Mr. Zhao has been suffering from hypertension for over 10 years. In recent years, he has been taking two antihypertensive medications, but sometimes he misses doses, leading to poor blood pressure control. At the pharmacy clinic of Zibo Central Hospital, the pharmacist switched to a single-pill combination preparation using the A+C scheme based on Mr. Zhao’s specific condition. Now, Mr. Zhao only needs to take one pill a day to achieve better blood pressure control.
The 2020 International Society of Hypertension (ISH) guidelines recommend that, except for low-risk stage 1 hypertension, elderly patients (>80 years old), or frail patients, all other hypertensive patients should prioritize combination therapy. It is also recommended to use single-pill combinations (SPC) consisting of two or more antihypertensive medications. SPCs have various combinations, among which the combination of angiotensin-converting enzyme inhibitors (ACEI) / angiotensin receptor blockers (ARB) with calcium channel blockers (CCB) has a synergistic effect on blood pressure reduction. This combined scheme is referred to as A+C in this article and can significantly improve blood pressure control rates. Multiple clinical studies have shown that compared to other combination therapy schemes, the A+C scheme has significant advantages in reducing the incidence of long-term cardiovascular events and protecting target organs related to hypertension. It is the optimal combined antihypertensive scheme recommended by the 2020 ISH guidelines.

