ADC, or antibody-drug conjugates, is a term that everyone is likely familiar with. The design concept of ADC originated from Paul Ehrlich’s idea of “magic bullets,” aimed at achieving precise targeted therapy while minimizing damage to normal tissues. As of now, there are 15 ADC drugs approved for market worldwide, with over 400 ADC candidates in the research and development stage, of which 24 have entered Phase III clinical trials.Behind the vigorous development of ADC, I am more interested in understanding how it has evolved to this extent over time, and what problems each generation of evolution has addressed. Reviewing the past helps us understand the new!Table 1 Approved ADC Drugs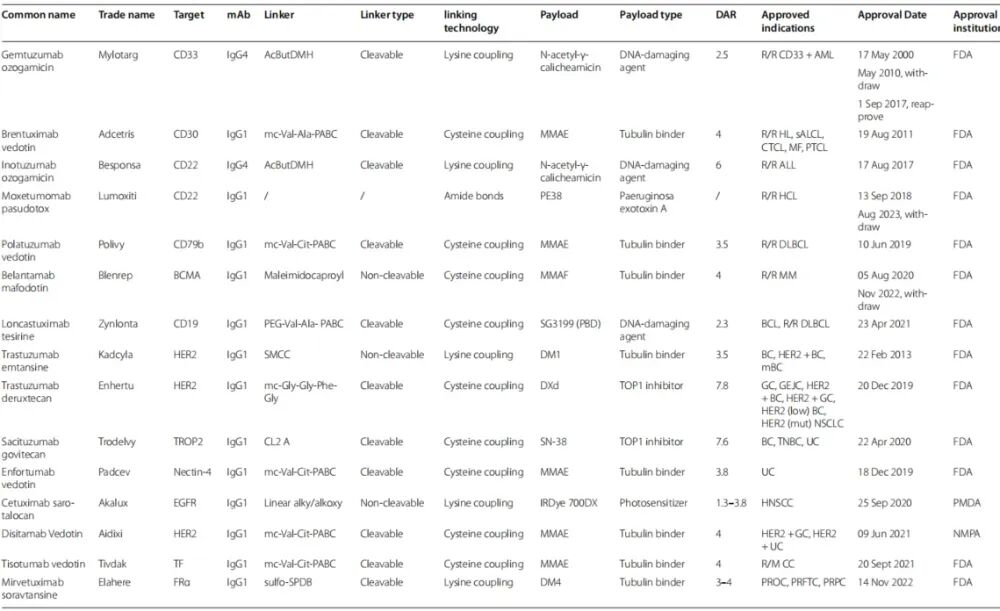 The development history of ADC can be summarized into four stages:First GenerationADC used murine antibodies, non-cleavable linkers, and traditional chemotherapy drugs as payloads.Representative drug: Gemtuzumab ozogamicin (targeting CD33).Problems: High immunogenicity, unstable linkers, and premature release of payloads leading to severe toxicity.Second GenerationADC used humanized antibodies, more stable linkers, and more potent payloads (e.g., MMAE).Representative drugs: Brentuximab vedotin (targeting CD30), Trastuzumab emtansine (T-DM1, targeting HER2).Improvements: Reduced immunogenicity and enhanced efficacy, but still faced issues of heterogeneity and off-target toxicity.Third GenerationADC used fully human antibodies, site-specific conjugation technology, and more uniform DAR (2 or 4).Representative drug: Enfortumab vedotin (targeting Nectin-4).Features: Enhanced hydrophilicity of linkers, reduced aggregation, and improved circulation stability.Fourth GenerationADC has a higher DAR (e.g., 7.8), stronger payloads, and smarter linkers.Representative drugs: Trastuzumab deruxtecan (DS-8201), Sacituzumab govitecan.Breakthrough: Significantly increased intratumoral drug concentration, enhancing the “bystander effect”.
