Recently, there has been a piece of news that is quite eye-catching.On November 19, 2025, the ADC biotechnology company Lifordi Immunotherapeutics announced the completion of a new round of strategic financing amounting to $42 million. The funds will primarily be used for ADCs beyond oncology—specifically, LFD-200, which targets VISTA, one of the most competitive emerging targets (both in cancer and autoimmunity).
Earlier, ABBV-773 had also been in the spotlight for a long time; domestically, one of the leading ADC companies, Yingen Biotech, is working hard to develop DB-2304, which is also an ADC drug for autoimmunity.
The author believes that under these circumstances, ADC drug therapy may be a very important potential trend in the future, and we must pay attention to it. Today, the author mainly uses the development journey of ABBV-773 to write this article, hoping to provide some help to future researchers.
01
The Birth of Pioneer ABBV-773
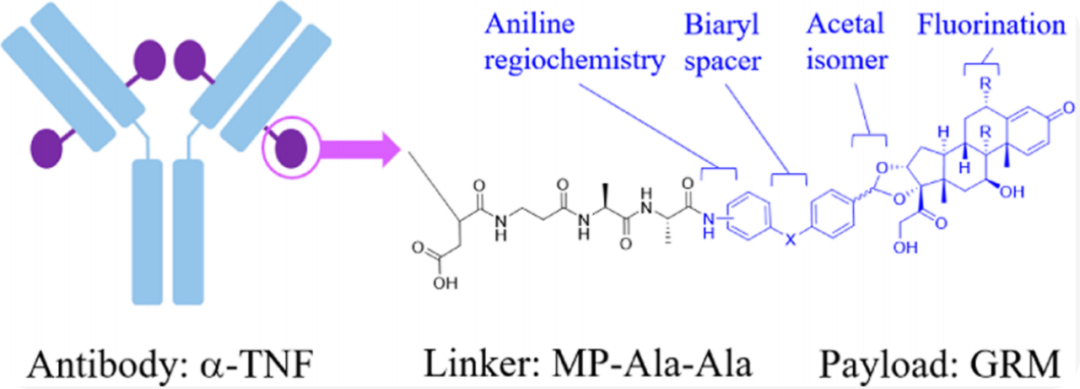
AbbVie, the pioneer in this era of competition, is the company that produced the autoimmunity drug Humira, and ABBV-773 is the first anti-inflammatory ADC to enter clinical trials. The specific preparation and screening process of this drug can be referenced in the article published in the ACS journal titled “Discovery of ABBV-3373, an Anti-TNF Glucocorticoid Receptor Modulator Immunology Antibody Drug Conjugate”; the literature details the screening process very thoroughly.
Here, we will not elaborate on the screening process of the payload, but will mention one point regarding the linker: the hydrolysis of the maleimide ring can stabilize the drug conjugate’s binding to the antibody, preventing it from easily undergoing decoupling through reverse Michael reactions. This mechanism, combined with direct action, attaches the dipeptide linker to the aniline of the drug molecule via an amide bond, forming a stable ADC. This stability has been validated in a crab-eating macaque model, and no changes in DAR were observed within two weeks.
Here, we will focus on the screening of the in vivo model: the mouse abdomen was sensitized with fluorescein isothiocyanate (FITC), and after 6 days, FITC was administered in the ear, leading to increased swelling in the ear. Before sensitization with FITC, a single treatment with 10 mg/kg or 3 mg/kg of the candidate ADC drug was given to assess the impact of the ADC drug on ear swelling. All candidate ADC molecules inhibited ear swelling, and no significant differences in efficacy were observed between the two tested doses.
In addition, the safety of the ADC must also be evaluated, specifically its impact on hormones in the body. To assess the effects of the ADC on corticosterone and P1NP, mice were stimulated with adrenocorticotropic hormone (ACTH) 72 hours after ADC administration, and plasma was collected 30 minutes later to measure corticosterone, testosterone, and P1NP levels. Unlike the effects on inflammation (where small differences were observed among the ADC molecules), some candidate molecules showed weak effects on corticosteroids, while others showed stronger effects, as seen in the significant differences below. No P1NP was detected at the tested doses—this indicates that these ADCs may have a wider therapeutic window.
