Antibody-drug conjugates (ADC) are a new class of targeted drugs composed of monoclonal antibodies (mAbs), cytotoxic drugs, and linkers that connect the two. They utilize the targeting capability of antibodies to selectively deliver cytotoxic molecules to tumor cells, exerting anti-cancer effects while avoiding impacts on healthy cells.
ADC drugs have rapidly developed in the field of breast cancer treatment, with 3 out of the 12 FDA-approved ADC drugs having indications for breast cancer. HER-2 is the most explored target, while other targets include trophoblast cell surface antigen 2 (TROP-2), LIV-1 (zinc transporter ZIP6), and HER-3.
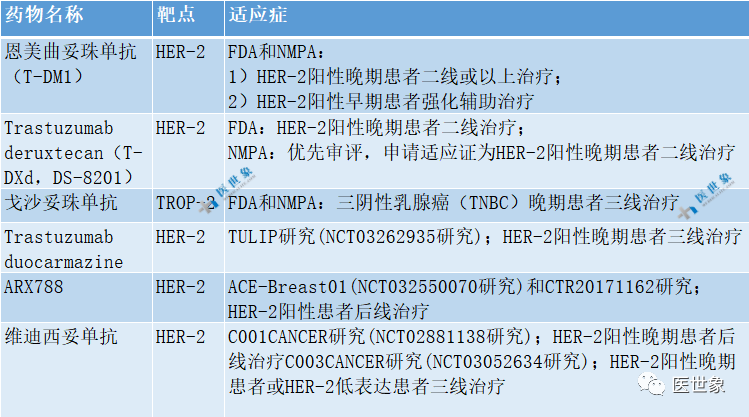
Currently, the three ADC drugs with FDA-approved indications for breast cancer areTrastuzumab emtansine (T-DM1), Trastuzumab deruxtecan (T-DXd, also known as DS-8201), and sacituzumab govitecan, with T-DM1 and sacituzumab govitecan also approved domestically. Additionally, three other ADC drugs [Trastuzumab duocarmazine (SYD985), ARX788, and vadastuximab talirine (RC48)] have entered clinical trials for breast cancer.