The development history of ADC can be summarized into four stages:First GenerationADC used murine antibodies, non-cleavable linkers, and traditional chemotherapy drugs as payloads.Representative drug: Gemtuzumab ozogamicin (targeting CD33).Problems: High immunogenicity, unstable linkers, and premature release of payloads leading to severe toxicity.Second GenerationADC used humanized antibodies, more stable linkers, and more potent payloads (e.g., MMAE).Representative drugs: Brentuximab vedotin (targeting CD30), Trastuzumab emtansine (T-DM1, targeting HER2).Improvements: Reduced immunogenicity and enhanced efficacy, but still faced issues of heterogeneity and off-target toxicity.Third GenerationADC used fully human antibodies, site-specific conjugation technology, and more uniform DAR (2 or 4).Representative drug: Enfortumab vedotin (targeting Nectin-4).Features: Enhanced hydrophilicity of linkers, reduced aggregation, and improved circulation stability.Fourth GenerationADC has a higher DAR (e.g., 7.8), stronger payloads, and smarter linkers.Representative drugs: Trastuzumab deruxtecan (DS-8201), Sacituzumab govitecan.Breakthrough: Significantly increased intratumoral drug concentration, enhancing the “bystander effect”.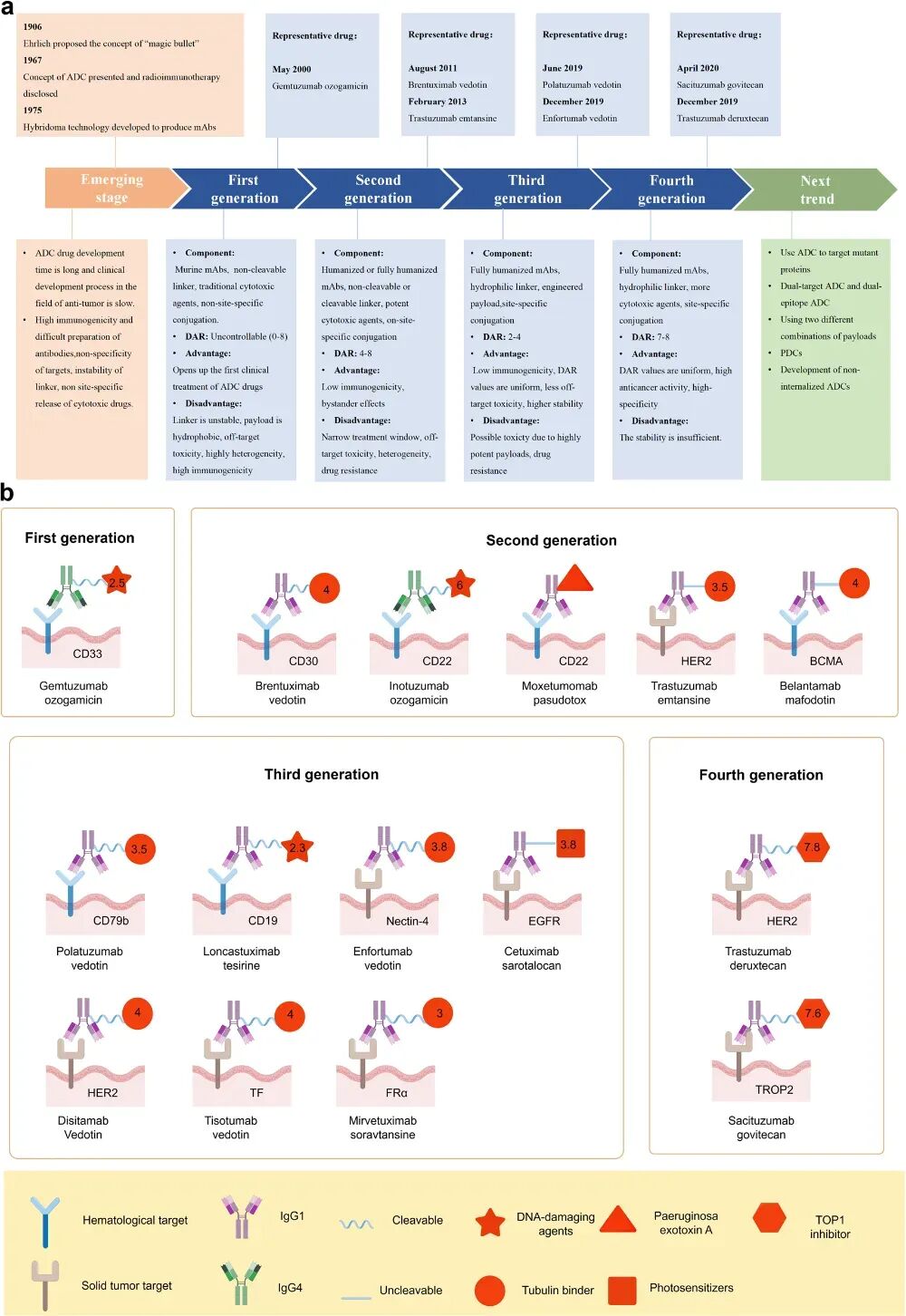 Figure 1 Development History of ADCMechanism of Action of ADCADC exerts its antitumor effects through the following mechanisms:Binding and internalization: ADC binds to tumor cell surface antigens and enters the cell via endocytosis.Lysosomal degradation: In the lysosome, the linker is cleaved by enzymes or acidic environments, releasing the payload.Cell killing: The payload interferes with DNA replication or microtubule function, inducing apoptosis.Bystander effect: Some payloads can penetrate cell membranes and kill adjacent antigen-negative or drug-resistant cells.Immune effects: The antibody portion can mediate ADCC, ADCP, CDC, and other immune killing mechanisms.