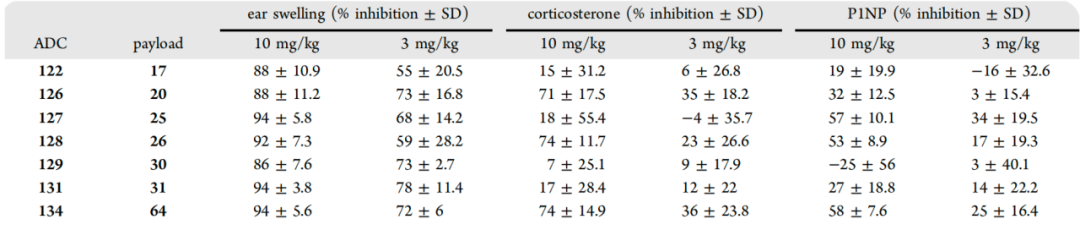
Subsequently, the trials were advanced to evaluate the anti-inflammatory effects of the ADC candidate molecules in a chronic inflammatory environment, leading to multiple ADCs being advanced into a mouse collagen-induced arthritis (mCIA) model, which essentially replicates many pathological features of human RA (rheumatoid arthritis) indications. The selected candidates were 122, 129, and 131, along with 126; the first three drugs showed good inhibition of inflammatory swelling with minimal hormonal impact, while 126 exhibited some inhibitory effects on hormones—moderate impact on P1NP but still significantly inhibited corticosterone.
Finally, in terms of efficacy, 122 and 129 showed a dose-dependent decrease in efficacy, while 126 and 131 showed similar effects in reducing paw swelling at both doses.
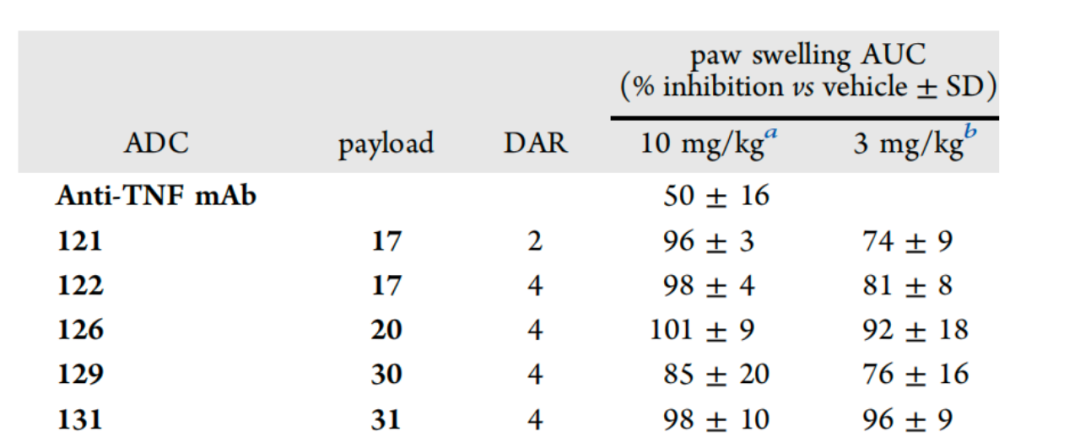
In the mCIA model, the effects of all four ADCs on paw swelling reduction lasted for more than 30 days after a single administration. Moreover, all ADCs showed significantly better efficacy than the parent monoclonal antibody (Adalimumab).
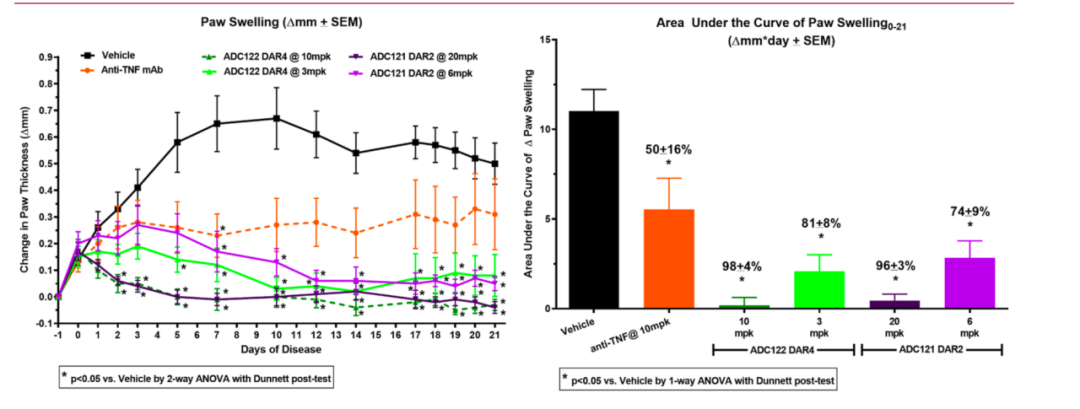
We can see that the final selections were molecules 122 and 121, both of which had similar efficacy at high doses, but considering the impact on hormones, 122 had a smaller hormonal impact, thus it was chosen. This molecule was used to prepare the human antibody, which is the well-known ABBV-3373.
