Recently, the ADC (Antibody-Drug Conjugate) conference has been held one after another, with major biotech companies competing to report their ADC pipelines. It is expected that 2024 will still be the main stage for ADCs.
Developing an entry-level ADC seems not too difficult, but how to evaluate the pharmacology and toxicology in the preclinical stage has become a top priority.
Although the experience of monoclonal antibodies can be referenced, given the unique aspects of ADCs, there are many challenges in the development and evaluation of ADCs. The difference between ADCs and naked monoclonal antibodies is that ADCs must bind to and internalize into tumor cells, thereby transporting and releasing small molecule drugs inside the cells. The antibody, small molecule drug, linker, and the methodology of linkage may all affect the ADCs’ efficacy and safety.
Currently, there are many in vivo and in vitro non-clinical research methods, and there is also development experience from marketed drugs, but predicting clinical efficacy and safety through optimized non-clinical research remains a challenge, and this article conducts an in-depth analysis on this.
01
The Development History of ADCs
Ideal ADCs should possess at least the following three characteristics:
1. Targeting ability: The ideal ADC target should have the antigen expressed only on the surface of the tumor; it should also be expressed at a high level and not easily shed.
2. Translocation process: Before reaching the target cells, the cytotoxic molecules should shed as little as possible, meaning the complete ADC should be internalized into the cells.
3. Release of the small molecule toxin: The small molecules should be released rapidly and in large quantities only inside tumor cells; the small molecules should have high toxicity to effectively kill tumor cells. Based on these characteristics, ADCs have undergone several stages of evolution (see Figure 1).
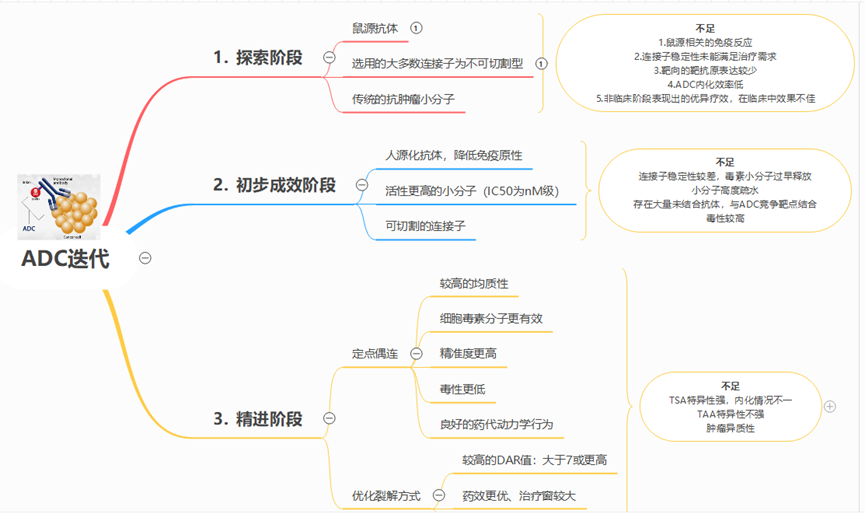
Figure 1 Iteration and Evolution of ADCs
02
Pharmacological Evaluation Strategies for ADCs
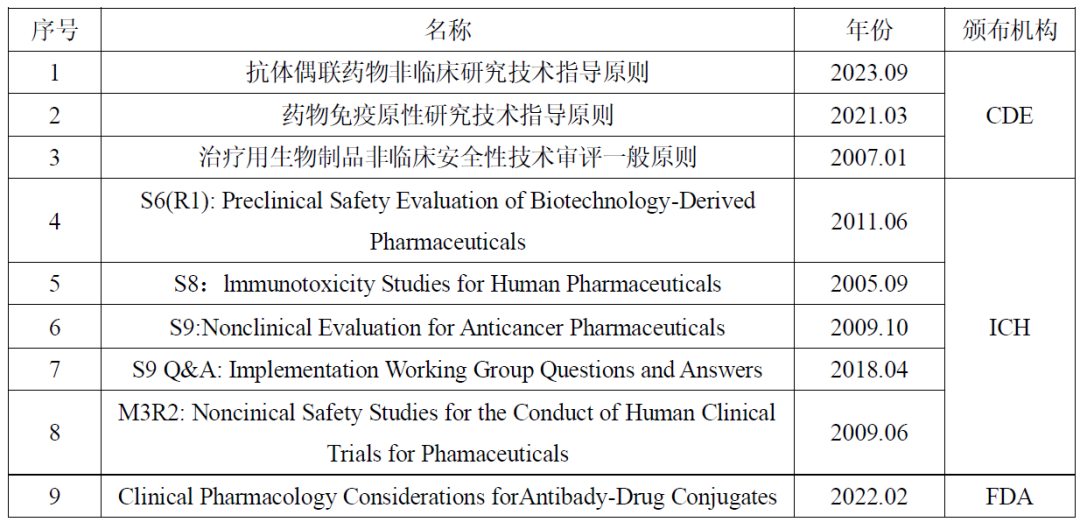
Table 1: Common Guidelines for Non-Clinical Evaluation of ADCs
The study of pharmacological effects usually focuses on the drug discovery or non-clinical evaluation phase, and the main experimental projects that need to be conducted include: target binding activity, antibody-mediated internalization, in vivo and in vitro tumor proliferation inhibition (for anti-tumor ADCs), antibody-dependent cellular cytotoxicity (ADCC), and complement-dependent cytotoxicity (CDC).
In the experiments, attention should be paid to the pharmacological differences between ADCs and naked monoclonal antibodies, as well as non-conjugated cytotoxic drugs. In vitro target binding studies play an important role in the optimization of linker/linkage methods in the early stages of drug research, and in the selection of relevant animal species for in vivo administration tests. In early drug optimization screening, attention should be paid to the internalization of ADCs, as the expression level of the target antigen and the heterogeneity of ADCs may affect the internalization of ADCs.