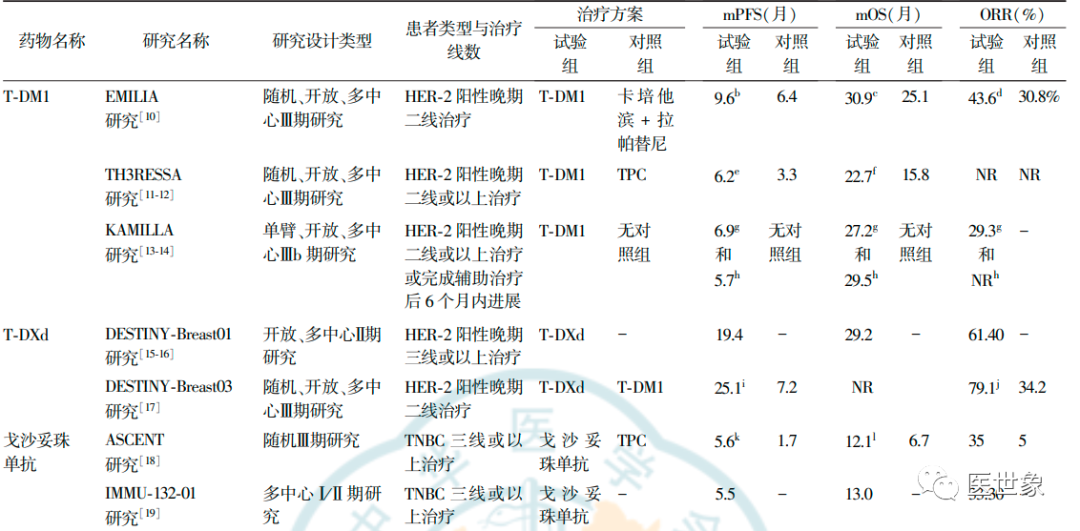
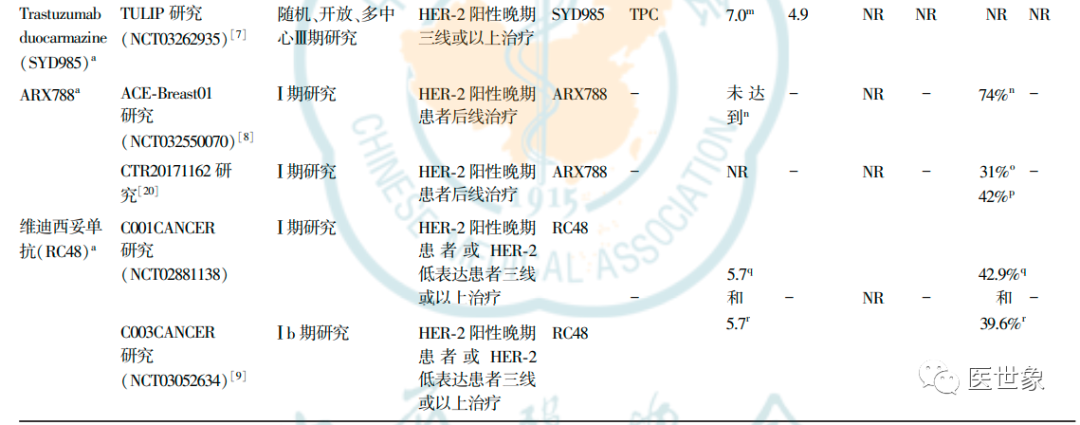
Key Research on the Effectiveness of ADC Treatment for Advanced Breast Cancer
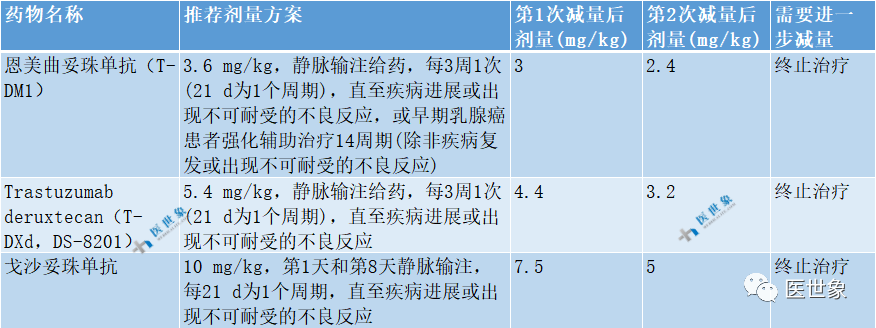
Recommended Dosage Schemes for ADC Drugs with Breast Cancer Indications
Common or Special Attention Adverse Reactions or Adverse Event Grading Standards and Management for ADC Drug Treatment in Breast Cancer Patients
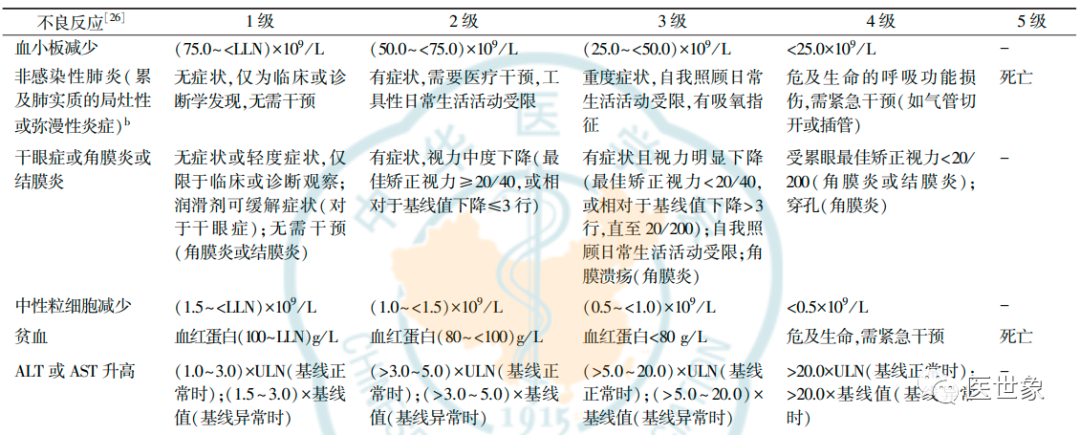
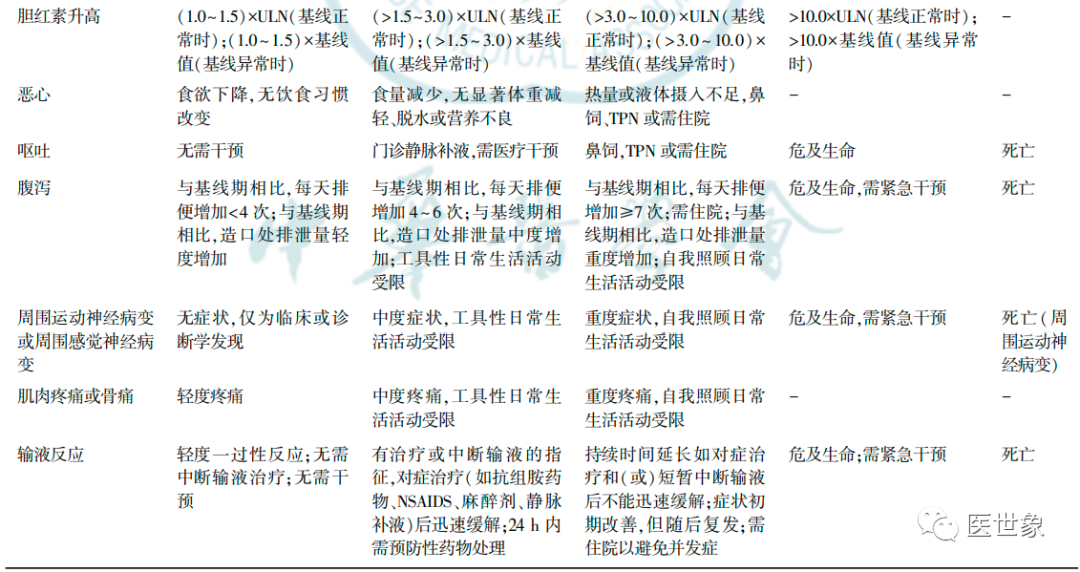
1. Adverse Reactions Requiring Special Attention
1. Pulmonary Adverse Reactions
Interstitial Lung Disease (ILD) is a heterogeneous group of diseases characterized by lung inflammation and/or fibrosis caused by various factors. The actual sequence of onset includes a series of inflammation and fibrosis. ILD not only disrupts the interstitial bed but also alters the parenchyma (alveoli, alveolar ducts, and bronchioles), with complications including worsening hypoxia, cardiovascular disease, pulmonary hypertension, and infections. Drug-induced ILD is one known cause.
The most commonly reported symptom of ILD is gradually worsening dyspnea, but sometimes cough is the only complaint. Pleuritic chest pain and hemoptysis are relatively rare. Patients may be completely asymptomatic but have imaging abnormalities. Bilateral basal crackles are a typical sign, but not necessarily found during every physical examination. Complete blood count may indicate eosinophilia; the most common X-ray feature is reticular opacities, and nodular or mixed patterns may also be seen. High-resolution CT (HRCT) typically shows changes primarily affecting the pleura and basal membrane, manifesting as reticular, honeycombing with or without traction bronchiectasis. Among the anti-HER-2 ADCs, T-DXd has the highest ILD-related mortality (1.7%~2.2%), while other HER-2 ADCs (including T-DM1 and Trastuzumab duocarmazine) have an ILD-related mortality of 0.1%~0.6%.