02
Clinical Trials of ABBV-3373
Finally, we arrived at the clinical trial phase. First, the Phase I trial assessed safety and tolerability in adults.
Overall, the pharmacokinetic characteristics of ABBV-3373 for subcutaneous and intravenous administration were similar to those of antibodies, with Cmax and AUC increasing with dose, and the duration of drug exposure was prolonged. The pharmacokinetic characteristics of ABBV-3373 and TAb were generally similar, with Tmax reached approximately 3 days after subcutaneous administration, followed by a clear single exponential decline, with a half-life of about 2 to 8 days. After intravenous administration, the serum concentration of ABBV-3373 decreased rapidly in the initial phase, consistent with typical intravenous administration characteristics, and then entered a slower elimination phase similar to that of the 300 mg subcutaneous administration group, with a half-life of about 4 to 12 days.
The concentration of unbound active payload was several orders of magnitude lower than that of ABBV-3373. Notably, the exposure of the active payload after subcutaneous injection appeared to be dose-dependent, while after intravenous injection, it deviated from the dose proportionality. Unlike ABBV-3373, the exposure of the active payload after subcutaneous injection was higher than that after intravenous injection at the same dose level.
Overall, the pharmacokinetic comparison of ABBV-3373 with the naked antibody Adalimumab showed that ABBV-3373 had a faster systemic clearance rate and shorter average half-life compared to Adalimumab. After a single subcutaneous injection, the average clearance rate and half-life of ABBV-3373 were as high as 79.3 mL/h and 7.4 days, respectively, while the average clearance rate and half-life of Adalimumab after a single subcutaneous injection were 20.0 mL/h and 20 days, respectively. The differences can be attributed to the impact of drug conjugation on the antibody scaffold (e.g., reduced hydrophilicity) and are consistent with observations of other ADC drugs.
In terms of safety, except for a transient decrease in serum cortisol levels at the 900 mg intravenous dose, there was no significant impact on serum cortisol levels.
Then came the Phase IIa trial. Adult patients with moderate to severe rheumatoid arthritis (RA) receiving background treatment with methotrexate were treated with either intravenous ABBV-3373 100 mg every two weeks for 12 weeks, followed by placebo treatment for 12 weeks; or subcutaneous Adalimumab 80 mg every two weeks for 24 weeks. The primary endpoint was the change in the 28-joint disease activity score (DAS28-CRP) from baseline at week 12.
As shown, although ABBV-3373 (-2.65) was significantly better than placebo and significantly better than historical data for Adalimumab (-2.13), p=0.022, it can be seen that under this trial, the difference between ABBV-3373 and the data for Adalimumab in the trial was not very large. Moreover, in terms of secondary endpoints, the drug and Adalimumab showed similar efficacy across most indicators.
(Image Source:https://acrjournals.onlinelibrary.wiley.com/doi/10.1002/art.42415)
In terms of safety, overall, ABBV-3373 data appears to be much better. In the active control phase (weeks 0-12), the overall incidence of treatment-emergent adverse events (TEAEs) in the ABBV-3373 treatment group (35.5%) was lower than that in the Adalimumab group (70.6%). Four patients receiving ABBV-3373 reported serious adverse events (SAEs) (non-cardiac chest pain, pneumonia, upper respiratory infection, and anaphylactic shock). Among them, two cases of serious infection were moderate and were considered not reasonably related to the study drug, resolving within 9-12 days.
However, at week 24, 40.0% (n = 12) and 17.6% (n = 3) of patients were found to have treatment-emergent anti-drug antibodies. Among patients treated with ABBV-3373, one patient developed treatment-emergent anti-drug antibodies at week 12, with a high titer (>100), and experienced anaphylactic shock after the fourth week of administration, leading to permanent discontinuation of the drug.
