Important targets for targeting prostate cancer (PCa) include: prostate-specific membrane antigen (PSMA), six-transmembrane epithelial antigen 1 (STEAP-1), solute carrier family 44 member 4 (SLC44A4), trophoblast cell surface antigen (Trop-2) and B7-H3.
Introduction
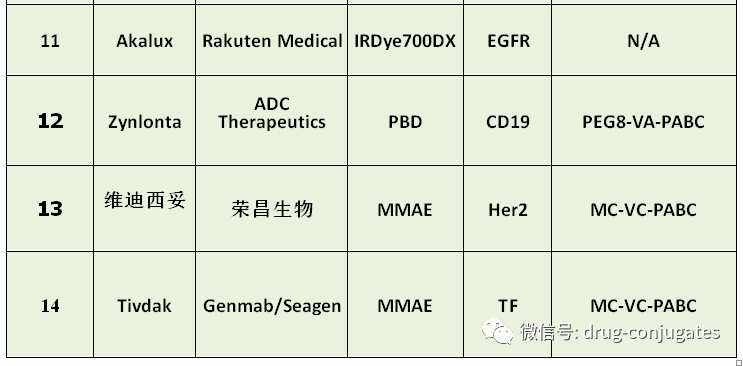
Antibody-drug conjugates (ADCs) consist of a linker, payload, and monoclonal antibody (mAb). They combine the advantages of high specificity targeting and potent killing effects, achieving precise and efficient destruction of cancer cells, and have become a hot topic in the development of anti-cancer drugs. Since the first ADC drug, Mylotarg ®, was approved by the FDA in 2000, as of December 2021, a total of 14 ADC drugs have been approved for hematological malignancies and solid tumors globally, and there are currently over 100 ADC candidates in various stages of clinical trials.

In 2021, 34,130 people died from prostate cancer (PCa) in the United States. Currently, there are limited treatment options available for refractory metastatic prostate cancer, and the prognosis is poor. Progress of antibody-drug conjugates (ADCs) in PCa is still unsatisfactory!
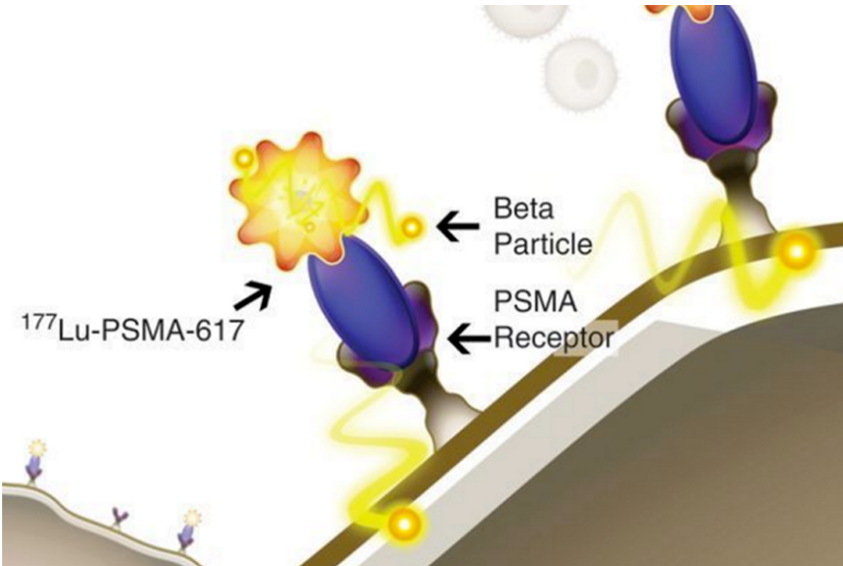
Approved ADC drugs for the treatment of prostate cancer177Lu-PSMA-617 (Pluvicto: Novartis)
On March 23, 2022, Novartis announced that the FDA has approved the company’s targeted radioligand therapy Pluvicto (lutetium Lu 177 vipivotide tetraxetan, 177Lu-PSMA-617) for the treatment of prostate-specific membrane antigen (PSMA) positive, treatment-experienced castration-resistant prostate cancer (mCRPC) patients. The approval of Pluvicto is based on data from the Phase III VISION trial, which showed an overall response rate (ORR) of 30%, with a complete response (CR) rate of 6%, and a 38% reduction in the risk of death. Pluvicto is the world’s first approved therapeutic drug targeting PSMA(PS: Novartis’s peptide-nuclide conjugate should be considered a PDC).
