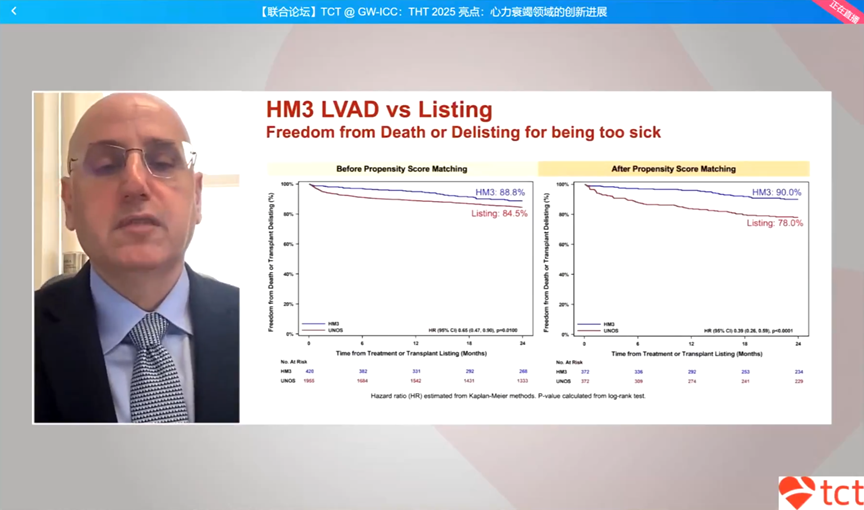
Figure 7: Comparison of Two-Year Survival Rates between HM3 LVAD and Transplant Waiting List
In terms of adverse events, LVAD patients have a lower risk of severe renal failure and infections compared to transplant patients, but the risk of disabling stroke is relatively higher. For some younger patients with end-stage heart failure, the strategy of initially implanting an LVAD to extend life warrants further investigation.
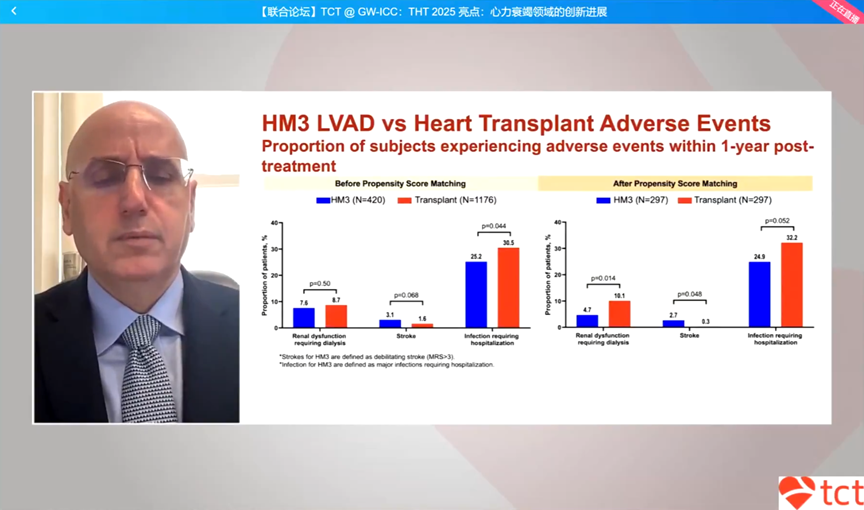
Figure 8: Bar Chart Comparison of Adverse Events One Year Post Heart Transplantation
3. Percutaneous Left Ventricular Reconstruction: Improving Heart Failure Prognosis through Physical Reversal of Remodeling
Before patients progress to needing an LVAD or transplantation, there exists a critical intermediate stage. For those who continue to experience symptoms despite receiving optimal medical therapy, how to delay or even reverse disease progression is a significant gap in current heart failure treatment. Professor Ulrich Jorde from the Montefiore Einstein Medical System introduced the innovative therapy of percutaneous left ventricular reconstruction, aimed at filling this gap. The theoretical basis of this therapy stems from the Law of Laplace, which states that the enlargement of the ventricular cavity (increased radius) leads to increased wall tension, creating a vicious cycle of increased energy expenditure and further deterioration of heart function.