Typically, immunofluorescence techniques are used to observe the internalization of ADCs in cells and their interaction with lysosomes.
In pharmacological studies, it is also necessary to consider the effects of ADCC and CDC. The absence of functional effects may have advantages to some extent, as the binding of ADCs to effector cells may reduce their accumulation at tumor sites, hinder their internalization, and produce normal cytotoxicity. Efficacy studies conducted at the cellular level or in animal models are the most direct reflection of the pharmacological effects of ADCs.
The expression level of the target antigen is a factor that needs to be considered in in vitro or in vivo efficacy tests. In tumor therapy, even if the target antigen is tumor-associated, if the expression level is not high, it may affect the binding and internalization of ADCs with the target antigen, thereby affecting the targeted delivery and release of cytotoxic drugs. The expression level of the target antigen is significantly related to clinical efficacy. The FDA-approved Kadcyla significantly improves the progression-free survival and overall survival of patients with high expression of Her2 in breast cancer, with the progression-free survival (PFS) of high-expression patients being 10.6 months, while that of low-expression patients is 8.2 months. The overall survival of the high-expression group is 34.1 months, while that of the low-expression group is 26.5 months.
Typically, immunohistochemistry is used to confirm the expression level of target antigens in tumor cells or normal cells; however, immunohistochemistry has the drawback of being difficult to predict immune responses under physiological conditions. Biodistribution or whole-body imaging tests in animal models can provide a comprehensive and intuitive understanding of the expression of target antigens throughout the body, the binding and internalization of ADCs with antigens, and the distribution ratio of tumor tissues to other tissues.
When investigating the efficacy of ADCs in animals, the species difference must first be considered. If ADCs do not have binding activity or have low binding activity with the antigens of mice, it may be necessary to consider using transgenic animals for efficacy testing or using animal-derived antibodies to conduct in vivo efficacy studies. Transgenic animals can avoid the use of surrogate antibodies, and for the expression of target antigens in the host vasculature or stroma, transgenic animals can not only investigate the efficacy but also observe toxic reactions to a certain extent. If the target antigen is only expressed in human tumor cells, transgenic animals are not needed, and efficacy can be investigated in nude mouse models inoculated with human tumor cells. When conducting efficacy studies at the cellular level or in animal models, it is also important to conduct PK/PD studies, analyze drug targeting distribution, receptor occupancy, and the relationship between drug exposure and effects, which will help in the design of clinical dosing regimens and the analysis of safety study results.