Figure 1 Development History of ADCMechanism of Action of ADCADC exerts its antitumor effects through the following mechanisms:Binding and internalization: ADC binds to tumor cell surface antigens and enters the cell via endocytosis.Lysosomal degradation: In the lysosome, the linker is cleaved by enzymes or acidic environments, releasing the payload.Cell killing: The payload interferes with DNA replication or microtubule function, inducing apoptosis.Bystander effect: Some payloads can penetrate cell membranes and kill adjacent antigen-negative or drug-resistant cells.Immune effects: The antibody portion can mediate ADCC, ADCP, CDC, and other immune killing mechanisms.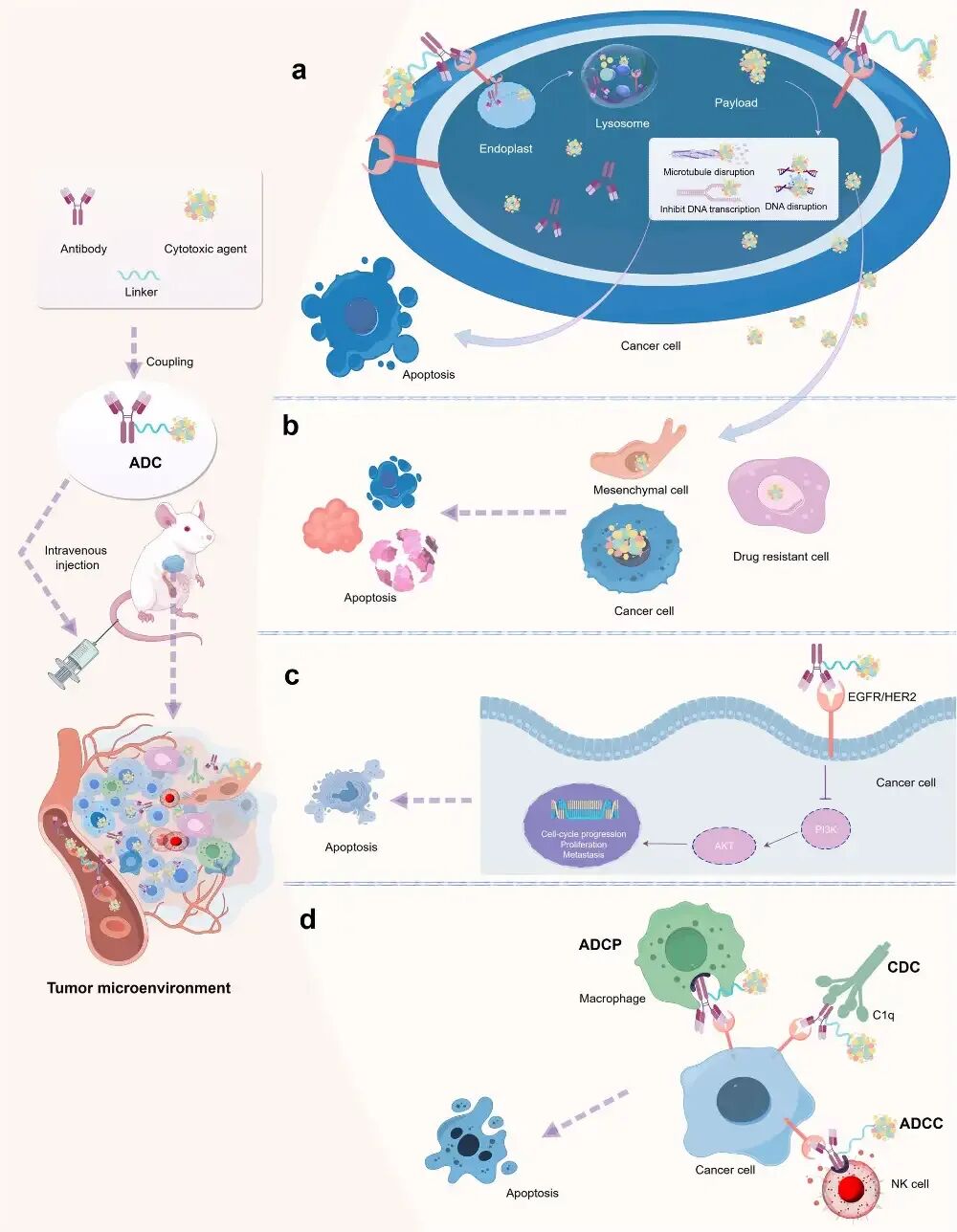 Figure 2 Mechanism of Action of ADCCore Components of ADCAntibody: An ideal antibody should have high specificity, low immunogenicity, long half-life, and ease of internalization.IgG1 is the most commonly used subtype (86.7%) due to its long half-life and strong immune effects.Bispecific antibodies (BsAbs) are the future trend, capable of targeting two antigens or epitopes simultaneously, enhancing specificity (e.g., ZW49, BL-B01D1).