Standard Symptomatic Management Process for ADC Treatment-Related ILD or Non-Infectious Pneumonitis
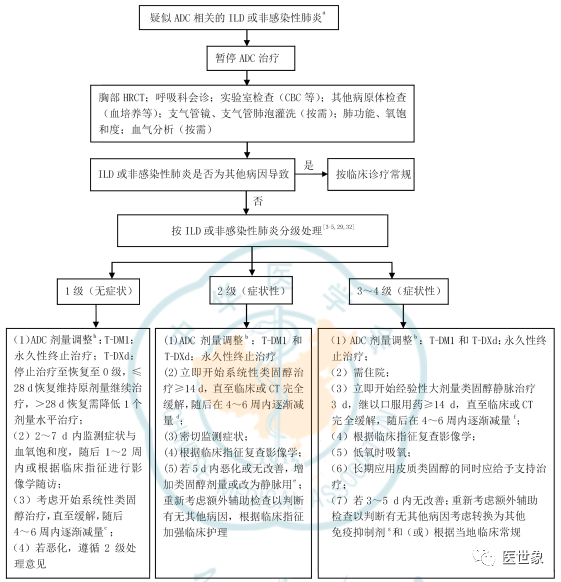
Patients with a history of lung disease should use T-DXd or T-DM1 cautiously. If treatment is initiated, close monitoring for signs of pulmonary lesions is required to detect and avoid severe ILD or non-infectious pneumonitis early. It is recommended to monitor and assess signs and new or worsening respiratory symptoms every 4-6 weeks. During treatment, once ILD or non-infectious pneumonitis is suspected, treatment should be suspended, and corticosteroid therapy should be considered immediately. After diagnosis, dosage should be adjusted based on the severity of ILD or non-infectious pneumonitis.
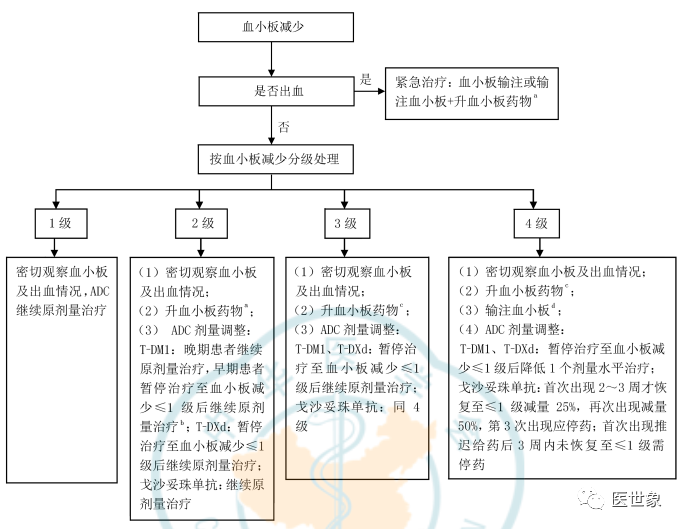
2. Thrombocytopenia
Thrombocytopenia is the most common drug-related adverse reaction among patients receiving T-DM1 treatment, with higher incidence and severity in Asian patients. During T-DM1 treatment, thrombocytopenia is the primary reason for dose reduction or even discontinuation. The platelet count in patients receiving T-DM1 typically drops to its lowest value on day 8 and recovers to grades 0-1 before the next scheduled dose.
Grade ≥3 thrombocytopenia occurring during T-DM1 treatment rarely leads to grade ≥3 bleeding.
It is recommended to monitor platelet counts before each administration. For patients with thrombocytopenia who are receiving anticoagulant therapy, close monitoring is essential. Patient education should also be provided to avoid bleeding.
