Antibody-drug conjugates (ADCs) have emerged as a significant platform for precision oncology, demonstrating remarkable efficacy in various solid tumors in recent years. With ongoing innovations in target selection and linker technology, the development of ADCs for the treatment of metastatic castration-resistant prostate cancer (mCRPC) has also made significant strides. This article systematically reviews the latest research advancements of ADC technology in prostate cancer treatment, based on a recent review published in npj Precision Oncology.
Mechanism of Action and Payload Innovations of ADCs
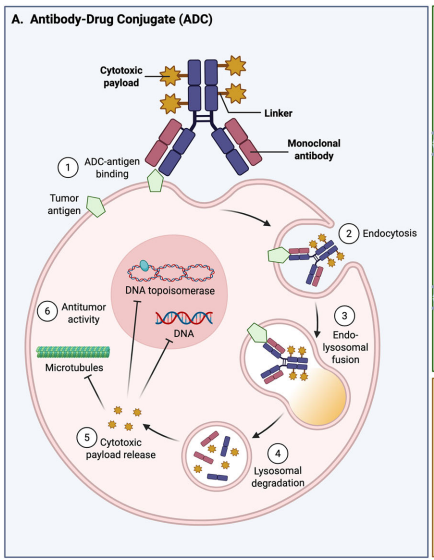
ADCs specifically target tumor cell surface antigens through monoclonal antibodies, coupled with highly potent cytotoxic payloads, to achieve precise killing of cancer cells. Their mechanism of action involves multiple steps, including antigen binding, endocytosis, lysosomal degradation, and payload release.
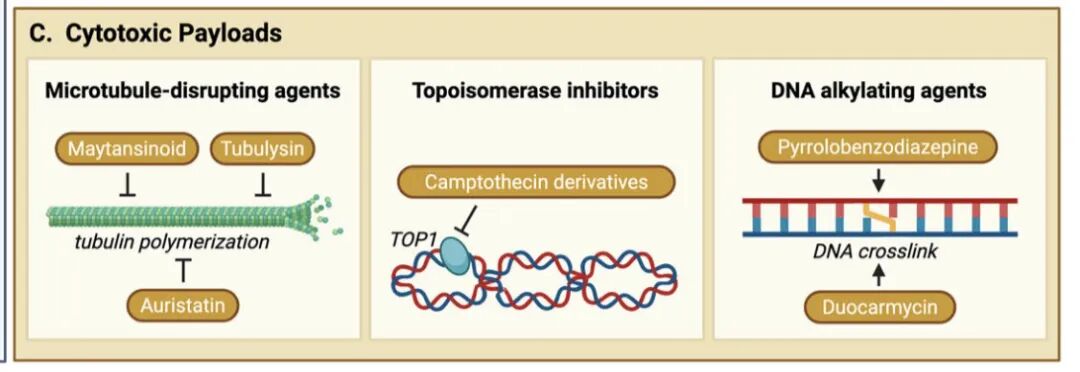
Currently, ADC payloads are primarily categorized into three major classes: microtubule inhibitors (auristatins, maytansinoids, tubulysins), topoisomerase I inhibitors (irinotecan, topotecan, exatecan, deruxtecan), and DNA alkylators (PBD dimers, duocarmycins). Notably, topoisomerase I inhibitors induce DNA single-strand breaks by forming stable complexes with DNA topoisomerase I, which may have particular efficacy in mCRPC patients with homologous recombination repair defects (such as BRCA1/2 mutations).
Innovations in linker technology are equally critical. Cleavable linkers (such as hydrazone, disulfide, peptide bonds, etc.) release payloads specifically in the tumor microenvironment, while non-cleavable linkers rely on complete antibody degradation for release, each having its pharmacokinetic advantages. New linker designs aim to balance circulation stability and tumor release efficiency to optimize the therapeutic window.