Looking back, it is speculated that the adverse reaction event led to the termination of this therapy in 2020, which is indeed regrettable.
03
The Future of Autoimmunity ADCs
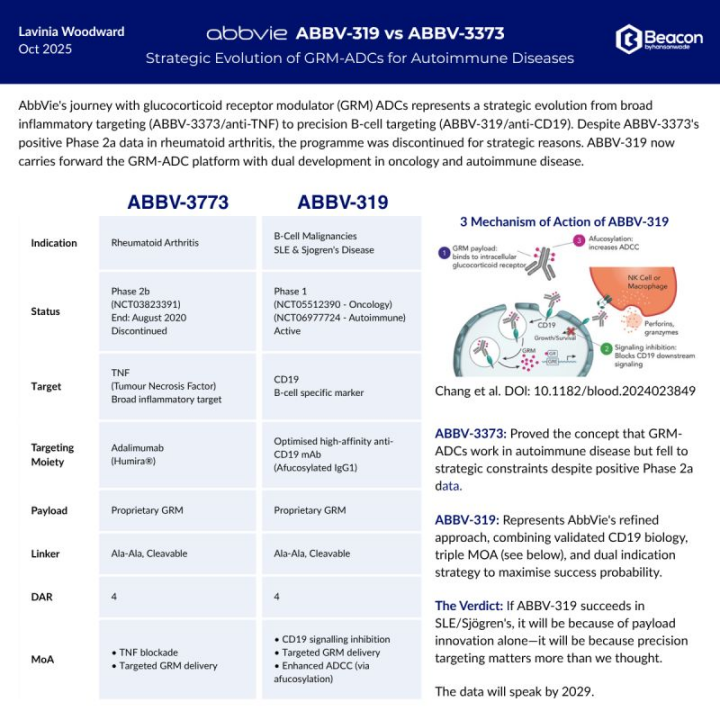
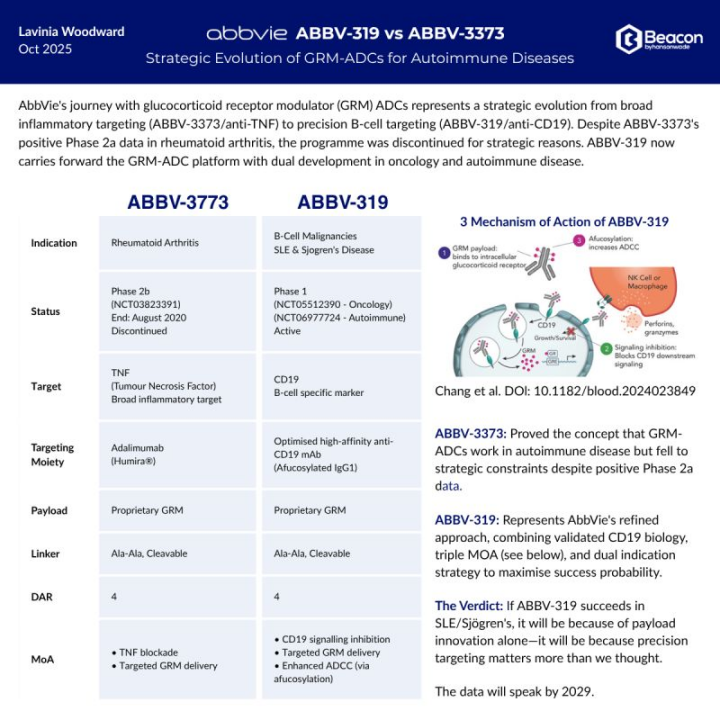
However, in August 2025, AbbVie introduced a new ADC with glucocorticoids as the payload. Its main target is CD19, but it is not for autoimmunity; rather, it is for B-cell lymphoma. It aims to reduce glucocorticoid-related toxicity while having three different mechanisms of action (MOA) to enhance therapeutic efficacy: (1) antibody-mediated delivery of glucocorticoid receptor modulators (GRM) effective payloads to induce apoptosis; (2) inhibition of the CD19 signaling pathway; (3) enhancement of Fc fragment-mediated effector functions through the deglycosylation of the antibody scaffold.