Figure 2 Mechanism of Action of ADCCore Components of ADCAntibody: An ideal antibody should have high specificity, low immunogenicity, long half-life, and ease of internalization.IgG1 is the most commonly used subtype (86.7%) due to its long half-life and strong immune effects.Bispecific antibodies (BsAbs) are the future trend, capable of targeting two antigens or epitopes simultaneously, enhancing specificity (e.g., ZW49, BL-B01D1).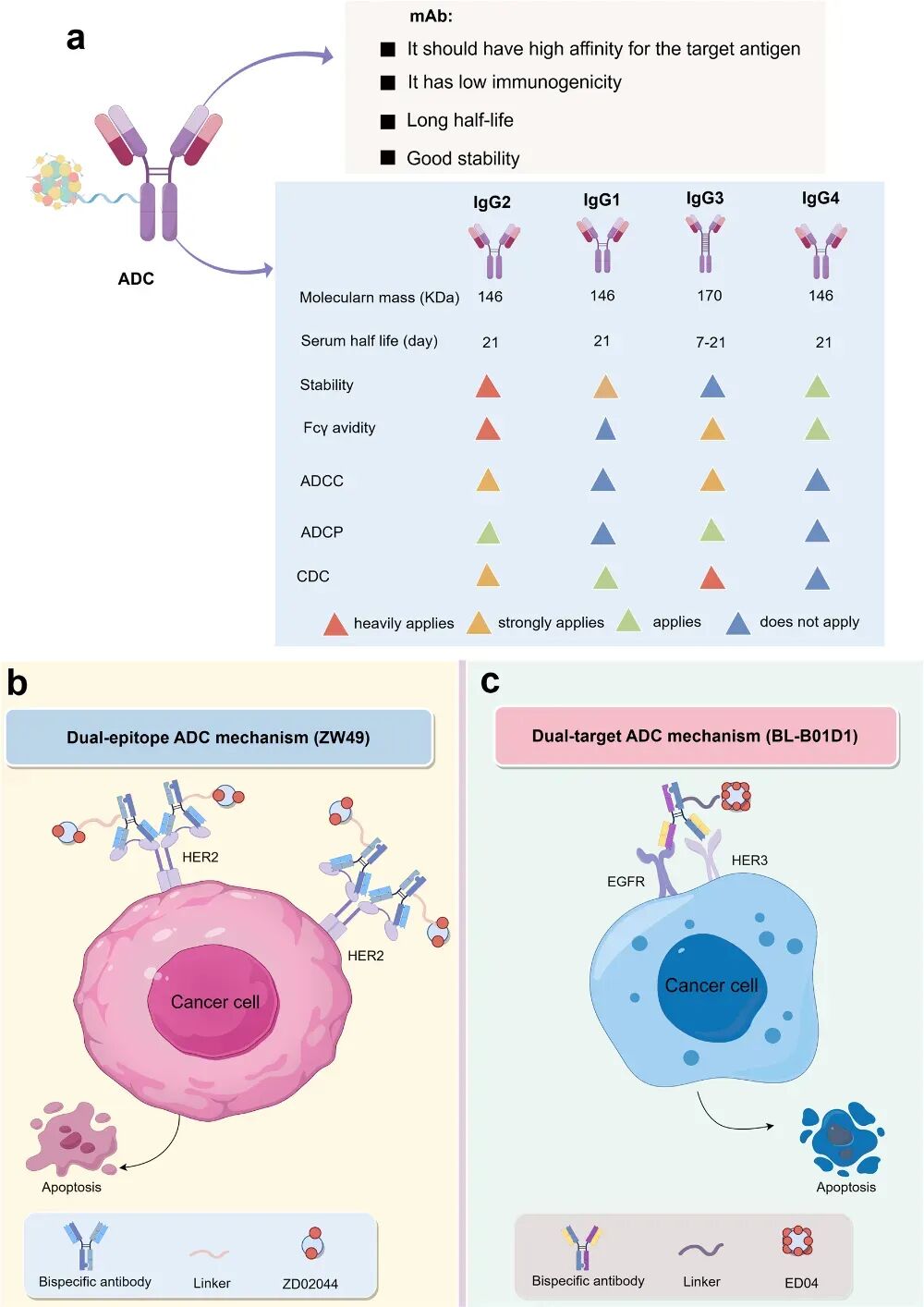 Figure 3 Antibodies in ADCTarget SelectionCommon targets for hematologic tumors:CD33, CD30, CD22, CD79b, BCMA, CD19.Common targets for solid tumors:HER2, TROP2, EGFR, Nectin-4, TF, FRα.HER2 is the most popular target, accounting for 20% of approved ADC drugs and 33.3% of Phase III ADC drugs.
Figure 3 Antibodies in ADCTarget SelectionCommon targets for hematologic tumors:CD33, CD30, CD22, CD79b, BCMA, CD19.Common targets for solid tumors:HER2, TROP2, EGFR, Nectin-4, TF, FRα.HER2 is the most popular target, accounting for 20% of approved ADC drugs and 33.3% of Phase III ADC drugs.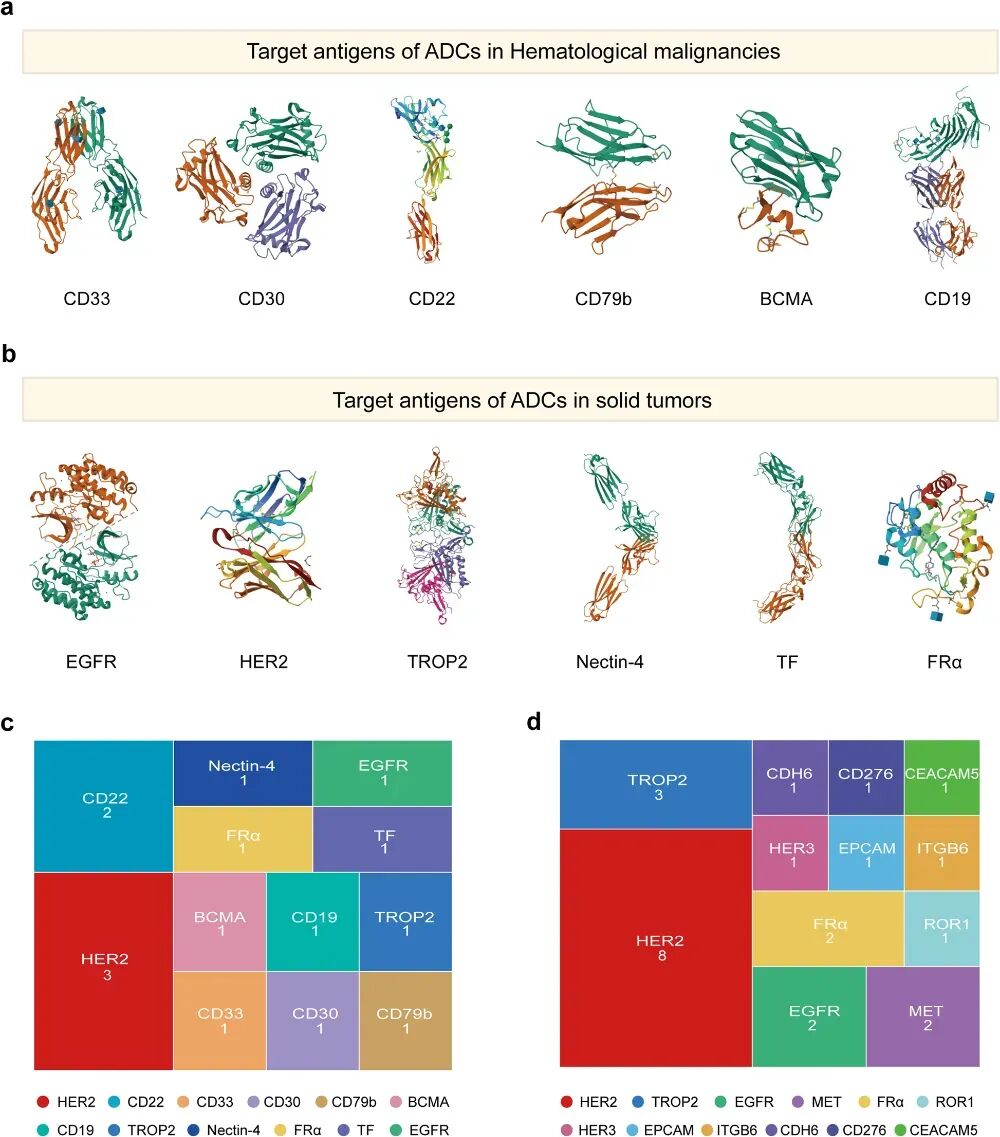 Figure 4 Targets of ADCLinkers are divided into cleavable and non-cleavable types (Fig. 5).Cleavable linkers:Chemically cleavable: e.g., hydrazone bonds (pH-sensitive), disulfide bonds (GSH-sensitive);Enzymatically cleavable: e.g., peptide linkers (Val-Cit, Gly-Gly-Phe-Gly), glycosidase linkers.Non-cleavable linkers:e.g., thioether bonds, maleimide, more stable but without bystander effect.73.3% of approved ADC drugs use cleavable linkers, with peptide linkers being the most common.
