
 Xiao-Jun Zhao Associate Professor
Xiao-Jun Zhao Associate Professor
Department of Urology, First Affiliated Hospital of Soochow University, Chief Physician, Doctor of Medicine, Master’s Supervisor.
Young Committee Member of the Urology Society of Suzhou Medical Association,Executive Committee Member of the Suzhou Society of Integrated Traditional Chinese and Western Medicine in Urology,Member of the Minimally Invasive Treatment Professional Committee of the Chinese Anti-Cancer Association,Member of the Chinese Anti-Cancer Association,Member of the Andrology Branch of Jiangsu Medical Association,Member of the Minimally Invasive Group of the Urology Branch of Jiangsu Medical Association,Member of the Kidney Cancer Collaborative Group of Jiangsu Anti-Cancer Association.
Participated in multiple projects of the National Natural Science Foundation, hosted one provincial-level project, two municipal-level projects, one project of the Jiangsu Provincial Key Laboratory of Immunology, one project of the National Key Laboratory of Functional Organic Molecular Chemistry, and two projects of Soochow University.
Specializes in comprehensive diagnosis and treatment of urological tumors, minimally invasive Da Vinci surgery, and full-process management.
Case Introduction
Patient: Male, 67 years old.
Chief Complaint: Intermittent painless gross hematuria for over a week.
Present Illness: Intermittent painless gross hematuria appeared over a week ago without obvious inducement, with urine color resembling wash meat water, accompanied by urinary frequency, urgency, dysuria, and occasional left flank pain.
Past Medical History: History of hypertension.
Physical Examination: No swelling in both renal areas, no tenderness or percussion pain in both renal areas. No tenderness in the ureteral pathway. Bladder not full, no tenderness in the suprapubic area, external genitalia developed normally.
Auxiliary Examinations
Urinalysis: Urine occult blood (2+), white blood cells 40.55 cells/ul.
Biochemistry: Albumin 36.1g/L, high-sensitivity C-reactive protein 9.33mg/L, cystatin C 1.238mg/L.
Blood Routine: Hemoglobin 122g/L.