The vast majority of thrombocytopenia can recover after treatment is paused, reduced, or terminated. Symptomatic supportive treatment should be provided as necessary, including addressing any other potential causes of thrombocytopenia, such as controlling infections or coagulopathy; platelet transfusions when indicated (e.g., when platelet count ≤10×10^9/L), and treatments to promote platelet production, including:
(1) Administering recombinant human interleukin-11 when thrombocytopenia is ≥2; (2) Administering recombinant human thrombopoietin (rhTPO) when thrombocytopenia is ≥2; (3) Thrombopoietin receptor agonists (TPO-RA) for patients whose platelet count has not recovered to ≤1 before the next T-DM1 treatment.
Standard Symptomatic Management Process for ADC Treatment-Related Thrombocytopenia
In clinical practice, the recommended dosage of rhIL-11 is 25-50 μg/kg, subcutaneously, once daily, for 7-10 days, until platelet counts return to normal or increase by 50×10^9/L compared to pre-treatment levels. During treatment, close monitoring and timely management of related adverse reactions, such as allergic or hypersensitivity reactions, atrial arrhythmias, and syncope, as well as more common issues like edema and fluid retention, should be conducted.
Recommended dosage of rhTPO is 300 U/(kg·d), once daily, for 14 days, until platelet counts return to normal or increase by 50×10^9/L compared to pre-treatment levels. Monitor complete blood count twice weekly, and in special circumstances, once every other day. Among patients experiencing rare severe persistent thrombocytopenia (≥3 and lasting more than 90 days) after T-DM1 treatment, the majority received rhTPO therapy, so attention should be paid to the ongoing status of persistent thrombocytopenia when using rhTPO.
TPO-RA is a second-generation platelet growth factor used during persistent thrombocytopenia and cannot replace platelet transfusions; the recommended dosage is romiplostim 2-3 μg/kg weekly, or eltrombopag 50-75 mg/day, until platelet counts return to normal.
3. Ocular Adverse Reactions
Limited data indicate that ocular adverse reactions typically occur after ≥2 treatment cycles, affecting the ocular surface, including keratitis, dry eye syndrome, corneal microcysts or deposits, and conjunctivitis. The most common symptom reported by patients is blurred vision, followed by decreased vision and diplopia. Ocular adverse events in patients treated with Trastuzumab duocarmazine are a major reason for discontinuation (10%-20.8%), including dry eye syndrome, conjunctivitis, and keratitis, with an incidence approaching 40%. Reports of dry eye syndrome have also been made in studies of T-DM1 and T-DXd, with incidences of 4% and 11%, respectively; conjunctivitis incidence related to T-DM1 is also 4%.
Slit-lamp examination is a standard method for diagnosis and assessment. Grade 1 adverse events can be managed with preservative-free artificial tears while continuing treatment at the original dose; grade 2-3 adverse events require treatment suspension, and autologous serum eye drops may be used, with a downgrade of one dose level to continue treatment once symptoms improve; grade 4 should result in treatment termination. The use of steroid medications should be avoided. If symptoms worsen or if grade 2 or higher adverse events occur, an ophthalmology consultation should be requested.

2. Common Adverse Reactions
1. Neutropenia
ADCs contain chemotherapeutic drug components, and thus can cause neutropenia, with sacituzumab govitecan being the most pronounced. Patients undergoing treatment with sacituzumab govitecan may experience severe or even life-threatening neutropenia. The median time to first occurrence for any grade and grade ≥3 neutropenia is 19 and 17 days, respectively, with median durations of 8.5 and 8 days.
Granulocyte colony-stimulating factor (G-CSF) is the standard medication for treating neutropenia.Patients with neutropenia accompanied by fever or recurrent infections must immediately begin anti-infective treatment. Empirical antibiotic treatment should be chosen based on the patient’s risk level, with high-risk patients requiring antifungal prophylaxis.