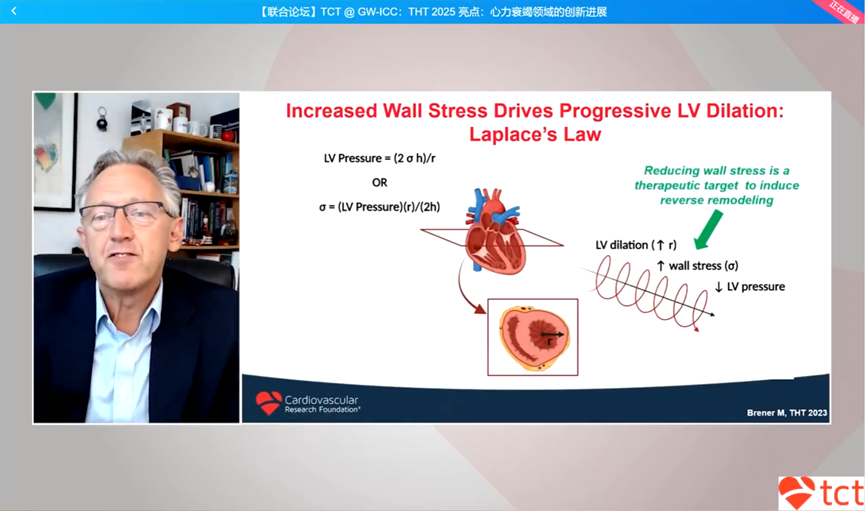
Figure 9: Illustration of the Law of Laplace and the Vicious Cycle of Ventricular Remodeling
Therefore, by physically reducing the left ventricle and lowering wall tension, it can not only immediately improve cardiac mechanics but may also initiate a biological remodeling process.
The AccuCinch system is designed based on this concept as a transcatheter minimally invasive device. The procedure involves implanting a ring of anchors along the base of the left ventricular inner wall via the femoral artery, and then tightening the connecting cords to “pull tight” the ventricular wall, thereby achieving ventricular reduction and morphological remodeling.

Figure 10: Illustration of the AccuCinch System Transcatheter Implantation Process
Early clinical studies have demonstrated the safety and efficacy of this technology. In 51 heart failure patients, the incidence of serious adverse events was low. Moreover, post-operative patients showed sustained improvements in cardiac structure and function. Data indicated that during the two-year follow-up period, the average left ventricular end-systolic volume (LVESV) decreased by approximately 30 milliliters, while the left ventricular ejection fraction (LVEF) increased by about 5%.
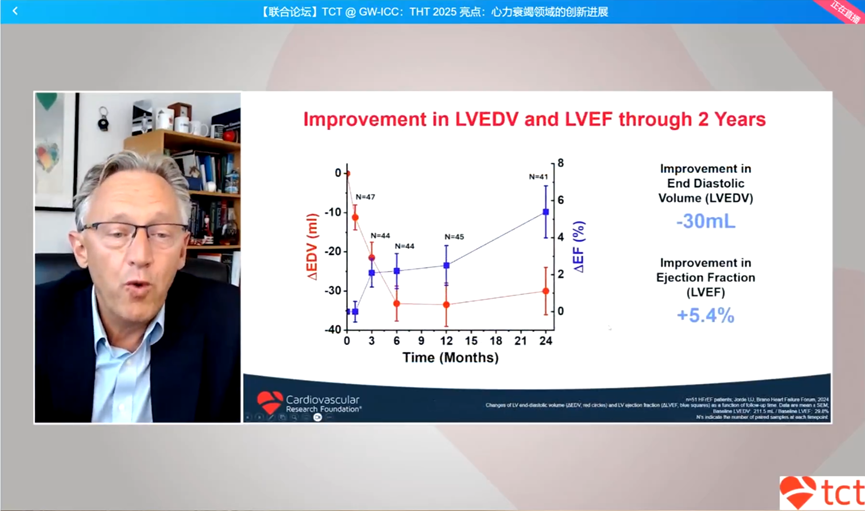
Figure 11: Trends in LVEDV and LVEF Changes Two Years Post AccuCinch
This improvement in structure and function translates into a tangible enhancement in patients’ quality of life, reflected in significant improvements in Kansas City Cardiomyopathy Questionnaire (KCCQ) scores, New York Heart Association (NYHA) functional classification, and six-minute walk distance.