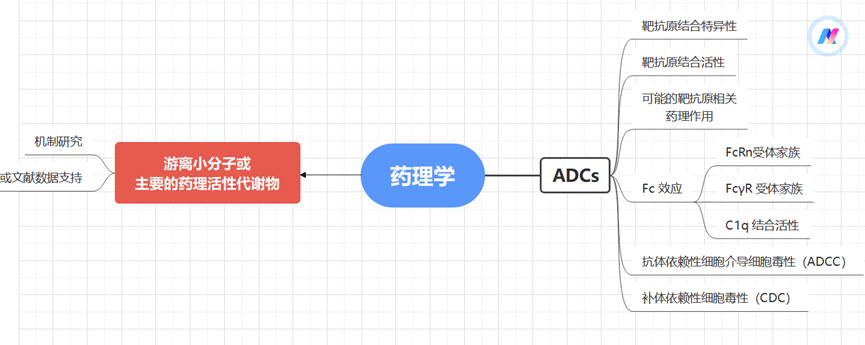
Figure 2 Pharmacological Evaluation Strategies for ADCs
03
Toxicological Evaluation Strategies for ADCs
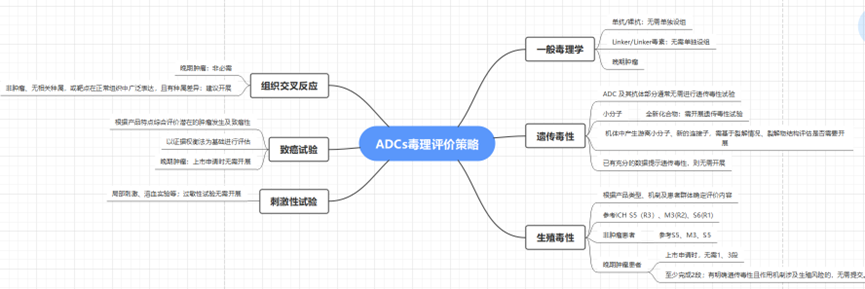
Figure 3 Non-Clinical Evaluation Strategies for ADCs
Selection of Animal Species: In order to fully expose the toxic characteristics of ADCs in non-clinical safety studies to support clinical development of ADCs, it is crucial to evaluate the relevance of the animal trial species and the translatability of non-clinical research results. This assessment typically involves examining the binding affinity of ADCs to target antigens in non-clinical species relative to humans, as well as comparing immunohistochemical staining profiles in tissue cross-reactivity studies. The effector function or immunogenicity of antibodies may also vary due to species differences.
Exposure Parameters and Metabolism: Additionally, like other drugs and biological products, the extrapolation of non-clinical research results to humans should include comparisons of exposure parameters and metabolism. For example, BR-96, an ADC covalently linked to the humanized BR96 monoclonal antibody’s cysteine residue via a 6-maleimidocaproic acid hydrazone linker, showed that the toxicity of BR-96 in dogs is more sensitive than in rats and monkeys, with the toxic effects of hemorrhagic enteritis serving as dose-limiting toxicity. Surprisingly, BR96-DOX and the unmodified monoclonal antibody BR96 exhibited the same dose-limiting toxicity, indicating that the toxicity is produced by the monoclonal antibody. Unlike unconjugated DOX, ADCs did not induce cardiomyopathy in rat models. Therefore, the dose selection for the Phase I clinical trial of BR96-Dox in human subjects was based on the toxicological results in dogs.