For patients receiving sacituzumab govitecan, G-CSF may be considered as secondary prophylaxis.For patients known to have decreased UGT1A1 enzyme activity, or those showing evidence of decreased UGT1A1 enzyme activity, such as acute early onset or abnormally severe adverse reactions, close monitoring is required, and treatment should be paused or stopped as necessary. UGT1A1 genetic testing has been proposed to reduce the risk of adverse reactions in high-risk UGT1A1 genotype patients and to maximize efficacy in low-risk UGT1A1 genotype patients through dose escalation.
2. Anemia
Chemotherapeutic drugs induce anemia by directly damaging hematopoiesis, including the synthesis of erythroid progenitor cells. Consistent with the characteristics of neutropenia in patients receiving sacituzumab govitecan treatment, homozygous individuals for the UGT1A1*28 allele have an increased risk of anemia, with the incidence of grades 3-4 anemia being 25%, while the incidence in heterozygous and wild-type homozygous subgroups is 10% and 11%, respectively.
For patients with anemia, the benefits and risks of transfusion should be weighed based on clinical symptoms, malignancy course, treatment response, comorbid conditions, or potential causes, as well as patient preferences, to select appropriate symptomatic supportive treatments, including the use of erythropoiesis-stimulating agents or red blood cell transfusions as necessary. During sacituzumab govitecan treatment, acute early onset or abnormally severe adverse reactions suggest the possibility of decreased UGT1A1 enzyme activity, and these patients should be closely monitored for complete blood counts.
3. Cardiac Adverse Reactions
Cardiac adverse reactions generally manifest clinically as decreased exercise tolerance due to dyspnea or fatigue, as well as fluid retention, such as swelling in the lower limbs or abdomen, difficulty lying flat, and weight gain; they may also be asymptomatic or accompanied by other cardiac or non-cardiac symptoms. The incidence of cardiac adverse reactions reported in T-DM1 and T-DXd studies is not high.
Decreased left ventricular ejection fraction (LVEF) is a known risk of trastuzumab, noted in the black box warning of T-DM1 and the warnings and precautions section of T-DXd. Routine cardiac function checks should be performed before starting treatment, with LVEF re-evaluated every 3 months during treatment. Non-invasive quantitative assessment methods include echocardiography, magnetic resonance imaging, CT, multi-gated acquisition scanning, and gated myocardial perfusion imaging. Patients with low baseline LVEF should carefully assess the benefit-risk ratio before deciding on treatment.
Decreased LVEF is associated with poor prognosis, and treatment methods depend on the underlying cause. The best management model for decreased LVEF involves interdisciplinary collaboration, including cardiologists, nutritionists, and pharmacists.
LVEF is the core indicator of left ventricular systolic function. Clinically, a simple classification based on the American College of Cardiology is commonly used: high output: LVEF >70%; normal: LVEF 50%-70%; mild abnormal: LVEF 40%-49%; moderate abnormal: LVEF 30%-39%; severe abnormal: LVEF <30%.
4. Hepatobiliary Adverse Reactions
Targeted therapy can cause liver adverse reactions. Meta-analysis shows that T-DM1 treatment is associated with an increased risk of elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST), as well as elevated bilirubin laboratory markers. The black box warning for T-DM1 indicates that some patients receiving T-DM1 have experienced liver adverse reactions, liver failure, and death.
Liver function should be monitored before starting T-DM1 treatment and before each administration, and patients should be vigilant for clinical symptoms of portal hypertension and/or CT evidence of cirrhotic-like changes. Patients receiving T-DM1 have been observed to develop regenerative nodules in the liver, which can only be diagnosed through histopathology. When clinical symptoms of portal hypertension and/or CT shows cirrhotic-like changes, but transaminases are normal and there are no other signs of cirrhosis, all patients should be considered for the possibility of liver regenerative nodules. For early and late breast cancer patients, the dosage adjustment scheme for T-DM1 differs; any grade of liver regenerative nodules in either early or late breast cancer patients should lead to termination of T-DM1 treatment. If drug-induced liver injury occurs in late breast cancer patients [serum ALT or AST >3× upper limits of normal (ULN) and total bilirubin >2×ULN], treatment should be permanently terminated after excluding other causes.