So far, no ADC has been approved for prostate cancer (PCa). Next, let’s take a look at the targets of ADCs in prostate cancer and the global clinical trial progress.
Structure of Antibody-Drug Conjugates (ADCs)
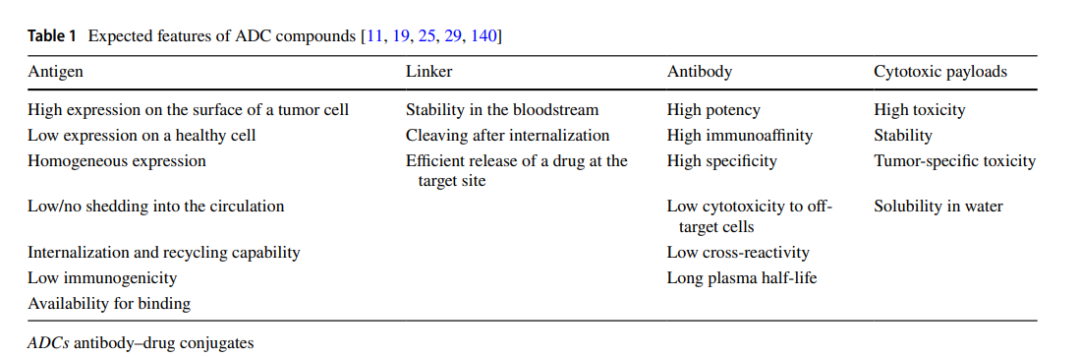
ADCs are composed of an antibody, an active payload, and a chemical linker. An ideal ADC drug remains stable in circulation, accurately reaches the therapeutic target, and ultimately releases the cytotoxic payload near the target (such as cancer cells). Each component affects the final efficacy and safety of the ADC. Overall, the development of ADCs requires consideration of all these key components, including targets, antibodies, cytotoxic payloads, linkers, and the choice of conjugation methods.

Structure and key elements of ADCs
ADC targets for prostate cancer and clinical progress
Androgen deprivation therapy (ADT) is an important treatment for prostate cancer (PCa). However, especially for castration-resistant disease, treatment options also include chemotherapy, anti-androgen therapy, radiolabeled therapy, gene-targeted therapy, immune checkpoint inhibitors, and autologous cell immunotherapy.
Important targets for targeting prostate cancer (PCa) include: prostate-specific membrane antigen (PSMA), six-transmembrane epithelial antigen 1 (STEAP-1), solute carrier family 44 member 4 (SLC44A4), trophoblast cell surface antigen (Trop-2) and B7-H3. Below we will introduce the status of these targets and the ADC drugs in clinical stages.
PSMA
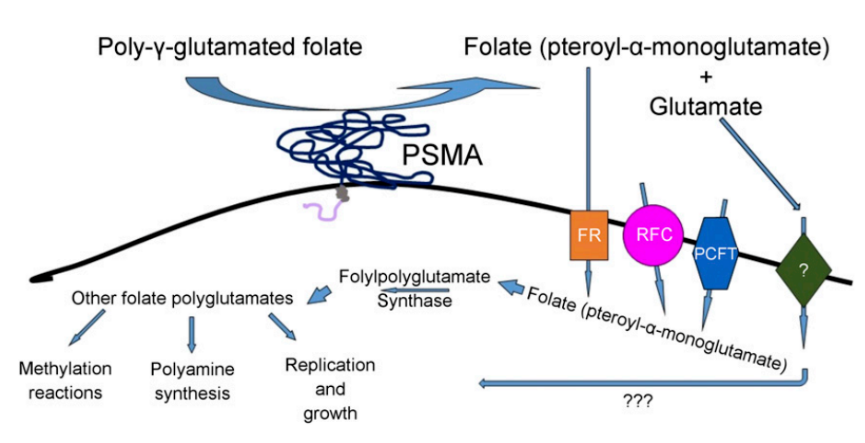
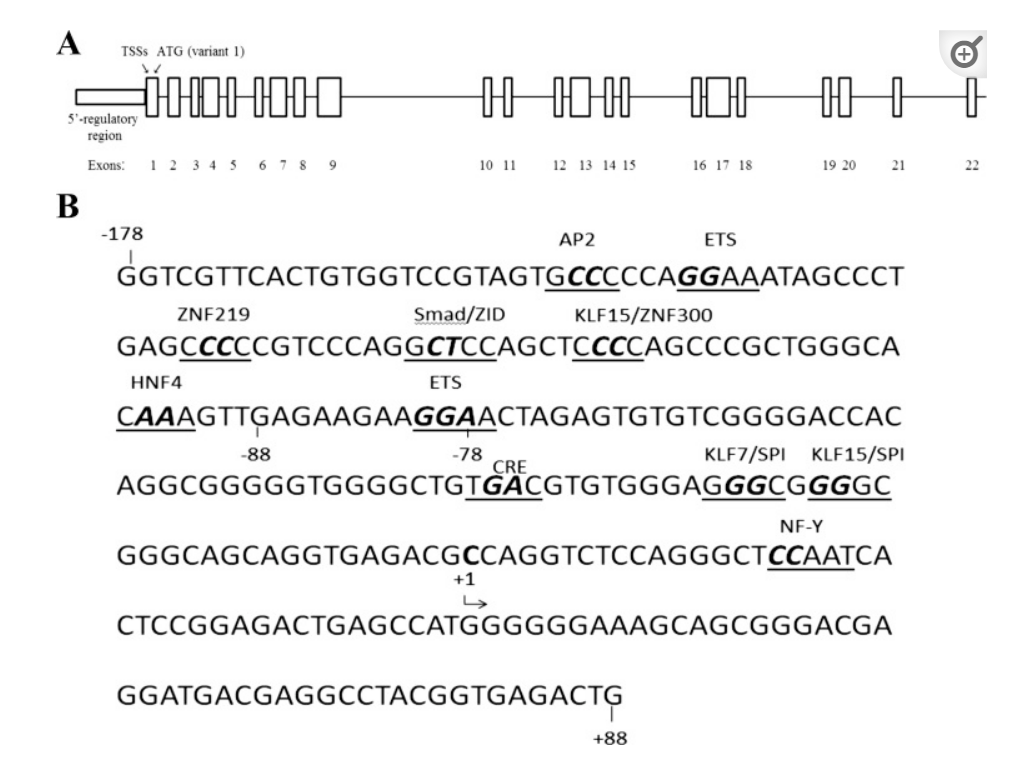