Expression of Antibody Targets: Similar to therapeutic monoclonal antibodies, the non-clinical evaluation of ADCs may be hindered by the lack of antigen targets in animal trial species. The guidelines from ICH S6 (R1) regarding the preclinical safety evaluation of biotechnological-derived drugs (2011) state that “the species selection for antibody-drug/toxin conjugates (ADCs) containing novel toxins/toxicants should follow the same general principles as those for unconjugated antibodies. The relevant animal species for monoclonal antibody testing are those that express the epitopes required for antibody and show a tissue cross-reactivity profile similar to that of human tissue.” Therefore, species and disease specificity may determine or limit non-clinical evaluation.
One example is Polatuzumab vedotin, which binds to CD79b on human B cells, but was found not to bind to CD79b in mice, rats, or cynomolgus monkeys, lacking pharmacologically relevant non-clinical species. Non-clinical toxicity studies used surrogate ADCs that bind to CD79b in cynomolgus monkeys with affinities similar to Polatuzumab vedotin and human CD79b, which is another method described in the ICH S6 (R1) guidelines for the non-clinical safety evaluation of biological products. The surrogate antibody-drug conjugate (ADC) used the same linker-drug as Polatuzumab vedotin, namely the microtubule inhibitor monomethyl auristatin E (MMAE), linked by a cleavable dipeptide valine-citrulline (vc) linker, and the average DAR value of the vc-MMAE molecule binding to the anti-CD79b monoclonal antibody (mAb) is similar, but the surrogate antibody differs from the clinical antibody in that it is a chimeric structure with non-humanized (mouse) complementarity-determining regions.
When using surrogate antibodies, it is important to adequately characterize the surrogates used for ADC safety evaluations (e.g., epitope binding, activity and potency, and PK).
Another example of a humanized ADC is Anetumab-ravtansine, which is a humanized anti-mesothelin antibody conjugated to DM4 (a maytansinoid microtubule inhibitor), showing effective cytotoxic effects on tumor cells expressing mesothelin. Since the ADC binds only to human mesothelin, target-mediated toxicity cannot be studied in non-clinical animal models; however, off-target toxicities unrelated to the antigen were evaluated in rats and cynomolgus monkeys. It is believed that the toxicity observed in humans may be related to the physiological expression of mesothelin in healthy tissues, limiting the maximum tolerated dose in clinical trials to below that predicted by non-clinical studies.
The expression of target antigens in normal tissues is a major safety concern for ADC therapy. Ideally, the expression of target antigens on normal cells should be very low; however, as seen in the two examples above, antibodies do not behave this way in practice. Other potential toxicities related to the lack of specificity of ADC targets include NaPi2b, a sodium-dependent phosphate transporter expressed in several tumor types but also detectable in normal tissues, playing a role in inorganic phosphate homeostasis. An ADC (anti-NaPi2b-vc-MMAE) was confirmed to have specific binding affinity by a humanized IgG1 anti-NaPi2b monoclonal antibody conjugated to MMAE via a vc peptide linker in normal human and cynomolgus monkey tissues. However, despite high-level expression in the normal lungs of monkeys, the safety of this cross-reaction can be accepted, with dose-limiting toxicity unrelated to normal tissue expression. In normal rats, non-binding species, and monkeys, the toxicological effects are consistent with the pharmacology of MMAE.
General Toxicology Design Principles: Generally, monoclonal antibodies/naked antibodies, Linker/Linker-toxin do not usually require separate groups; the monoclonal antibody molecule is one of the main factors affecting or determining systemic exposure, and dose design should comprehensively consider the pharmacological doses of ADCs, the characteristics of the antibody molecule, and the toxicity characteristics of small molecule toxins.