Enhanced CT (2024-08-12, our hospital): Thickening of the wall at the left ureter-bladder junction and bladder trigone, highly suggestive of K, recommended cystoscopy for further examination; slight tortuosity of the upper segment of the left ureter; hydronephrosis with dilation of the left renal pelvis and ureter, slightly reduced perfusion of the left kidney; prostatic hyperplasia.
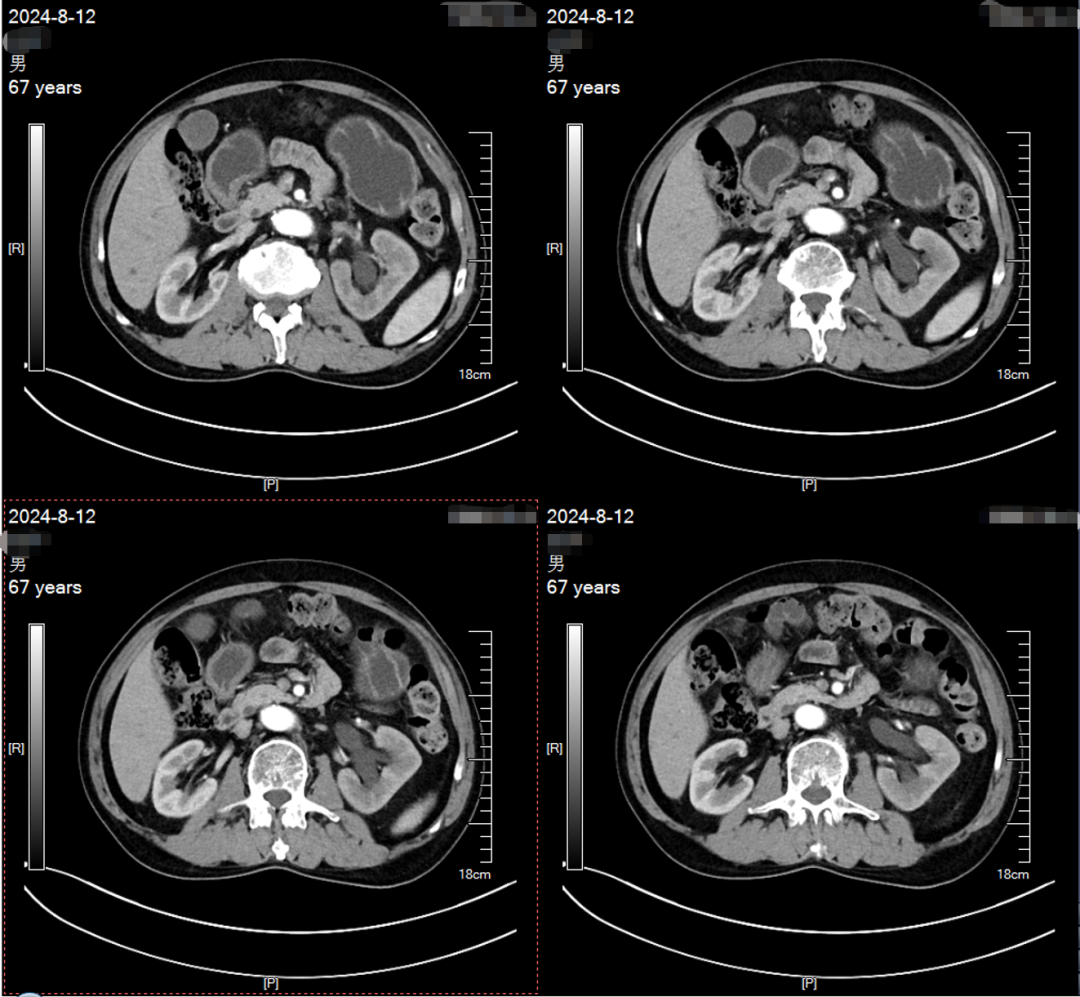
Hydronephrosis of the left renal pelvis and ureter
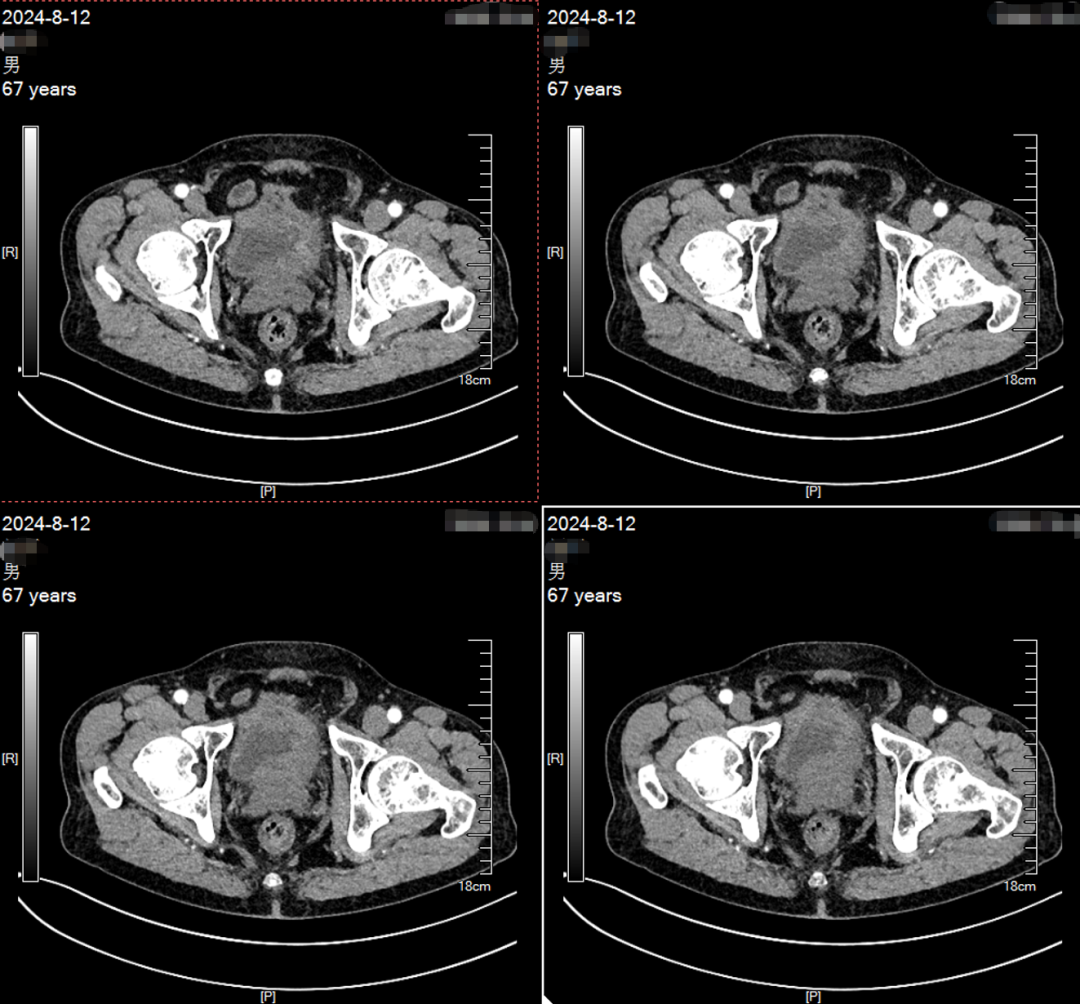
Thickening of the wall at the left ureter-bladder junction and bladder trigone
Treatment Process
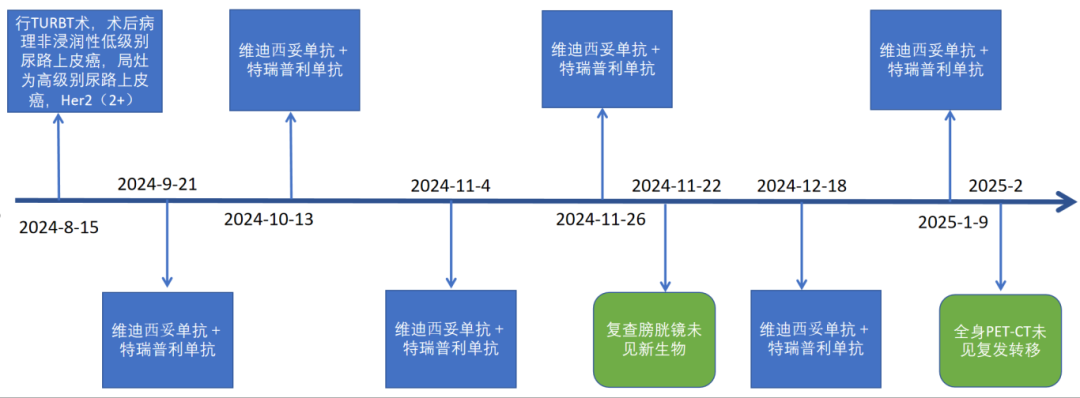
On 2024-08-15, the patient underwent the first TURBT at our hospital: During the operation, a large cauliflower-like tumor was observed extending from approximately the 5 o’clock position of the left bladder neck to the left bladder wall, measuring about 6cm*5.5cm, easily bleeding upon touch. Additionally, the posterior wall and the area around the left ureteral orifice were affected by the tumor, and there were scattered small cauliflower-like tumors around the right ureteral orifice, approximately 2mm in size.