1
The Mechanism of A+C Synergistic Antihypertensive Effect

ACEI/ARB mainly exert their effects through two pathways in the renin-angiotensin-aldosterone system (RAAS), acting on angiotensin-converting enzyme (ACE) and ACE2.
In the classical ACE-angiotensin II (Ang II)-angiotensin receptor (mainly type 1 receptor, AT1R) pathway, ACEI/ARB inhibit the generation of active Ang II (or block Ang II from binding to AT1R), causing relaxation of vascular smooth muscle cells and endothelial cells, and inhibiting the release of catecholamines from the adrenal medulla and aldosterone from the adrenal cortex, thereby dilating the arteries and veins and reducing sodium and water retention, resulting in a blood pressure-lowering effect. Additionally, ACEI can inhibit the degradation of vasodilatory bradykinin.
In the ACE2 pathway, both ACEI and ARB can activate ACE2 to convert Ang II into angiotensin (1-7) [Ang (1-7)], promoting renal artery vasodilation, activating endothelial nitric oxide synthase (eNOS) in endothelial cells, and inducing diuresis, thereby exerting an antihypertensive effect.
On the other hand, CCBs block the L-type calcium channels, reducing the influx of extracellular Ca2+ into cells, lowering intracellular Ca2+ concentration, relaxing vascular smooth muscle, dilating arteries, and lowering blood pressure.
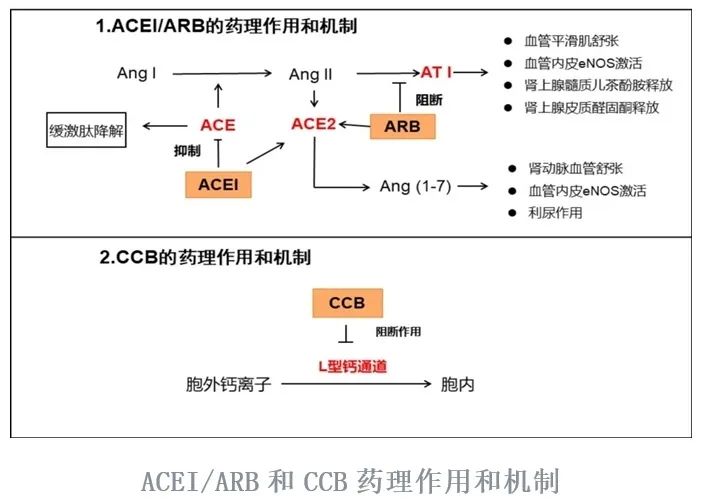
ACEI/ARB combined with CCB has a complementary mechanism of action that enhances the antihypertensive effect and can mutually offset or alleviate adverse reactions. The reflex activation of RAAS by CCB can be inhibited by ACEI/ARB, and ACEI/ARB can alleviate peripheral edema induced by CCB by dilating peripheral venous blood vessels. Adverse effects such as vascular edema and dry cough caused by ACEI can be partially alleviated by CCB.
2
ACEI/CCB and ARB/CCB
SPC Selection Criteria
The selection of A+C SPC is mainly based on the specific comorbidities of hypertensive patients and the contraindications of the medications. Dihydropyridine CCBs have no absolute contraindications, but when selecting A+C SPC, special attention should be paid to the contraindications of ACEI/ARB.
Contraindicated populations include: ① Those allergic to CCB or ACEI; ② Those who have had adverse reactions to CCB or ACEI, especially those who experienced significant cough or angioedema due to ACEI; ③ Acute congestive heart failure; ④ Hyperkalemia; ⑤ Severe renal failure [estimated glomerular filtration rate (eGFR)<30 mL/(min·1.73m2)]; ⑥ Pregnant or breastfeeding; ⑦ Bilateral renal artery stenosis.
Precautionary populations include: ① Rapid arrhythmias; ② Heart failure; ③ Severe leg edema.
Timing of selection: It is recommended to initiate A+C SPC for high-risk patients whose blood pressure exceeds the control target by 20/10 mmHg or for hypertensive patients who have not achieved targets with monotherapy.
3
ACEI/ARB Combined with CCB
Recommendations for SPC Use
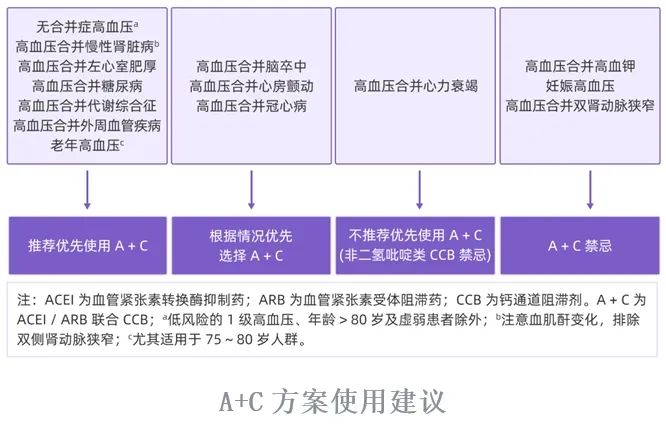
➤Hypertensive patients without comorbidities
(1) For hypertensive patients without comorbidities whose blood pressure exceeds the target value by more than 20/10 mmHg or who have not achieved targets with monotherapy, A+C SPC treatment is recommended as the first choice.
(2) Excluding low-risk stage 1 hypertension, patients over 80 years of age, and frail patients, other patients with blood pressure >140/90 mmHg may also consider low-dose A+C SPC treatment.
➤Hypertension with Chronic Kidney Disease (CKD)
In the combined antihypertensive treatment for hypertension with CKD, A+C or A+D is usually chosen. For hypertensive patients with CKD, when combination therapy is needed, it is recommended to prioritize A+C SPC treatment [excluding eGFR<15 mL/(min·1.73 m2)]. It is also suggested that adult patients with hypertension and CKD should control systolic blood pressure to <120 mmHg if tolerated.
➤Hypertension with Left Ventricular Hypertrophy
For patients with hypertension and left ventricular hypertrophy, A+C SPC is recommended as the first choice for combination therapy.
➤Hypertension with Coronary Heart Disease
For such patients with angina, the A+C scheme can be one of the preferred options. Furthermore, if these patients have not achieved ideal blood pressure control after using ACEI/ARB + β-blockers or have contraindications to β-blockers, the addition of long-acting CCB should be considered.
➤Hypertension with Heart Failure
For patients with hypertension and heart failure, if blood pressure remains uncontrolled after using ACEI/ARB, diuretics, β-blockers, and SGLT2 inhibitors, the combined use of dihydropyridine CCB (recommended amlodipine, felodipine; not recommended nifedipine) should be considered to control blood pressure, or sacubitril/valsartan can be recommended as a replacement for ACEI/ARB treatment.
➤Hypertension with Atrial Fibrillation
The A+C scheme can be one of the preferred options for blood pressure control in patients with hypertension and atrial fibrillation. However, dihydropyridine CCBs have poor rhythm control effects (weaker than β-blockers), and when rhythm control is involved, other medications should be added based on specific circumstances.
➤Hypertension with History of Stroke
For patients with hypertension and a history of stroke, the A+C scheme can be one of the preferred options.
➤Hypertension with Diabetes
In the treatment of hypertension with diabetes, the A+C scheme is recommended as the first choice.
➤Hypertension with Metabolic Syndrome
A+C SPC has protective effects against cardiovascular disease risks and target organ damage, thus it is recommended for hypertensive patients with metabolic syndrome to prioritize A+C SPC.
➤Hypertension with Peripheral Artery Disease (PAD)
ACEI/ARB and CCB can improve endothelial function in diseased vessels while lowering blood pressure, so it is recommended for hypertensive patients with PAD to prioritize A+C SPC.
➤Hypertension in Elderly Patients
It is recommended that elderly hypertensive patients prioritize A+C SPC.
The A+C scheme has many advantages, including good antihypertensive efficacy, fewer adverse reactions, improved prognosis, and protection of target organs. SPC can enhance medication adherence and blood pressure target achievement rates. As the advantages of combination therapy, intensified therapy, and SPC become increasingly evident, the rational use of the A+C combination SPC will make significant contributions to improving blood pressure control rates and target achievement rates in China.
Source: Hypertension Science Popularization Studio, Pharmacy Department Zhan Ying
Editor: Chen Yuan
Review: Publicity Department

 Share
Share Like
Like View
View