Focus on Payload-Related Toxicity: Although targeted release of small molecular compounds achieves drug enrichment in targeted tissues and improves the therapeutic window, the main toxic reactions of ADCs still resemble the toxicity characteristics of the connected small molecular compounds. Most ADCs exhibit a weaker degree of toxicity compared to direct administration of small molecular compounds, but some ADCs may increase tissue toxic reactions from antibody target binding or off-target binding. Although ADCs enhance the targeted release of small molecular compounds, some small molecular compounds can still be released prematurely, and some free small molecular compounds can also rapidly diffuse from target cells to surrounding tissues or systemic circulation, or the apoptosis or damage of target cells may lead to the entry of free small molecular compounds into systemic circulation. The antibody portion in ADCs may also bind to surface receptors or antigen epitopes on other non-target tissues or organs, for example, through Fc receptor-mediated phagocytosis, and the drug may have toxic effects on corresponding tissue cells after metabolic breakdown. Therefore, the toxicity of ADCs is closely related to the characteristics of the antibody, small molecular compounds, and linkers, and as the antibody, small molecular compounds, and linkers change, their toxicity response characteristics will also change. In non-clinical safety studies, attention should be paid to the influence of drug composition structure and pharmacokinetic characteristics on toxic effects, and comprehensive analysis of experimental results.
Genotoxicity: Biological macromolecules generally do not directly interact with DNA, and the ADC and its antibody portions usually do not require genotoxicity testing. The potential genotoxicity of ADCs comes from the small molecular compounds. If the payload small molecular compounds are novel compounds, genotoxicity testing should be conducted; for new free small molecular compounds and/or new linkers produced in the body, the need for relevant genotoxicity studies should be assessed based on the physicochemical properties, degradation characteristics, and structural factors of the ADC; if sufficient data indicate that the target detection substance has genotoxicity, there is no need to conduct genotoxicity studies.
Reproductive Toxicity: The small molecular compounds, linkers, and naked antibodies in ADCs may adversely affect reproductive organs, fertility, embryo-fetal development, and offspring development, thus attention should be paid to the reproductive toxicity risks of ADCs. The research strategies, experimental designs, implementation, and evaluation of reproductive toxicity of ADCs should refer to ICH S5 guidelines, while considering the mechanism of action of the ADC and the patient population, adopting a specific analysis strategy for specific issues. ADCs intended for patients with advanced tumors may refer to ICH S9 guidelines for reproductive toxicity studies.
For biological products, reproductive toxicity is usually evaluated in pharmacologically relevant animal species. If rodents and rabbits are both target-binding related animal species, two animal species should be used for embryo-fetal development toxicity tests, unless embryonic lethality or teratogenicity has already been confirmed in one species. If the target-binding animal species are non-human primates or there are no relevant animal species, it is generally considered to first use rats or rabbits to conduct reproductive toxicity tests, investigating the reproductive toxicity of free small molecular compounds. If the research results confirm positivity, there is no need to further investigate reproductive toxicity in target-binding related animal species; otherwise, it may be necessary to consider using non-human primates or transgenic animals or surrogate molecules to identify antigen-mediated reproductive toxicity. If the antibody or small molecular compounds in the ADC have literature data clearly indicating potential reproductive toxicity risks, there is no need to conduct reproductive toxicity studies, and relevant risk control can be based on the literature information.
Carcinogenicity: The necessity of carcinogenicity studies can be considered based on the characteristics of ADCs, following relevant guidelines such as ICH S1, ICH S6, and ICH S9.
Immunogenicity/Immunotoxicity: After ADCs enter the biological system, they may cause immunogenicity and produce anti-drug antibodies. Evaluating the immunogenicity of ADCs helps analyze the pharmacokinetics, efficacy, and safety results of the drug; therefore, it is usually necessary to conduct anti-drug antibody testing in non-clinical safety studies of ADCs. Anti-drug antibodies may arise from the antibody portion and linker portion in ADCs, and based on immunogenicity risks, it should be considered whether further investigation of antigen epitopes is needed. The development, validation, and analytical detection strategies for the methodology of immunogenicity analysis of ADCs should follow the “Technical Guidance for Immunogenicity Studies of Drugs”. Relevant guidelines such as ICH S6, ICH S8, and ICH S9 should be referenced, combining factors such as the type and mechanism of action of ADCs to reasonably design immunotoxicity detection indicators. In addition to routine immunotoxicity studies, additional immunotoxicity studies should be considered if necessary.