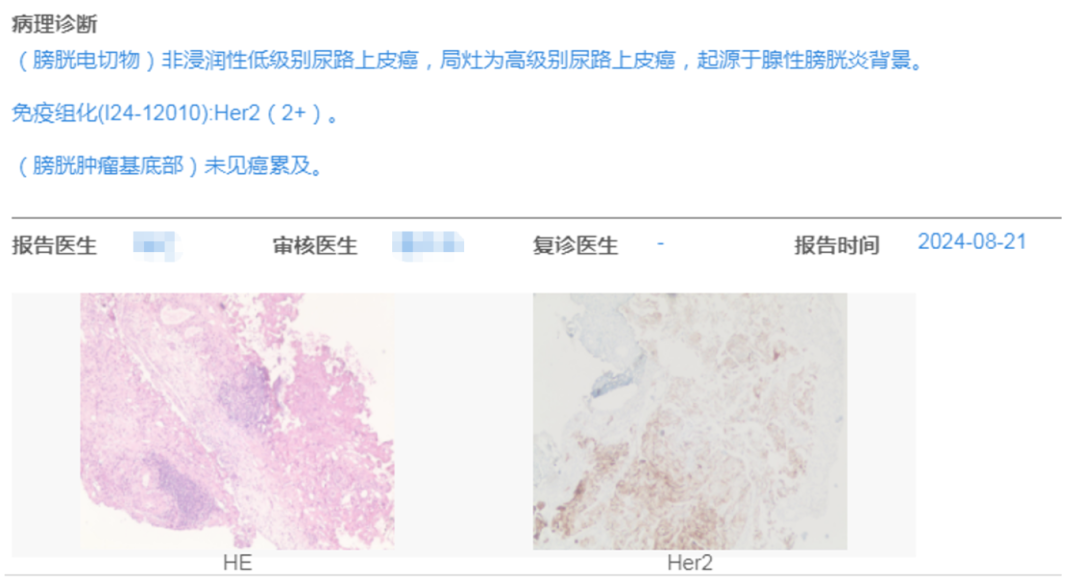
Postoperative pathology: Non-invasive low-grade urothelial carcinoma, with focal high-grade urothelial carcinoma.
Immunohistochemistry: Her2 (2+).
Diagnosis: Bladder tumor, tumor in the lower segment of the left ureter, T1bN0M0, G3-4, high risk.
On 2024-08-29, the patient underwent the first GC regimen chemotherapy, experiencing severe adverse reactions such as nausea and vomiting. Subsequently, treatment was changed to Vadastuximab + Toripalimab.
Vadastuximab + Toripalimab Treatment
Time Period: From 2024-09-21 to January 2025;
Dose: Vadastuximab 120mg/each + Toripalimab 240mg/each;
Regimen: Once every 3 weeks (2024-09-21, 2024-10-13, 2024-11-04, 2024-11-26, 2024-12-18, 2025-01-09);
Side Effects: Mild nausea and vomiting.
Subsequently, close follow-up + bladder instillation continues to this day.
On 2024-11-20 (3 months post-surgery), re-examination CT: After TURBT at the left ureter-bladder junction, thickening of the lower segment of the left ureter.
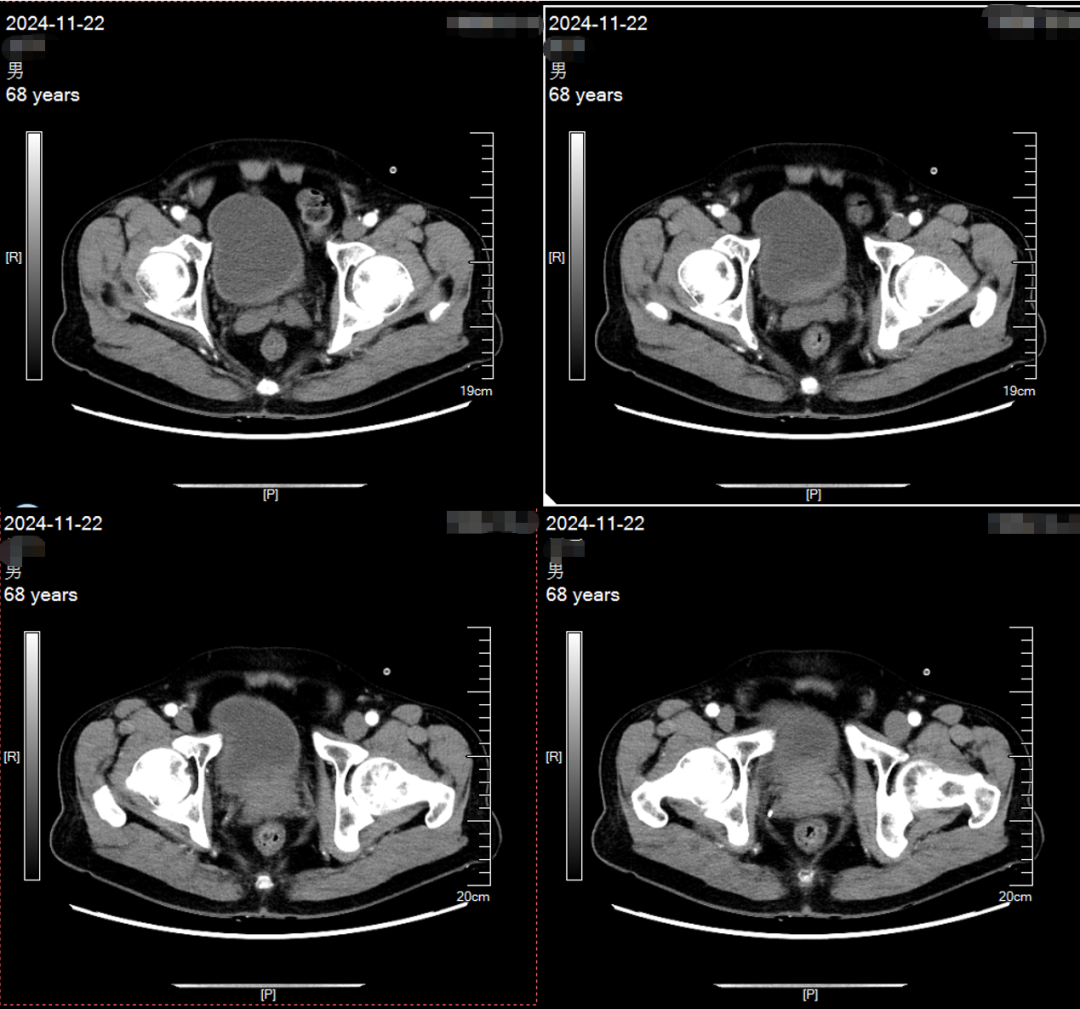
On 2024-11-22 (3 months post-surgery), re-examination cystoscopy: No new tumors seen in the bladder, with scarring visible in the trigone area and around the left ureteral orifice from previous electrosurgery. No significant new tumors found in the lumen during left ureteroscopy. Multiple TURBT biopsies were taken, pathology report available.
3 months post-surgery, CR, pathological PCR status, continued maintenance treatment regimen for a total of 6 times..
In February 2025, Vadastuximab 120mg + Toripalimab 240mg after 6 cycles, re-examination PET-CT at 6 months post-surgery.6 months post-surgery, CR..
Treatment Process
Conclusion