Key Targets for Prostate Cancer ADCs
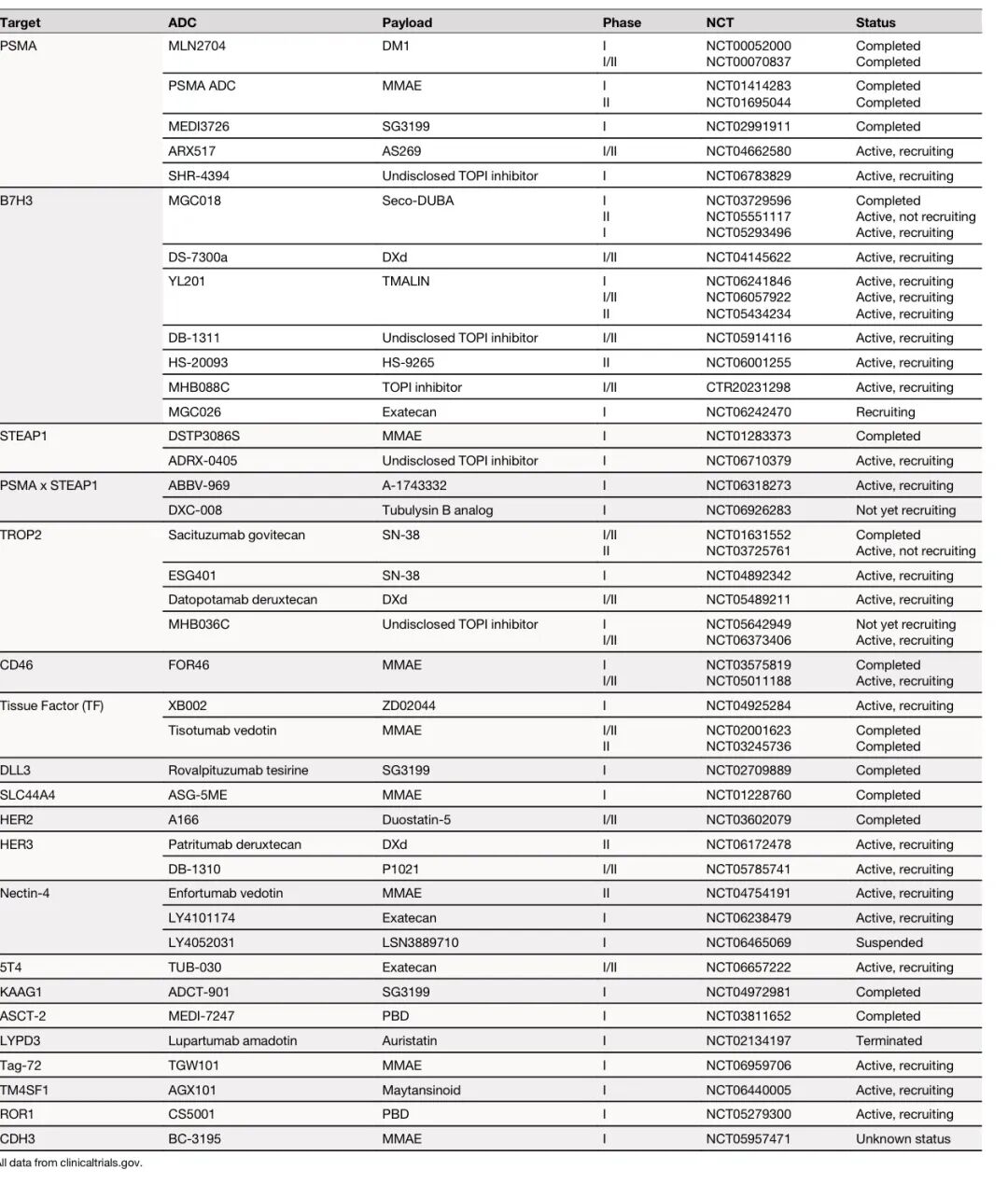
PSMA-targeted ADCs
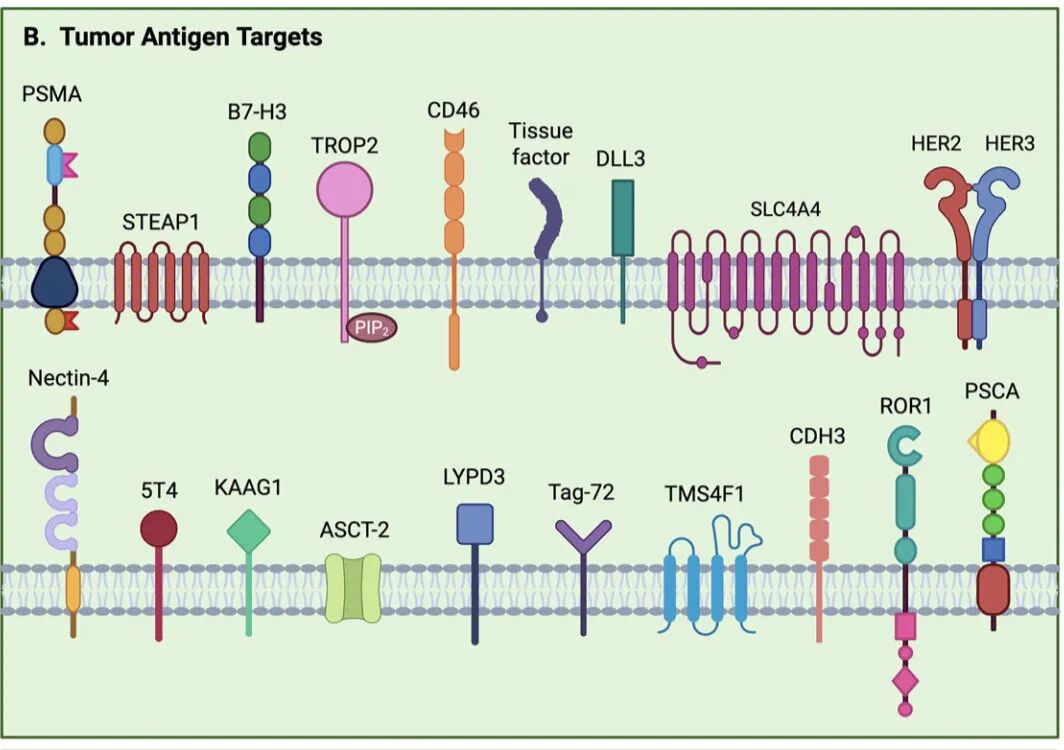
Prostate-specific membrane antigen (PSMA) is upregulated in mCRPC and is the most extensively studied target to date. Early ADCs such as MLN2704 (DM1 payload) and PSMA ADC (MMAE payload) showed initial anti-tumor activity but were limited in clinical application due to dose-limiting toxicities such as neurotoxicity caused by unstable linkers.
The next-generation PSMA-targeted ADC ARX517 employs a novel non-cleavable linker technology, demonstrating good safety in the phase I APEX-01 study, with some patients in the 2.8 mg/kg dose group achieving PSA50 responses and soft tissue lesion shrinkage. Its expanded cohort study (NCT04662580) is currently ongoing.
B7-H3-targeted ADCs
B7-H3 overexpression in prostate cancer is associated with tumor metastasis, invasion, and poor prognosis. Vobramitamab duocarmazine (MGC018) showed anti-tumor activity in phase I studies, but further development was halted due to toxicity issues.
Ifinatamab deruxtecan (I-DXd, DS-7300) utilizes the Deruxtecan payload, achieving an objective response rate of 25% in mCRPC patients, with a median progression-free survival of 4.8 months. Additionally, novel B7-H3-targeted ADCs such as YL201 and DB-1311 have shown preliminary efficacy and are currently in early clinical development.
STEAP1-targeted ADCs
Six-transmembrane epithelial antigen of the prostate 1 (STEAP1) is overexpressed in 90% of prostate cancers and remains expressed in PSMA-negative tumors, making it an important supplementary target. The phase I study of Vandortuzumab vedotin (DSTP3086S) showed an 18% PSA50 response rate, but further development was discontinued.
Currently, bispecific ADCs are emerging as a new direction, with ABBV-969 (PSMA×STEAP1 dual-target) and DXC-008 (tubulysin B payload) entering clinical research stages, promising to overcome resistance issues caused by tumor heterogeneity.
Other Emerging Targets
TROP2: Sacituzumab govitecan and Datopotamab deruxtecan are being studied in mCRPC, with preliminary data showing some efficacy.
CD46: FOR46 combined with enzalutamide showed synergistic effects in a phase Ib study, with 41.2% of patients achieving long-term disease stability.
Tissue factor (TF): XB002 and Tisotumab vedotin have validated feasibility in solid tumors, with exploration ongoing for prostate cancer indications.
DLL3: Upregulated in neuroendocrine differentiated prostate cancer, Rova-T was discontinued due to toxicity issues, but new mechanisms such as bispecific T cell engagers are still under development.