PSMA is a type II transmembrane glycoprotein with high specificity for the prostate, possessing carboxypeptidase activity that catalyzes the hydrolysis of N-acetyl aspartyl glutamate to glutamate and N-acetyl aspartate. It consists of a 19-amino acid intracellular domain, a 24-amino acid transmembrane domain, and a 707-amino acid extracellular domain. The FOLH1 (folate hydrolase 1) gene of PSMA is located on chromosome 11, and its expression is regulated by androgen signaling. PSMA is primarily expressed on the surface of prostate epithelial cells, with lower expression observed in the proximal tubules of the kidney outside the prostate, small intestine brush border, Schwann cells, and astrocytes. Upon activation, PSMA is rapidly internalized within the cell.
PSMA levels are more than 1000 times higher in PCa than in benign prostate tissue, and increase during androgen deprivation and anti-androgen treatment. Additionally, PSMA is expressed in the tumor-associated neovasculature. Preclinical studies in PCa have shown that PSMA is involved in proliferation, migration, and survival through MAPK and PI3K-AKT pathways. PSMA expression is associated with tumor staging, Gleason scores, prostate-specific antigen (PSA) at diagnosis, tumor angiogenesis, and ERG (ETS-related gene) negativity in primary PCa;
Clinical progress of PSMA-targeted ADCs
ADCs targeting PSMA studied in clinical trials include MLN2704 and PSMA-ADC MEDI3726.
NCT00052000 is a Phase I non-randomized trial aimed at assessing the dose-limiting toxicity (DLT), maximum tolerated dose (MTD), and pharmacokinetics of MLN2704. The study recruited 23 hormone treatment-failed mCRPC patients. Using a traditional 3 + 3 dose escalation scheme, the dose range was 18 – 342 mg/m2. The most common CTC grade 1-2 adverse events (AEs) included fatigue (65%), nausea (56%), and diarrhea (39%). 35% of patients experienced neuropathy (13% CTC grade 1, 22% CTC grade 2). Only 13% of patients had CTC grade 3 drug-related toxicity, and no CTC grade 4 toxicity was reported. MTD was not reached. The most common DLT was febrile neutropenia.