Patients in the high-risk group of non-muscle invasive bladder cancer (NMIBC) and extremely high-risk subgroup are generally recommended to undergo radical cystectomy (RC) or transurethral resection of bladder tumor (TURBT) + postoperative adjuvant Bacillus Calmette-Guérin (BCG) bladder instillation immunotherapy due to the characteristics of tumor recurrence and progression.
For upper urinary tract urothelial carcinoma, guidelines generally recommend radical partial ureterectomy.
Due to the significant surgical trauma, high postoperative and long-term complications, renal insufficiency after surgery, and significant reduction in quality of life for patients after ureter diversion, some patients refuse or are unsuitable for radical surgery.
Therefore, choosing a safe and effective organ-preserving treatment strategy is extremely important.
This case of a high-risk NMIBC patient, who also had upper urinary tract urothelial carcinoma on the same side, achieved PCR after 3 months of comprehensive treatment mainly consisting of TURBT + DV. This effectively controlled the tumor and successfully preserved functional organs, greatly improving the patient’s quality of life.
The treatment regimen of ADC drugs + TURBT + bladder instillation shows significant efficacy in treating high-risk NMIBC and is one of the options for comprehensive bladder preservation.
The comprehensive treatment centered on Vadastuximab shows significant efficacy in treating upper urinary tract urothelial carcinoma and is one of the options for comprehensive organ preservation.
ADC drugs (Vadastuximab) have good safety, and patients have good clinical tolerance.
Statement:This content is intended for medical and pharmaceutical professionals only and does not constitute actual treatment advice. For reprints, please contact for authorization; infringement will be pursued!
Editor: Wu Mengxia
Reviewed by:Huang Pengcheng