Clinical Challenges and Future Directions
The clinical application of ADCs in prostate cancer still faces multiple challenges: the high density of tumor stroma and sparse vascular distribution limit ADC penetration; target expression heterogeneity affects efficacy; and resistance mechanisms to payloads (such as microtubule mutations and topoisomerase mutations) may lead to cross-resistance.
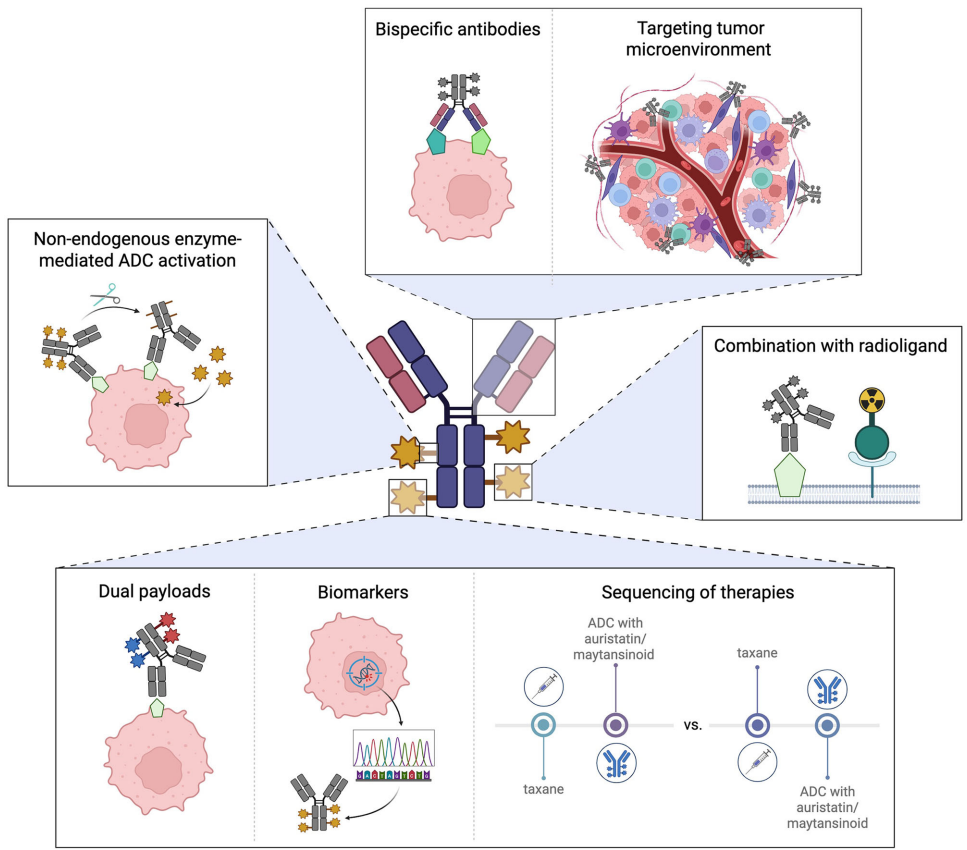
Future development directions include: bispecific ADCs (such as PSMA×B7-H3 dual-target GenSci143), dual payload ADCs (delivering different mechanism cytotoxic drugs simultaneously), tumor microenvironment targeting (such as targeting cancer-associated fibroblasts), and combination therapy strategies (such as sequential use with PARP inhibitors or 177Lu-PSMA-617).
Biomarker-guided patient selection is also crucial. Techniques such as PSMA-PET and STEAP1 imaging help screen advantageous populations; molecular features like HRD status and SLFN11 expression may predict the efficacy of topoisomerase inhibitors; and the discovery of correlations between RB1/TP53 deletions and B7-H3 ADC efficacy marks a move towards precision ADC therapy.
Conclusion
ADCs offer new possibilities for mCRPC patients. With increasing target diversity, optimized linker technologies, and expanded payload mechanisms, ADCs are expected to play a role in prostate cancer treatment. Future efforts will require more refined patient stratification and more rational combination strategies to maximize the clinical benefits of ADCs.
______
References: Lin C, Hadfield MJ, Santopietro A, et al. The evolving landscape of antibody-drug conjugates (ADCs) for treatment of prostate cancer. npj Precis Oncol. 2025;9:351. doi:10.1038/s41698-025-01131-0