NCT00070837 is a Phase I/II clinical trial based on the positive results of NCT00052000, aiming to assess the dose, pharmacokinetics, immunogenicity, and tumor response of MLN2704. A total of 62 mCRPC patients were recruited. The dose range was 60-462 mg/m2, with four different administration schemes administered intravenously. Peripheral neuropathy was the most common adverse reaction to the drug, occurring in 71% of enrolled patients. In 10% of cases, neuropathy was clinically significant (CTC grade 3/4). Other common AEs included nausea (61%), fatigue (60%), anorexia, and diarrhea (39%). Only 5 patients (8%) showed a PSA decline of over 50%. No PR or complete response (CR), 35% of patients achieved stable disease (SD).
NCT01414283 Phase I clinical trial aimed to confirm the role of PSMA-targeted ADC in taxane-resistant mCRPC patients. Establishing MTD was the primary endpoint. The study recruited 52 patients who received 0.4-2.8 mg/kg PSMA ADC for up to four cycles, Q3W. MTD was determined to be (2.5 mg/kg). Neutropenia was the dose-limiting factor, reaching a nadir two weeks after administration. Approximately 50% of patients achieved promising anti-tumor responses, measured as circulating tumor cell conversion or PSA reduction.
NCT01695044 Phase II trial is a continuation of NCT01414283 Phase I trial. This trial is a single-arm study, with mCRPC patients (n=119) divided into those who have not received chemotherapy (n=35) or docetaxel pre-treated (n=84) groups.
NCT02991911 Phase I/Ib trial aimed to evaluate the safety, pharmacokinetics, immunogenicity, and anti-tumor activity of MEDI3726 in mCRPC patients after non-response to enzalutamide or abiraterone. 33 patients received MEDI3726. Due to AEs (90.9%), study results were limited, including grade 3 or 4 CTC in 45.5% of patients; median progression-free survival (PFS) was 3.9 months, and median OS was 10.6 months. Preclinical studies have shown that the activity of MEDI3726 depends on phosphorylated histone H2AX and has shown activity in xenograft and cell line studies.
5D3-DM1 is a novel anti-PSMA antibody that has promising characteristics as a drug, with efficacy results recently published by Huang et al. 5D3-DM1 is characterized by higher affinity than J591 antibody, rapid internalization and centrosome localization capability, persistence, and effective drug release. The drug has shown good anti-tumor activity both in vitro and in vivo. Responses were observed in PSMA-positive cells, but minimal anti-tumor activity was seen in PSMA-negative cells. The toxicity was low, with no significant renal or liver damage.