ABBV-319 has shown potent GRM-driven anti-tumor activity in vitro against various malignant B cell lines, as well as in in vivo xenograft models and patient-derived xenograft models (PDX).
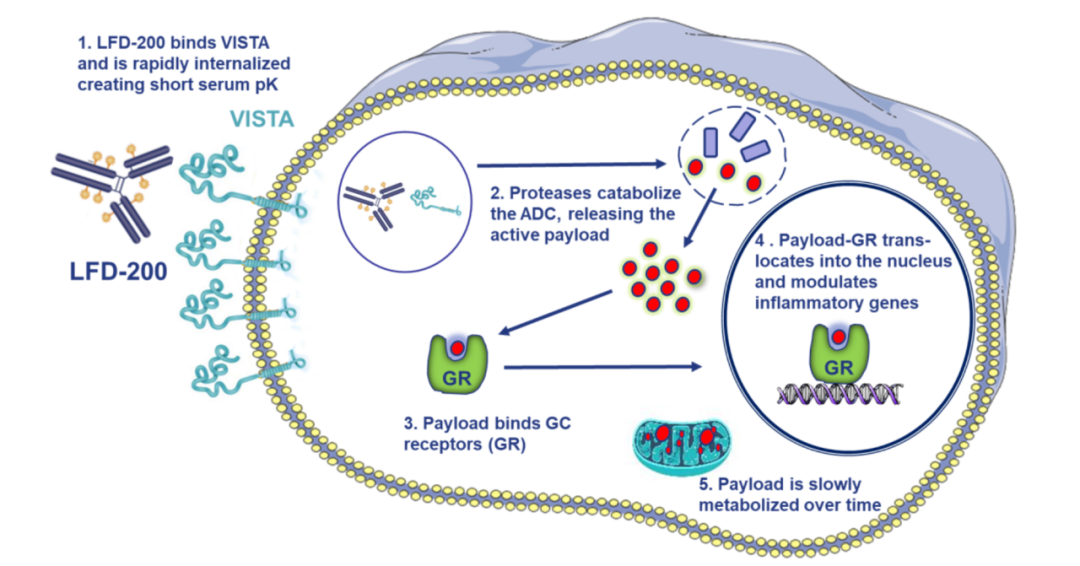
Additionally, as mentioned at the beginning of the article, VISTA may be a promising target for future autoimmunity ADCs. The unique biological characteristics of VISTA, such as its rapid internalization and intracellular accumulation, make it an ideal choice for ADC therapy. Lifordi’s main ADC candidate, LFD-200, has shown in preclinical studies that it has a short serum half-life, long retention time in immune cells, and can exert long-term immunosuppressive functions within these cells without causing systemic administration-related toxicity.
Currently, its clinical Phase I trial for RA is ongoing. This double-blind, randomized, single/multiple dose (SAD/MAD) Phase I clinical trial plans to recruit 176 subjects across seven research centers outside the United States. The study will evaluate the safety, tolerability, pharmacokinetics, and pharmacodynamics of subcutaneously administered LFD-200.
This Phase I clinical trial is based on previous results presented at the American College of Rheumatology (ACR), which showed that LFD-200 could achieve at least 7 days of sustained glucocorticoid (GC) exposure in immune cells of non-human primates (NHP). After administration of clinically relevant doses for 13 weeks, the candidate drug also inhibited the expression of pro-inflammatory cytokines, with no observed toxic reactions.
Domestically, Yingen Biotech has built its own platform in this area—DIMAC. DIMAC provides targeted treatment solutions with lower systemic exposure, stronger efficacy, and better safety to reshape the treatment of autoimmune diseases. Molecules developed on the DIMAC platform have demonstrated effective and broad anti-inflammatory activity in preclinical studies, with long drug action duration, high stability, and low systemic exposure, promising to provide patients with chronic autoimmune diseases with treatments that have lower side effects and higher efficacy.
Currently, its flagship pipeline DB-2304 targeting BDCA2 has entered Phase I clinical trials.
Conclusion: In any case, the failure of ABBV-3373 provides us with very valuable experience, such as its efficacy being not significantly different from that of Adalimumab, and it led to a severe allergic reaction in one patient, but it still paved a new path for future researchers—a new path to reduce the side effects of inflammation treatment.
——-THE END———-
Disclaimer: This article is a reprint and share; the views, content, images, and copyrights belong to the original author. If there is any infringement, please contact for removal!