5. Gastrointestinal Adverse Reactions
Nausea, vomiting, and diarrhea are common and severe gastrointestinal adverse reactions among patients treated with sacituzumab govitecan. The median time to onset and duration of any grade diarrhea related to sacituzumab govitecan is 14.0 and 8.0 days, respectively, with grade ≥3 diarrhea lasting 15 and 6 days. Reports of gastrointestinal adverse reactions have also been made for T-DXd and T-DM1, with relatively mild severity.
The black box warning for sacituzumab govitecan indicates the possibility of severe diarrhea, and monitoring should be conducted with fluid and electrolyte administration as needed. Pre-treatment with antiemetics is recommended before starting treatment. If there are no contraindications, atropine can be used to pre-treat and control any early-onset diarrhea of any severity. For late-onset diarrhea, infectious causes should be assessed, and if no other triggers are found, loperamide should be used immediately, starting with a dose of 4 mg, followed by 2 mg for each subsequent diarrhea episode, with a maximum daily dose of 16 mg. Loperamide should be discontinued 12 hours after diarrhea resolution. For patients whose diarrhea does not resolve, the aforementioned loperamide regimen can be given every 2 hours; if there is no improvement after 24 hours, octreotide 100-150 mg should be considered, 3 times daily. Severe diarrhea should be managed with hospitalization.
6. Neurological Adverse Reactions
Peripheral neuropathy includes lesions of peripheral nerve cells and fibers, with clinical manifestations and severity related to extensive pathological changes affecting motor, sensory, and autonomic nerve fibers. Peripheral neuropathy is not always reversible, with common symptoms including numbness (hypoesthesia) and sensory abnormalities, which may also be accompanied by pain, weakness, and loss of deep tendon reflexes.
Currently, there are no effective drugs to prevent or treat chemotherapy-induced neuropathy, with duloxetine being the only medication with evidence for painful peripheral neuropathy, but its efficacy is limited. Based on clinical experience, dexamethasone pre-treatment may help reduce the occurrence of neuropathy. When making treatment decisions, the expected benefit/risk ratio should be weighed. Management of peripheral neuropathy caused by ADC treatment can refer to guidelines for managing chemotherapy-induced peripheral neuropathy, with dose delays, reductions, switching regimens, or termination of ADC treatment considered for intolerable neuropathy and/or functional impairment.
7. Musculoskeletal Adverse Reactions
T-DM1 and sacituzumab govitecan have reported various categories and degrees of musculoskeletal pain and arthralgia, with current reports indicating grade 1-2, requiring no special management. In rare severe cases, dose adjustments and symptomatic supportive treatment may be conducted.
8. Infusion Reactions
The incidence of infusion-related reactions for T-DM1 is 1.4%-1.6%, while for T-DXd it is 2.6%. Infusion reactions often manifest as flushing, chills, fever, dyspnea, hypotension, wheezing, bronchospasm, and tachycardia. Patients should be closely monitored for infusion reactions, especially during the first infusion. The first infusion time for T-DM1 and T-DXd should be >90 min; if well tolerated, subsequent infusion times can be >30 min. The first infusion time for sacituzumab govitecan should be >3 hours; if well tolerated, subsequent infusions can be maintained at 1-2 hours. Patients should be observed for symptoms or signs for at least 30 minutes during and after the infusion of sacituzumab govitecan. If an infusion reaction occurs, the infusion rate should be slowed or the infusion should be paused; if a severe or life-threatening infusion reaction occurs, treatment should be permanently discontinued.