STEAP-1
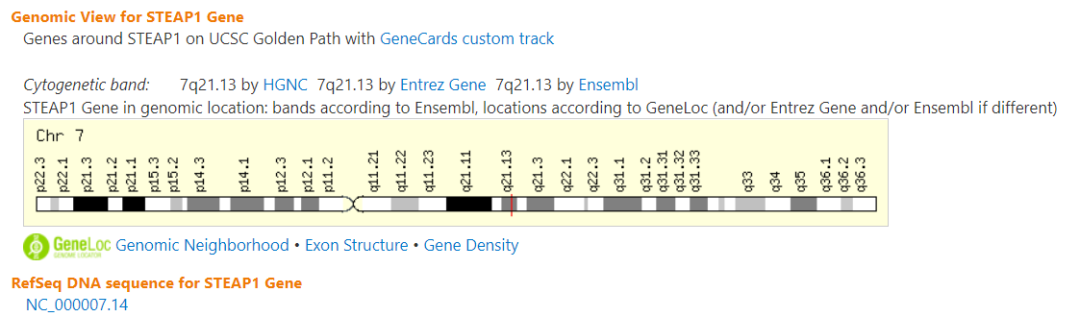
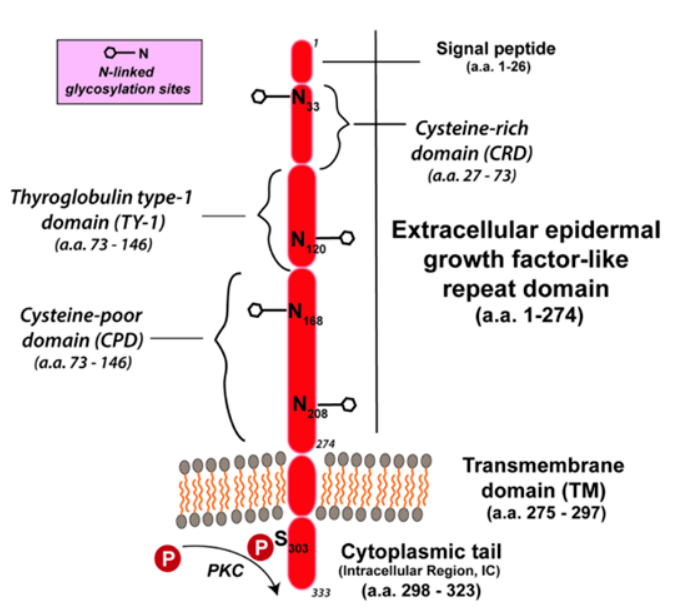
STEAP-1 protein is a 339-amino acid cell surface antigen that may act as an ion channel or protein transporter. In humans, the STEAP-1 gene is located on chromosome 7. An IHC study confirmed its high expression in prostate epithelial cells, particularly at cell-cell junctions. STEAP-1 expression has been observed at all clinical stages of PCa. In non-prostate tissues, STEAP-1 is moderately expressed in bladder cells and is overexpressed in cancers other than PCa, such as rhabdomyosarcoma, bladder cancer, colon cancer, and ovarian cancer. STEAP regulates tumor growth by modulating intracellular communication between tumor and stroma . The expression profile of STEAP-1 makes it a promising drug target. Additionally, STEAP has been used in peptide-based vaccines. A preclinical study in PCa and BCa xenografts showed that anti-STEAP antibodies could inhibit tumor growth.
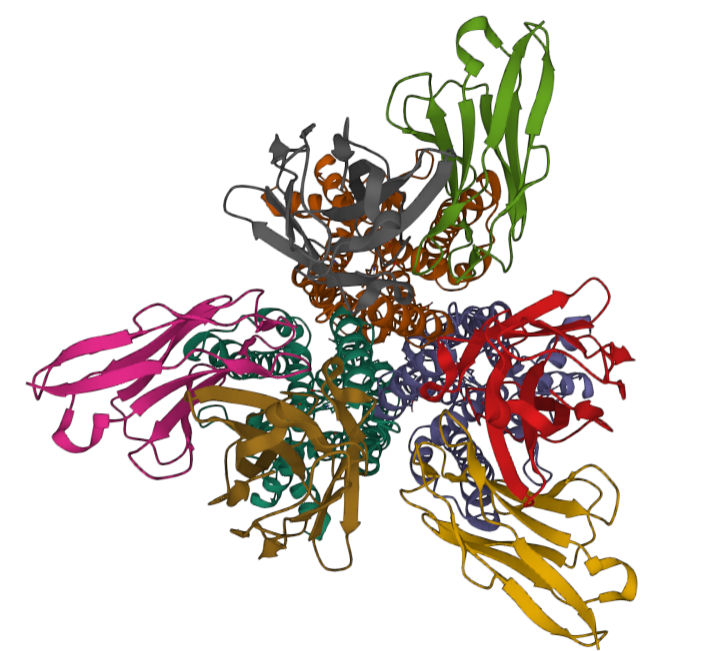
PDB:6Y9B Cryo-EM structure of trimeric human STEAP1 bound to three Fab120.545 fragments
Clinical progress of STEAP-1-targeted ADCs
Vandortuzumab vedotin (VV) is currently the only ADC targeting STEAP-1 in PCa research. NCT01283373 is a Phase I study that evaluated the safety and pharmacokinetics of increasing doses of VV (DSTP3086S) in mCRPC patients. A total of 84 patients were enrolled. The dose escalation group included intravenous injections of 0.3-2.8 mg/kg VV every 3 weeks (28 patients) and weekly treatments (7 patients). In the initial expansion group, 10 patients received 2.8 mg/kg treatment, while 39 patients in two expansion cohorts received 2.4 mg/kg treatment. The most common AEs were fatigue (56%), peripheral neuropathy (51%), and nausea (38%). 31% of 77 patients experienced grade 3 or 4 AEs. Those who received >2 mg/kg of the study drug achieved an 18% PSA decline, radiographic response (6%), and circulating tumor cell conversion (59%). The trial confirmed that DSTP3086S ADC has acceptable safety and shows activity in mCRPC patients.