Figure 4 Targets of ADCLinkers are divided into cleavable and non-cleavable types (Fig. 5).Cleavable linkers:Chemically cleavable: e.g., hydrazone bonds (pH-sensitive), disulfide bonds (GSH-sensitive);Enzymatically cleavable: e.g., peptide linkers (Val-Cit, Gly-Gly-Phe-Gly), glycosidase linkers.Non-cleavable linkers:e.g., thioether bonds, maleimide, more stable but without bystander effect.73.3% of approved ADC drugs use cleavable linkers, with peptide linkers being the most common.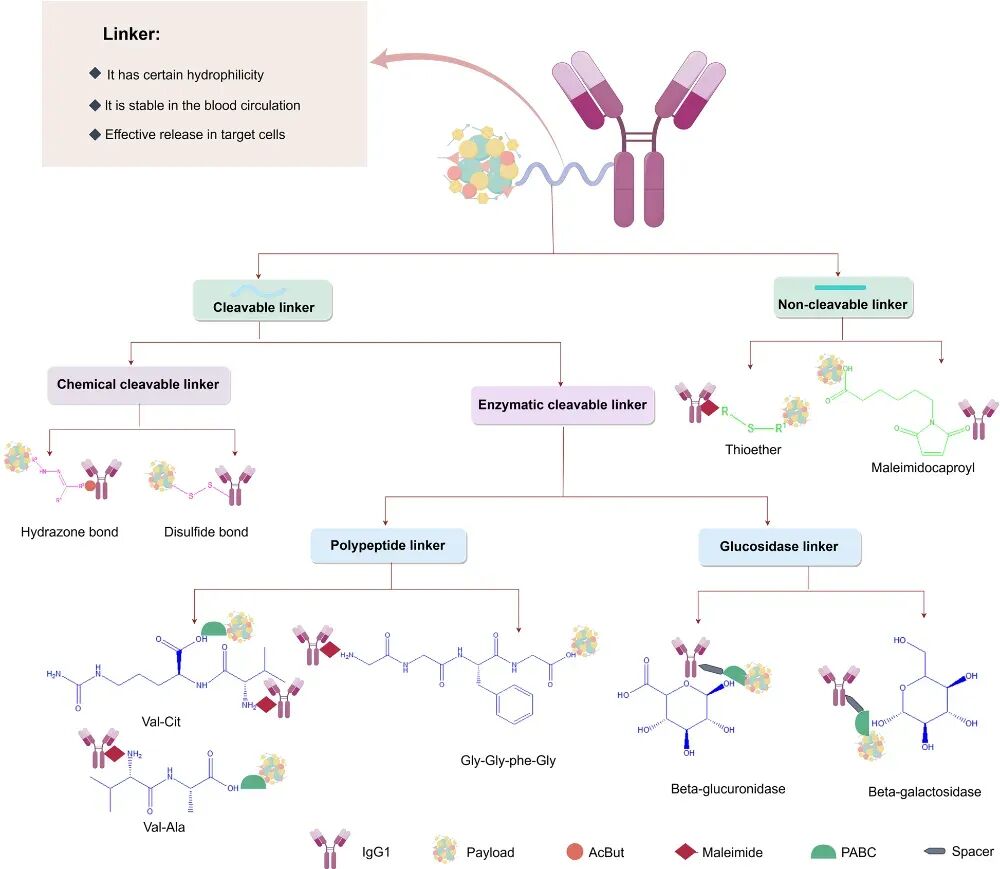 Figure 5 Types of Linkers in ADCPayloads mainly include:Microtubule inhibitors: e.g., MMAE, MMAF, DM1, DM4 (accounting for 53.3% of approved ADC drugs);DNA damaging agents: e.g., Calicheamicin, PBD;TOP1 inhibitors: e.g., DXd, SN-38 (accounting for 45.8% in Phase III ADC trials);Others: bacterial toxins (PE38), photosensitizers (IRDye700DX), etc.Development trends: expanding from traditional chemotherapy drugs to new payloads such as immune stimulators and RNA inhibitors.
Figure 5 Types of Linkers in ADCPayloads mainly include:Microtubule inhibitors: e.g., MMAE, MMAF, DM1, DM4 (accounting for 53.3% of approved ADC drugs);DNA damaging agents: e.g., Calicheamicin, PBD;TOP1 inhibitors: e.g., DXd, SN-38 (accounting for 45.8% in Phase III ADC trials);Others: bacterial toxins (PE38), photosensitizers (IRDye700DX), etc.Development trends: expanding from traditional chemotherapy drugs to new payloads such as immune stimulators and RNA inhibitors.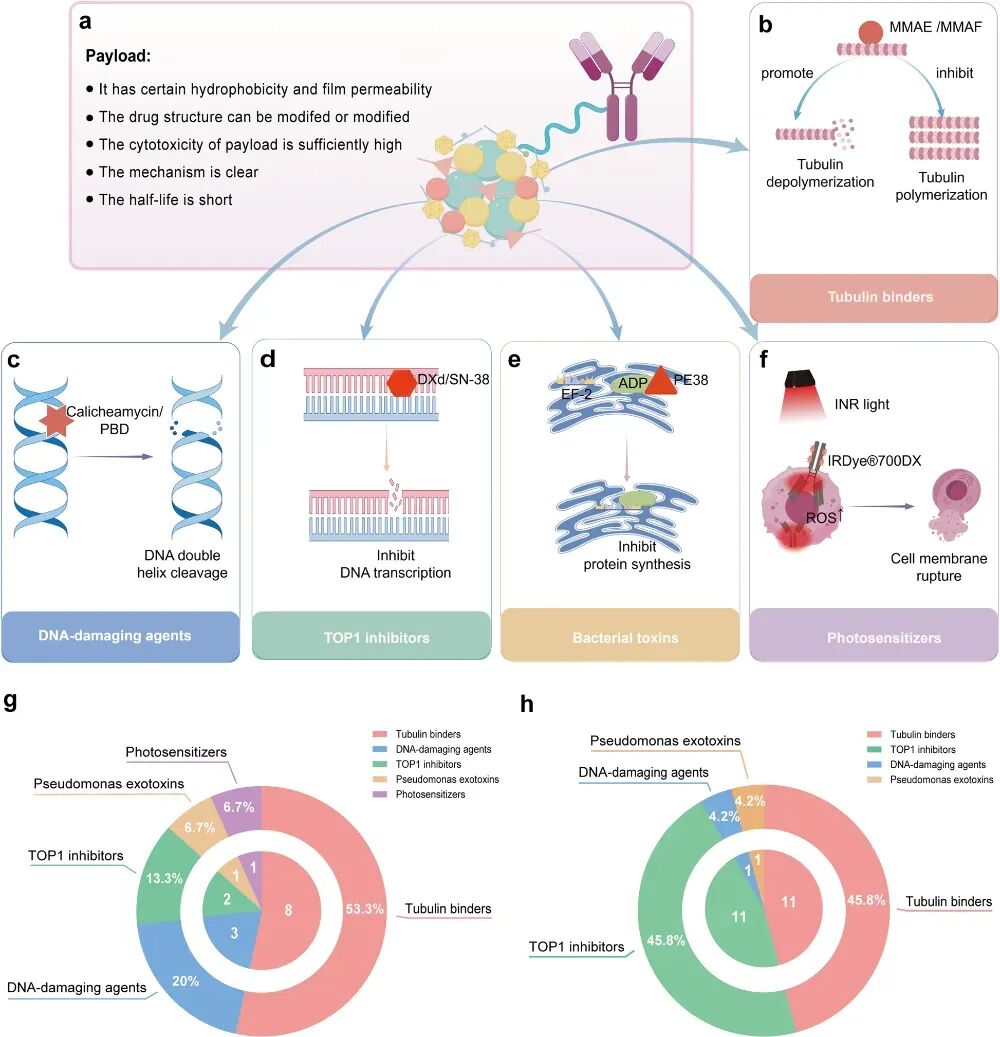 Figure 6 Payloads in ADCClinical Applications of Approved ADCHematologic tumors:Gemtuzumab ozogamicin: used for CD33+ AML, withdrawn due to unstable linker, later re-approved after dose optimization.Brentuximab vedotin: used for HL and ALCL, replacing vincristine in CHOP, significantly improving PFS.Polatuzumab vedotin: used for DLBCL, superior to R-CHOP when combined with R-CHP.Loncastuximab tesirine: the first PBD-class ADC, used for R/R DLBCL, has a