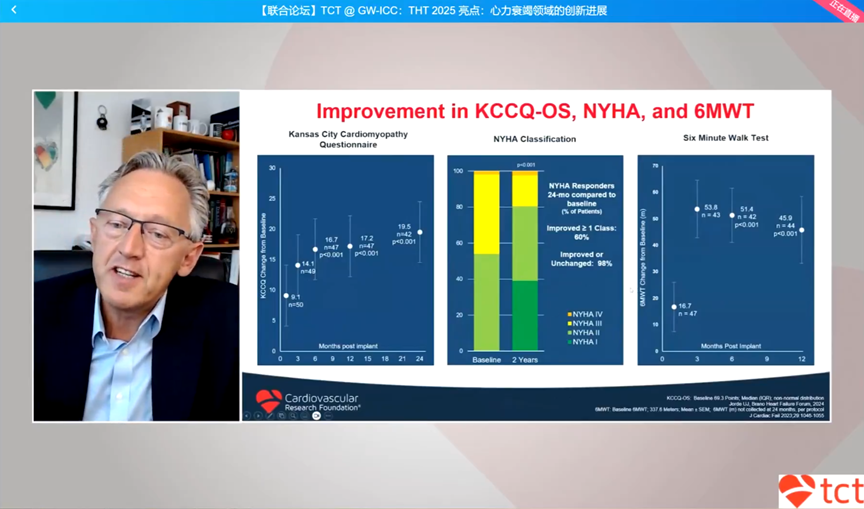
Figure 12: Improvements in KCCQ, NYHA Classification, and Six-Minute Walk Test
To further validate the effectiveness of this therapy, a large international multicenter randomized controlled study named CORCINCH-HF is underway. This study aims to clarify whether AccuCinch combined with drug therapy is superior to drug therapy alone for mid-to-late stage heart failure patients with reduced ejection fraction, left ventricular enlargement, but without severe mitral regurgitation, who still have symptoms under standard drug treatment. The success of this study could provide a new effective treatment option for this type of patient while preserving their “native heart”.
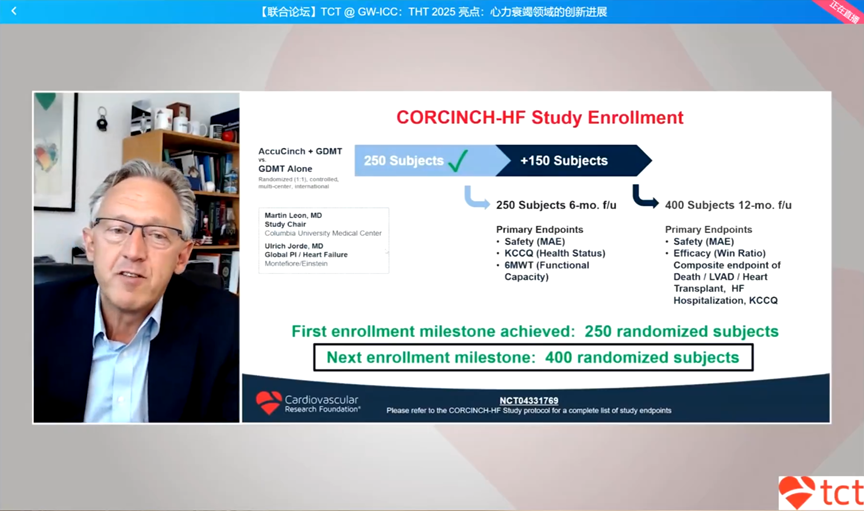
Figure 13: Design of the CORCINCH-HF Study
4. Temporary Mechanical Circulatory Support (tMCS) for Acute Decompensated Heart Failure: Device Selection and Clinical Decision-Making
Acute decompensated heart failure is the most common reason for hospitalization among heart failure patients, with the most critical manifestation being cardiogenic shock. Professor Sean Pinney from Mount Sinai Health System pointed out that cardiogenic shock due to heart failure exacerbation (HF-CS) differs significantly in pathophysiology and patient characteristics from cardiogenic shock caused by acute myocardial infarction (AMI-CS). Patients with HF-CS typically experience long-term negative remodeling, poor ventricular compliance, and higher filling pressures; while they may respond to tMCS, they often ultimately require escalation to LVAD or heart transplantation as definitive treatment.