SLC44A4
SLC44A4 or choline transporter-like protein 4 is a transmembrane protein belonging to the choline transporter family. SLC44A4 is involved in the synthesis of non-neuronal acetylcholine and is expressed in epithelial secretory prostate cells. IHC studies have shown that SLC44A4 is upregulated in several tumors, including 85% of primary PCa. Its higher expression has been demonstrated in poorly differentiated tumors. In vivo studies revealed that SLC44A4-targeted antibodies have anti-tumor activity in androgen-dependent and independent tumor xenografts. ASG-5ME is an ADC drug targeting SLC44A4.
Clinical progress of SLC44A4-targeted ADCs
NCT01228760 is a Phase I clinical trial aimed at determining the MTD of ASG-5ME in metastatic or non-metastatic CRPC patients. The study is divided into two parts— the first part determines the safe dose of ASG-5ME, and the second part evaluates safety and anti-tumor activity. A total of 46 patients participated in the study. 26 patients were included in the dose escalation group, which was divided into 7 cohorts. Doses ranged from 0.3-3 mg/kg. 20 patients were included in the dose expansion cohort and received 2.4 or 2.7 mg/kg of the study drug. 25% of assessed patients achieved a PSA response, with a decline of >50%. According to RECIST 1.1 criteria, SD and PD were the most common outcomes, while the most common AEs were fatigue and diarrhea. Two deaths occurred during the study.
Trop-2
Trop-2 is a surface transmembrane glycoprotein that is particularly present in prostate cells. The main function of Trop-2 remains unknown; however, according to the literature, it regulates prostate cell self-renewal, intercellular adhesion, and extracellular interactions. In PCa, Trop-2 drives metastatic potential and supports PCa growth by regulating the α5β1 integrin-dependent signaling pathway. Trop-2 is upregulated in >70% of PCa, but its expression is higher in tumors extending beyond the prostate, CRPC, and neuroendocrine cancers.
Clinical progress of Trop-2-targeted ADCs
NCT03725761 is an ongoing Phase II study aimed at determining the safety and efficacy of SG in mCRPC patients who have progressed on next-generation anti-androgens (enzalutamide, apalutamide, or abiraterone acetate). The primary endpoint is the PSA response rate, defined as a PSA decline of ≥ 50% by week 9 of treatment or earlier. Secondary endpoints include radiographic PFS, OS, and toxicity rates. 55 patients will participate in this study.
B7-H3 (CD276)
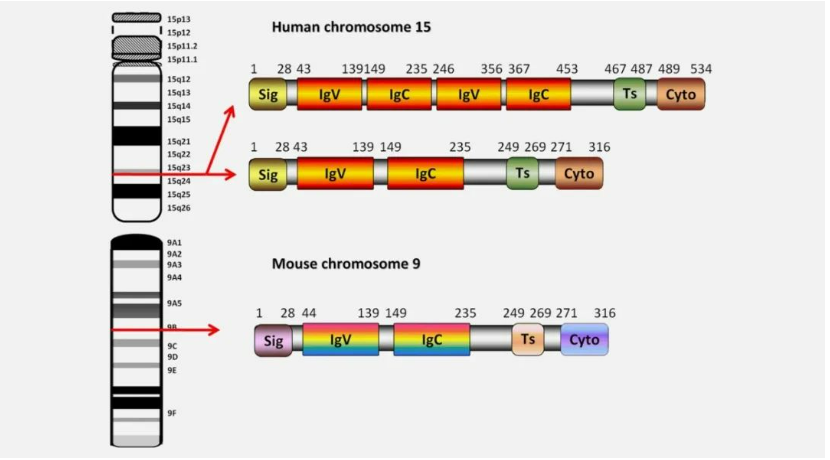
The immune checkpoint molecule B7-H3, also known as CD276, is a membrane protein member of the B7-CD28 family of immunomodulatory proteins and is an I-type membrane protein with a sequence similarity to the extracellular domain of programmed death receptor-1 (PD-L1). In normal human tissues, B7-H3 is expressed at low levels, but it is abnormally overexpressed in various tumor cancers, playing an important role in tumorigenesis, immune evasion, and is associated with poor prognosis in tumors. In PCa, its expression is related to Gleason scores, tumor staging, lymph node metastasis, and castration-resistant disease. Additionally, B7-H3 expression is associated with BRCA2 and ATM mutations in PCa.