strong bystander effect.Solid tumors:Trastuzumab emtansine (T-DM1): the first solid tumor ADC, used for HER2+ breast cancer.Trastuzumab deruxtecan (DS-8201): with a DAR of up to 7.8, effective even in low HER2 expression, overturning traditional classifications.Sacituzumab govitecan: targeting TROP2, used for triple-negative breast cancer and urothelial carcinoma.Enfortumab vedotin: targeting Nectin-4, used for urothelial carcinoma, showing significant effects when combined with PD-1 inhibitors.
Figure 6 Payloads in ADCClinical Applications of Approved ADCHematologic tumors:Gemtuzumab ozogamicin: used for CD33+ AML, withdrawn due to unstable linker, later re-approved after dose optimization.Brentuximab vedotin: used for HL and ALCL, replacing vincristine in CHOP, significantly improving PFS.Polatuzumab vedotin: used for DLBCL, superior to R-CHOP when combined with R-CHP.Loncastuximab tesirine: the first PBD-class ADC, used for R/R DLBCL, has a strong bystander effect.Solid tumors:Trastuzumab emtansine (T-DM1): the first solid tumor ADC, used for HER2+ breast cancer.Trastuzumab deruxtecan (DS-8201): with a DAR of up to 7.8, effective even in low HER2 expression, overturning traditional classifications.Sacituzumab govitecan: targeting TROP2, used for triple-negative breast cancer and urothelial carcinoma.Enfortumab vedotin: targeting Nectin-4, used for urothelial carcinoma, showing significant effects when combined with PD-1 inhibitors.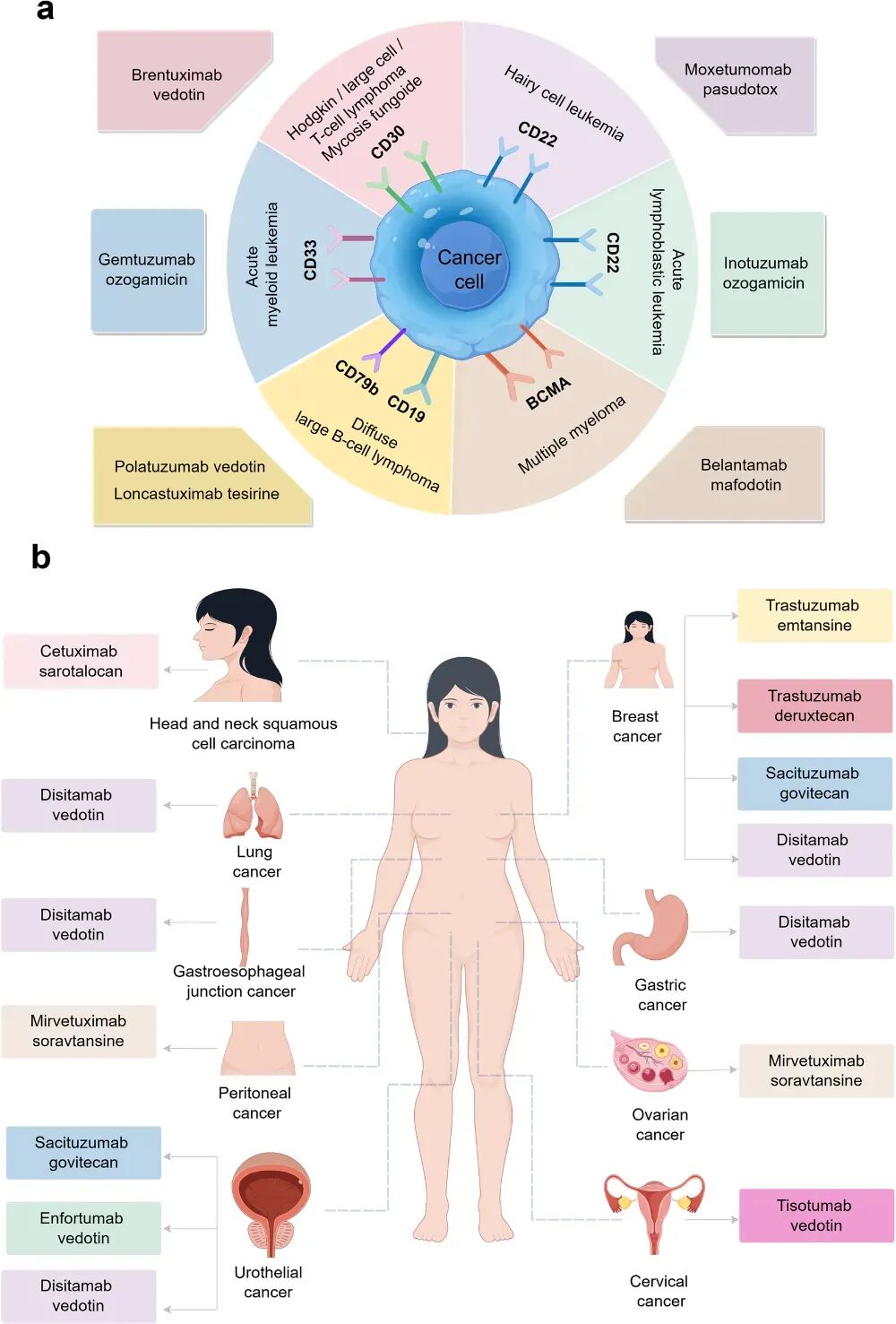 Figure 7 ADC for Hematologic and Solid TumorsCurrent Challenges for ADCToxicity management: e.g., neutropenia, ocular toxicity, thrombocytopenia;Resistance mechanisms: antigen downregulation, drug efflux, escape from signaling pathways;Heterogeneity issues: uneven DAR, aggregation, immunogenicity.Future