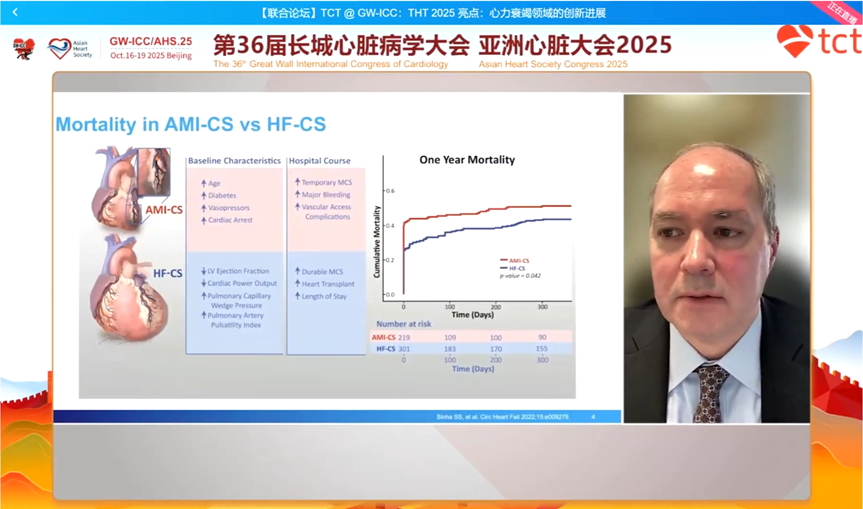
Figure 14: Comparison of One-Year Cumulative Mortality Rates between AMI-CS and HF-CS Patients
In the face of the critical condition of HF-CS, precise decision-making is crucial. Clinically, the shock classification system from the Society for Cardiovascular Angiography and Interventions (SCAI) is widely used to dynamically assess shock from Class B (beginning) to Class E (near death). This classification system helps clinicians determine the timing of intervention and select the most appropriate tMCS device based on the patient’s ventricular involvement (left heart, right heart, or biventricular failure), oxygenation status, and prognostic goals.