Prior to each infusion of sacituzumab govitecan, antipyretics, H1 and H2 receptor blockers may be pre-administered, and glucocorticoids may be used in patients with a history of infusion reactions. Additionally, a two-drug (e.g., dexamethasone combined with a 5-HT3 receptor antagonist or NK1 receptor antagonist) or three-drug (building on the two-drug regimen, the third medication can be selected based on indications) pre-treatment regimen can be employed.
Patients with a known history of severe infusion-related reactions or hypersensitivity reactions to any component of the ADC should not use this drug.
For common adverse reactions, the general adjustment strategies are:
(1) Grade 1 generally requires no special management; (2) Grade 2 requires treatment suspension until the adverse reaction recovers to ≤1, after which treatment can continue at the original dose or a dose reduction of one level (if recovery time >3 weeks); (3) Grade 3-4 adverse reactions require treatment suspension until recovery to ≤1, after which a dose reduction of one level should be continued; if recovery does not occur within 3 weeks, treatment should be considered for termination.
The above principles for dosage adjustments of currently approved ADCs are general guidelines; in clinical practice, it is essential to follow the latest version of each drug’s instructions for dose reduction or treatment termination.
Cited from: Breast Cancer Group of the Oncology Physician Branch of the Chinese Medical Doctor Association, International Medical Exchange Branch of the Chinese Anti-Cancer Association. Expert Consensus on the Safety Management of Antibody Drug Conjugates for Breast Cancer in China [J]. Chinese Journal of Oncology, 2022, 44(9): 913-927. DOI: 10.3760/cma.j.cn112152-20220521-00360.Written by: Yuan Peng (National Cancer Center, National Clinical Research Center for Cancer, Special Medical Department, Peking Union Medical College Cancer Hospital), Xu Ling (Breast Disease Center, Peking University First Hospital)This article is compiled by Yishixiang Zorro, please contact us for authorization.
Join Hands Against Cancer
The fight against cancer is long and painful. Communication between patients and their families with doctors or cancer friends can provide some treatment assistance and spiritual comfort; we have established support groups for various types of cancer, hoping to provide some help. Currently, there are support groups for lung cancer, breast cancer, liver cancer, colorectal cancer, gastric cancer, and pancreatic cancer.
Patients or family members in need, as well as healthcare friends willing to help, can apply to join the group. Group management personnel WeChat: 13023252650, please add a note indicating cancer type + identity (patient or healthcare).
Recommended Reading:
1. The National Health Commission has clearly requested that these genes be listed as essential testing items!
2. 90% of cancer patients die from metastasis! What is cancer metastasis all about?
3. The Fudan University Shanghai Medical Team has discovered the secret of folic acid-induced cancer! Is it safe for pregnant women to supplement folic acid?
4. About 30% of early-stage lung cancer patients will relapse and metastasize after surgery! How do experts predict cancer recurrence?
5. The Lancet: Ping Pong and other racket sports can reduce all-cause mortality by 47%!6.[Free Medication] New Drug for Stomach Cancer: A New Type of Anti-HER2 ADC Drug [T-DXd]7. Small pulmonary nodules; 80% of young doctors do not consider this diagnosis.8.China’s first! A popular science manual for the diagnosis and treatment of small cell lung cancer patients.9.How to choose third-generation TKI after resistance to first/second-generation EGFR-TKI in lung cancer?10. The “miracle drug” metformin shows new progress in cancer treatment! Promotes NK cell function, becoming a new way of tumor treatment in conjunction with immunotherapy.——End of this issue——We (Yishixiang, WeChat ID: medhealife)are committed to reporting research results in the field of tumors and disseminating popular science knowledge;focusing on tumor prevention, early screening and diagnosis, treatment, and rehabilitation management throughout the entire tumor life cycle, providing the latest information for doctors, patients, and related personnel;contributing to the benefit of medicine for the public.
