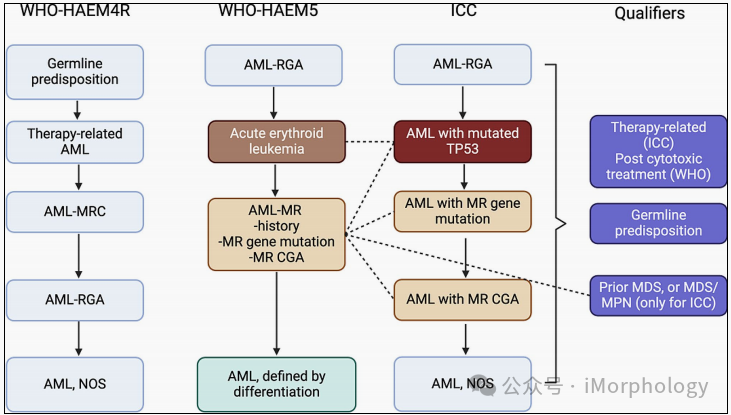
Image Source: Xiao W, Nardi V, Stein E, Hasserjian RP. A practical approach on the classifications of myeloid neoplasms and acute leukemia: WHO and ICC. J Hematol Oncol. 2024;17(1):56. Published 2024 Jul 29.
For TP53 positive MDS, MDS/AML, and AML, the requirements for TP53 mutations differ, leading to the discrepancies in classifications of TP53 positive MDS, MDS/AML, and AML by WHO and ICC.
Firstly: WHO requires that both types of MDS (including low blast count and high blast count) have double mutations; whereas ICC only requires double mutations for MDS (low blast count, with 5-9% bone marrow blasts/2-9% peripheral blood) type, while MDS/AML (with 10-19% bone marrow blasts and 10-19% peripheral blood) and AML only require a mutation.
Secondly: WHO does not set a requirement for the allele variant frequency (VAF) of TP53 mutations; while ICC requires VAF ≥ 10%.
Thirdly: WHO defines TP53 double mutations as ① TP53 double mutations, ② or single mutations + evidence of copy neutral loss of heterozygosity (CN-LOH); while ICC defines it as ① double mutations (each VAF ≥ 10%), ② or single TP53 mutation with del (17p), VAF>50%, 17p TP53 locus CN-LOH analysis, ③ or complex karyotype (if there is no TP53 gene locus LOH information).
Fourthly: Due to the above situations, WHO in the classification of MDS diagnoses, as long as there is evidence of TP53 double mutations (requirements as mentioned above), there is a diagnosis of bi-TP53 MDS (i.e., all MDS subtypes, including low blast count MDS, with bone marrow blasts 5-9%/ peripheral blood 2-4%, and bone marrow 10-19%/ peripheral blood 5-19%/ containing Auer bodies); ICC in the classification of MDS diagnoses, for MDS with bone marrow blasts less than 10%, or low blast count MDS with double mutations (requirements as mentioned above) can be diagnosed, while the type with bone marrow blasts 10-19% does not require TP53 double mutations and is diagnosed as TP53 mutated MDS/AML.
Fifthly: For AML (with blasts ≥ 20%), there is no type of TP53 positive AML in WHO, so where does TP53 positive AML generally fall in WHO? As there is no subtype, many TP53 positive AML are classified as ① acute erythroid leukemia (AEL): TP53 mutations can occur, but are not a necessary criterion; or classified as ② AML-MR (complex karyotype, due to unbalanced translocations leading to 5q/7q/17p deletions or monosomy of 7), but if the morphological criteria meet AEL, it is prioritized to be diagnosed as AEL. In ICC, this type exists (no need for TP53 double mutations, but VAF still ≥ 10%). If any somatic TP53 mutation is detected (VAF ≥ 10%), AML-MRC will be replaced by TP53–AML.
In the early 20th century, MDS was first described as “refractory anemia/leukemia precursor”. In 1976, FAB named it “myelodysplastic syndromes”, including RAEB and CMML. In 1982, it was revised to “myelodysplastic syndromes”, including five entities: RA, RARS, RAEB, RAEB-t, and CMML. This classification was widely used by clinicians and pathologists for nearly 20 years, and while it had some prognostic value, there was significant variability in prognosis among patients of each type. Based on FAB, the 2001 WHO system emerged, which distinguished between single/multiple lineage dysplasia; increased blast counts were divided into two categories; and the 5q- subtype was first proposed. CMML was included in MDS/MPN; RAEB-t was also classified as AML (with blast proportions 20%). In 2008, WHO added provisional types of childhood MDS and MDS-U, and proposed other blood cell reductions besides anemia (“refractory cytopenia” rather than “refractory anemia”). In 2017, WHO released an extensive classification system, removing reductions in cells, anemia, neutrophils, and platelets, instead using “single or multiple lineage dysplasia”. Another major change was the dominance of erythroid lineage (erythroid > 50%) and blast counts ≥20% (NEC) cases, previously diagnosed as erythroleukemia, were reclassified as MDS after ANC count. In 2022, WHO further increased genetic definitions of MDS, including 5q-, TP53, SF3B1 mutations; and morphological definitions of MDS, no longer subdividing into single/multiple lineage dysplasia. Perhaps in the future, genetic definitions will be adopted for MDS classification, while the types defined morphologically will gradually decrease.
Previous Review
2024 SUMMARY
09
Is there a connection between tea and leukemia? Latest research: tea can not only fight cancer, but drinking three cups a day can also combat aging!
White blood cell count over 100,000! What are the key management principles for leukocytosis!
Don’t supplement vitamins blindly! JCI latest: supplementation of “antioxidant” vitamins C and E may increase tumor progression and metastasis.
Tyrosine Kinase Inhibitors Summary丨What are the differences between BCR-ABL VS BTK in treating malignant hematological tumors?
Star Mark 🌟“Meis Hematology New Frontiers”🌟Receive timely updates on every freshly published article!