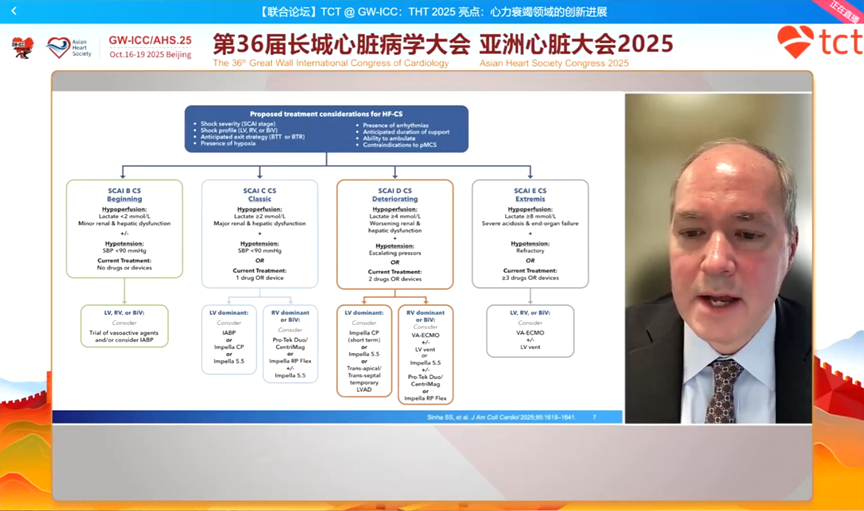
Figure 15: Treatment Considerations for HF-CS (Based on SCAI Classification)
tMCS mainly includes three types of devices:
-
Intra-aortic balloon pump (IABP), which increases coronary perfusion during diastole by expanding the balloon and reduces afterload during systole by collapsing the balloon, can increase cardiac output by approximately 0.5 L/min;
-
Micro-axial flow pump (Impella), which is inserted into the left ventricle via the peripheral artery, directly pumps blood from the left ventricle into the aorta, providing stronger blood flow support and effectively “decompressing” the left ventricle;
-
andVeno-arterial extracorporeal membrane oxygenation (VA-ECMO), which not only provides circulatory support but also gas exchange function, suitable for patients with biventricular failure combined with respiratory failure.
Despite the widespread clinical application of tMCS, high-level evidence remains relatively scarce. The recently published ALTSHOCK-2 study is a randomized controlled trial targeting HF-CS patients, comparing the efficacy of IABP with standard medical therapy, with results showing no significant difference in 60-day survival rates between the two groups. However, this study had a high crossover rate, with some patients in the standard treatment group ultimately receiving IABP or other support devices due to worsening conditions. This reflects the inherent difficulties of conducting strict randomized controlled trials in critically ill shock patients. Therefore, current clinical practice relies more on comprehensive assessments by multidisciplinary teams, making individualized device selection and management based on patients’ hemodynamic data and clinical trajectories.
5. Expert Discussion: Future Directions in Heart Failure Device Therapy

Figure 16: Expert Discussion Session
During the discussion session, the three experts reached a consensus on the future of heart failure device therapy. For durable LVADs, the core breakthrough in the future lies in achieving “fully implantable” devices, completely eliminating external driveline through transcutaneous energy transfer technology, which will fundamentally address the long-standing issue of infection that troubles patients. At the same time, smart technology is another important direction, developing “smart pumps” that can automatically adjust speed based on patients’ activity levels, further improving patients’ exercise tolerance and quality of life.
For left ventricular reconstruction technology, experts unanimously believe it precisely fills the significant gap between drug therapy and end-stage treatment. It provides an effective means for those who have not yet reached the critical stage requiring LVAD but whose quality of life has been severely compromised, allowing them to retain their native heart and delay disease progression.
Finally, regarding the lack of evidence for cardiogenic shock treatment, experts suggested a need to shift the thinking in clinical research. Given the challenges of implementing traditional randomized controlled trials in the shock domain, future studies may need to explore using high-quality real-world registry data for propensity score matching and other methods, comparing with randomized trial data, thereby providing timely and feasible evidence support for clinical decision-making while ensuring scientific rigor.
6. Conclusion: Device Therapy Propels Heart Failure Management into a New Era of Individualization
This report systematically showcases the latest advancements in the field of heart failure device therapy, covering the entire chain from delaying the progression of mid-stage heart failure, supporting long-term survival of end-stage patients, to rescuing acute cardiogenic shock. Whether through physical reversal of remodeling to repair the heart or through mechanical assistance to replace heart function, these innovative technologies profoundly change the treatment paradigm for heart failure. In the future, as technology continues to mature and clinical evidence accumulates, heart failure treatment will no longer be a “one-size-fits-all” approach, but rather a personalized treatment strategy collaboratively developed by multidisciplinary teams based on precise assessments of patients’ disease stages, hemodynamic characteristics, and individual needs, with the ultimate goal of maximizing patient survival and improving their quality of life.
GW-ICC/AHS 2025
Clickto read the original article for the latest updates