DirectionsBispecific ADC: to improve targeting and internalization efficiency;New payloads: such as immune stimulators (TLR/STING agonists), RNA inhibitors (Amatoxin);Non-internalizing target ADC: such as CD20, CAIX, FAP;Non-tumor applications: such as autoimmune diseases, infectious diseases, neurological disorders.ADC represents a significant advancement in targeted cancer therapy, with its design concept evolving from “magic bullets” to “smart missiles.” Through continuous optimization of antibodies, linkers, and payloads, ADC has achieved significant improvements in efficacy and safety. In the future, with breakthroughs in bispecific antibodies, new payloads, and brain-targeting technologies, ADC is expected to play an important role in a wider range of disease areas.References:Wang R, Hu B, Pan Z, Mo C, Zhao X, Liu G, Hou P, Cui Q, Xu Z, Wang W, Yu Z, Zhao L, He M, Wang Y, Fu C, Wei M, Yu L. Antibody-Drug Conjugates (ADCs): current and future biopharmaceuticals. J Hematol Oncol.Akram F, Ali AM, Akhtar MT, Fatima T, Shabbir I, Ul Haq I. The journey of antibody-drug conjugates for revolutionizing cancer therapy: A review. Bioorg Med Chem.
Figure 7 ADC for Hematologic and Solid TumorsCurrent Challenges for ADCToxicity management: e.g., neutropenia, ocular toxicity, thrombocytopenia;Resistance mechanisms: antigen downregulation, drug efflux, escape from signaling pathways;Heterogeneity issues: uneven DAR, aggregation, immunogenicity.Future DirectionsBispecific ADC: to improve targeting and internalization efficiency;New payloads: such as immune stimulators (TLR/STING agonists), RNA inhibitors (Amatoxin);Non-internalizing target ADC: such as CD20, CAIX, FAP;Non-tumor applications: such as autoimmune diseases, infectious diseases, neurological