Clinical progress of B7-H3-targeted ADCs
MGC018 shows good activity and safety. Common DLTs in the Phase I dose escalation study include neutropenia and fatigue. Dose: 3 mg/kg, Q3W. 55.5% of mCRPC patients in the study achieved a PSA response. Preliminary results of the NCT03729596 Phase I cohort dose expansion study of MGC018 were presented at the recent European Society for Medical Oncology conference, which recruited mCRPC patients after chemotherapy and next-generation hormone therapy; 53.8% achieved PSA response, and PR was 25%.
Commentary
Important targets for targeting prostate cancer (PCa) include: prostate-specific membrane antigen (PSMA), six-transmembrane epithelial antigen 1 (STEAP-1), solute carrier family 44 member 4 (SLC44A4), trophoblast cell surface antigen (Trop-2), and B7-H3.
Although many ADC designs targeting prostate cancer are similar to the currently marketed linkers and payloads, the clinical results have not been particularly impressive, with significant differences even among different antibodies targeting the same antigen.
In the domestic context, validated targets for suitable indications are paramount! Those who blindly criticize FIC are just playing tricks!
References:
[1] Antibody drug conjugate: the “biological missile” for targeted
cancer therapy. Signal Transduction and Targeted Therapy (2022) 7:93
[2] The matrix in cancer. Nat Rev Cancer. 2021 Feb 15. doi: 10.1038/s41568-020-00329-7. Epub ahead of print. PMID: 33589810.
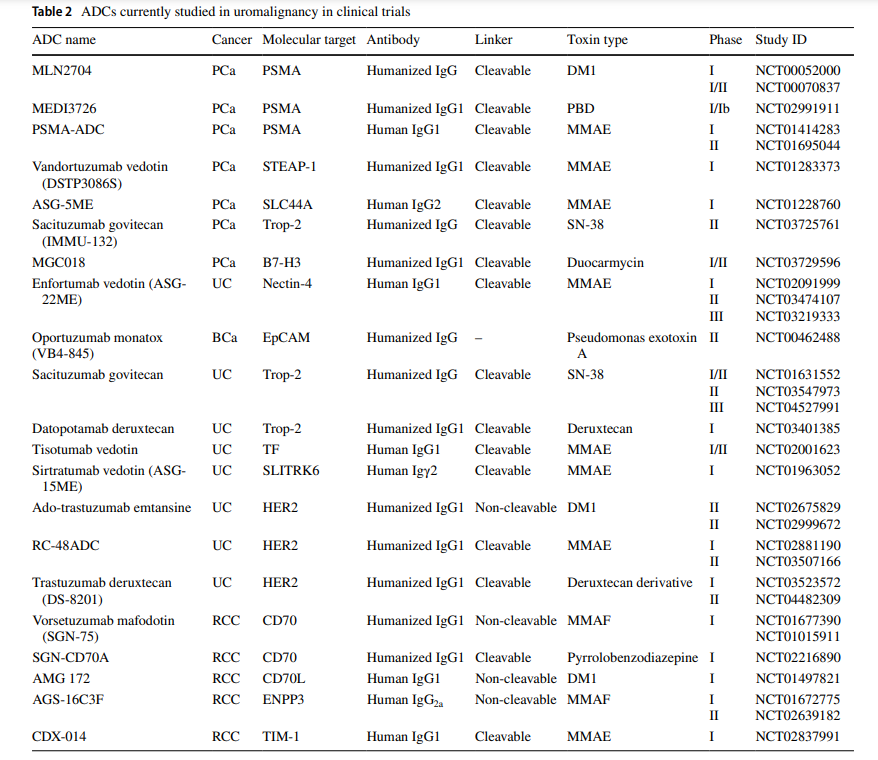
[3] Current status and future prospects of antibody–drug conjugates in urological malignancies. doi: 10.1111/iju.14925
[4] Antibody–Drug Conjugates in Uro‑Oncology. doi.org/10.1007/s11523-022-00872-3