Phototoxicity: Before Phase I clinical trials, a preliminary assessment of potential phototoxicity should be conducted based on the photochemical properties of small molecular compounds (including linkers) and the pharmacological/chemical categories. If these data assessments indicate potential risks, appropriate protective measures should be taken for clinical trial subjects. If the phototoxicity risk cannot be adequately evaluated based on non-clinical data or clinical experience, a phototoxicity assessment following the principles described in ICH S10 should be provided before clinical trials involving a large sample size (Phase III).
Tissue Cross-Reactivity: Tissue cross-reactivity studies are in vitro tissue binding tests using immunohistochemical techniques to determine the binding characteristics of antibodies and antigen epitopes in tissues. Tissue cross-reactivity studies can provide useful supplementary information for understanding target distribution and also provide information on potential unintended bindings. Studies using human tissues for tissue cross-reactivity are an integral part of the initial safety evaluation series for antibody-based drugs. When there are no target-binding related animal species, tissue cross-reactivity information is particularly important for predicting human toxicity risks. For ADCs intended for advanced tumor indications, relevant animal species can be used to evaluate toxicological effects, and when there are no special concerns, tissue cross-reactivity studies are not necessary.
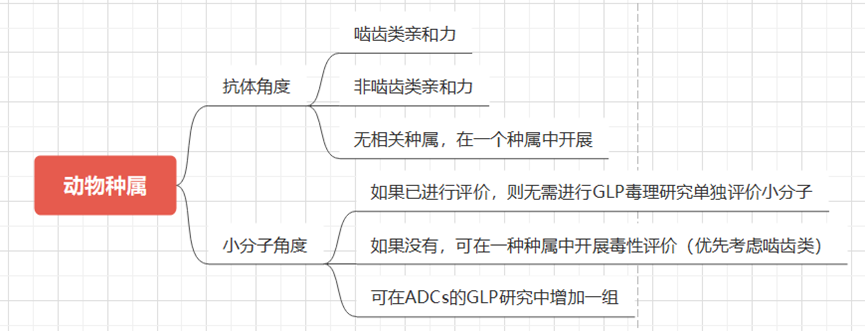
Figure 4 Strategy for Selecting Animal Species
04
Conclusion
Currently, the non-clinical pharmacology and toxicology research of ADCs has relevant technical guidelines issued by ICH, FDA, NMPA, etc. In research, ADCs can also refer to guidelines such as ICH S6 and ICH S9, while designing scientifically reasonable non-clinical pharmacology and toxicology studies based on drug characteristics, maximizing the extrapolation of non-clinical animal level efficacy and toxicity responses to humans, predicting the efficacy and safety of ADCs in clinical applications, thereby improving the success rate of clinical trials and reducing development risks. New drug developers can communicate with review agencies regarding preliminary research results and existing issues to obtain scientifically standardized non-clinical research support information.
References:
Technical Guidance for Non-Clinical Research of Antibody-Drug Conjugates. (NMPA, September 25, 2023)
Fisher JE Jr. Considerations for the Nonclinical Safety Evaluation of Antibody-Drug Conjugates. Antibodies (Basel). 2021 Apr 19;10(2):15. doi: 10.3390/antib10020015. PMID: 33921632; PMCID: PMC8167597.
Yan Liping, Wang Haixue, Wang Qingli. Key Considerations for Non-Clinical Pharmacology and Toxicology Research of Anti-Tumor Antibody-Drug Conjugates. China New Drug Journal, 2017, 26(16):1894-1899.
-
Some materials referenced the ADC non-clinical evaluation strategy lecture (Tang Naping, January 24, 2024)
Scan the WeChat QR code to add the editor of the Antibody Circle,those who meet the conditions can join the Antibody Circle WeChat group!Please indicate: Name + Research Direction!
 This public account’s reprinted articles are intended to convey more information and clearly indicate the source and author. Media or individuals who do not wish to be reprinted can contact us ([email protected]), and we will immediately delete them. All articles represent the author’s views and do not represent the position of this site.
This public account’s reprinted articles are intended to convey more information and clearly indicate the source and author. Media or individuals who do not wish to be reprinted can contact us ([email protected]), and we will immediately delete them. All articles represent the author’s views and do not represent the position of this site.