disorders.ADC represents a significant advancement in targeted cancer therapy, with its design concept evolving from “magic bullets” to “smart missiles.” Through continuous optimization of antibodies, linkers, and payloads, ADC has achieved significant improvements in efficacy and safety. In the future, with breakthroughs in bispecific antibodies, new payloads, and brain-targeting technologies, ADC is expected to play an important role in a wider range of disease areas.References:Wang R, Hu B, Pan Z, Mo C, Zhao X, Liu G, Hou P, Cui Q, Xu Z, Wang W, Yu Z, Zhao L, He M, Wang Y, Fu C, Wei M, Yu L. Antibody-Drug Conjugates (ADCs): current and future biopharmaceuticals. J Hematol Oncol.Akram F, Ali AM, Akhtar MT, Fatima T, Shabbir I, Ul Haq I. The journey of antibody-drug conjugates for revolutionizing cancer therapy: A review. Bioorg Med Chem. Disclaimer: This article is based on existing public information and literature data, and has no conflicts of interest with any organization or individual. For clinical medication, please refer to clinical guidelines or consult a physician.If there are any copyright issues, please contact the medical academic within 30 days of publication.Unauthorized reproduction of original content on other platforms is prohibited.©2021 Medical Academic. All rights reserved.
Disclaimer: This article is based on existing public information and literature data, and has no conflicts of interest with any organization or individual. For clinical medication, please refer to clinical guidelines or consult a physician.If there are any copyright issues, please contact the medical academic within 30 days of publication.Unauthorized reproduction of original content on other platforms is prohibited.©2021 Medical Academic. All rights reserved.