Click the “Chinese Practical Surgery Journal” above to subscribe!

[Cite this article] National Health Commission of the People’s Republic of China. Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition) [J]. Chinese Practical Surgery Journal, 2022, 42(3): 241-273.
Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition)
National Health Commission of the People’s Republic of China
Chinese Practical Surgery Journal, 2022, 42(3): 241-273
1 Overview
Primary liver cancer is currently the 4th most common malignant tumor and the 2nd leading cause of cancer death in China, posing a serious threat to the life and health of the Chinese people. Primary liver cancer mainly includes three different pathological types: hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and combined hepatocellular-cholangiocarcinoma (cHCC-CCA). The three types differ significantly in terms of pathogenesis, biological behavior, histopathology, treatment methods, and prognosis, with HCC accounting for 75%-85% and ICC accounting for 10%-15%. In this guideline, “liver cancer” refers only to HCC.
To further standardize the diagnosis and treatment of liver cancer in China, the former National Health and Family Planning Commission announced the “Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2017 Edition)” in June 2017, which was updated by the National Health Commission in December 2019. The “Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2019 Edition)” reflected the state of liver cancer diagnosis, multidisciplinary comprehensive treatment, and research at that time, playing an important role in standardizing the diagnosis and treatment of liver cancer, improving the prognosis of liver cancer patients, ensuring medical quality and safety, and optimizing medical resources. Since the release of the “Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2019 Edition)”, many high-level evidences conforming to the principles of evidence-based medicine have emerged in the diagnosis, staging, and treatment of liver cancer, especially research results suitable for the Chinese context. Therefore, the National Health Commission entrusted the Oncology Branch of the Chinese Medical Association to work with the Liver Cancer Professional Committee of the Chinese Anti-Cancer Association, the Ultrasound Medicine Branch of the Chinese Medical Association, the Surgical Physician Branch of the Chinese Physician Association, and the Interventional Physician Branch of the Chinese Physician Association to organize multidisciplinary experts in the field of liver cancer nationwide, combining the latest practices in clinical diagnosis, treatment, and research of liver cancer, to revise and update the “Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition)”. This aims to promote the implementation of the goal of increasing the overall 5-year survival rate of malignant tumors by 15% in the “Healthy China 2030” planning outline.
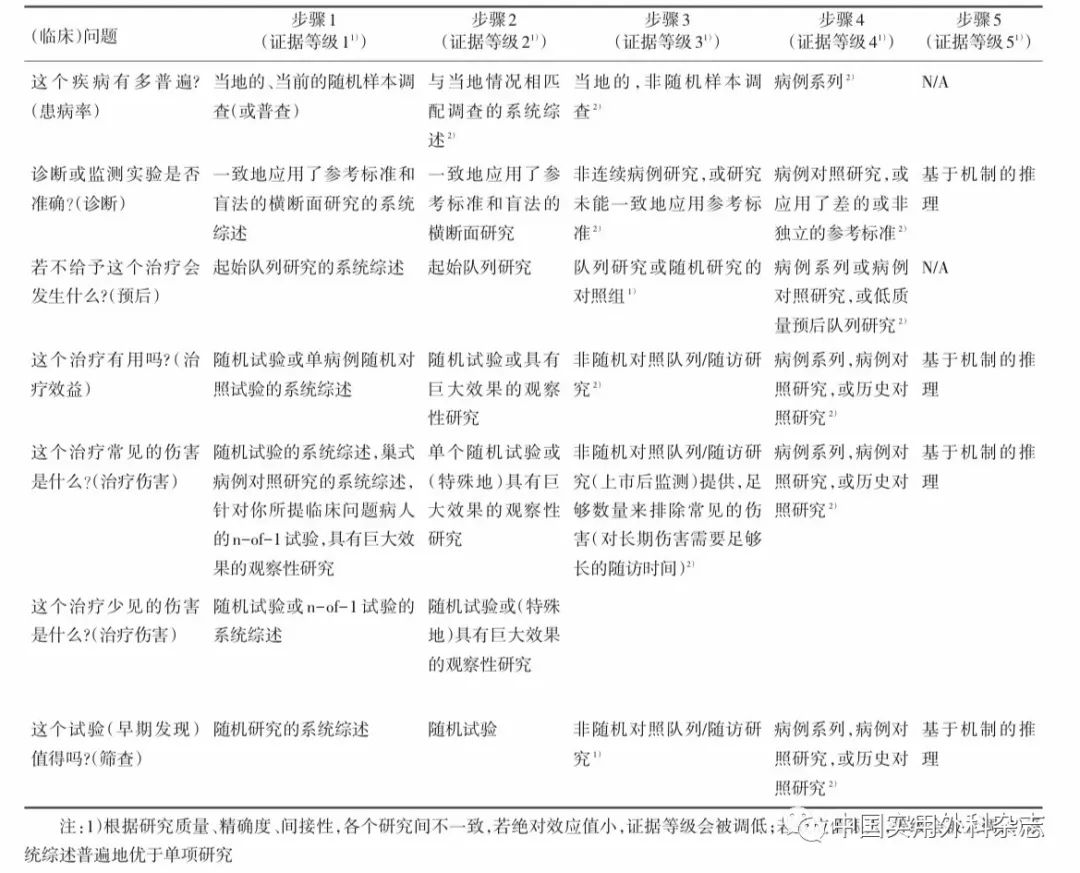
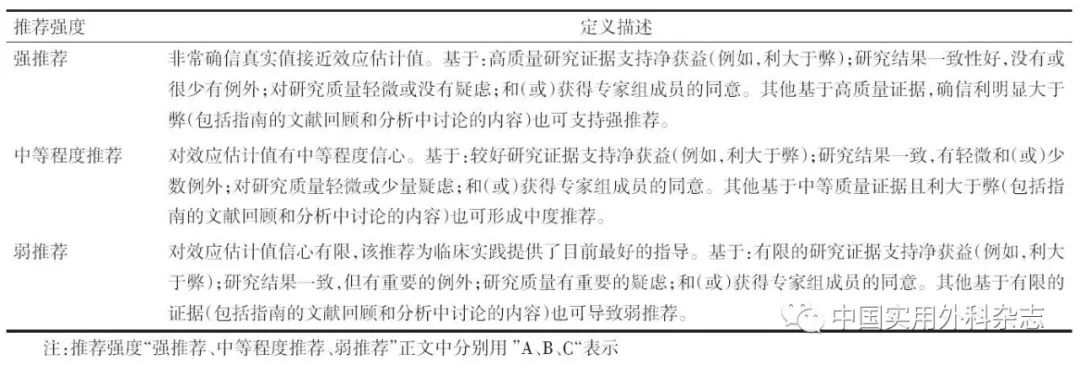
The grading of evidence evaluation and recommendations (grading of recommendations, assessment, development, and evaluation, GRADE) methodology is currently the most widely used system for evidence evaluation and recommendation grading. The GRADE system includes two parts: the first part is evidence evaluation, which classifies the quality of evidence into four levels: high, moderate, low, and very low based on bias risk, inconsistency, indirectness, imprecision, and publication bias in the evidence. The second part is the grading of recommendations, which considers factors such as the balance of benefits and harms of medical interventions, quality of evidence, values and preferences, and costs and resource use to formulate recommendations, classifying recommendations into two categories: strong recommendation and weak recommendation (conditional recommendation). The greater the difference in benefits and harms of medical interventions, the higher the quality of evidence, the clearer and more convergent the values and preferences, and the lower the costs and resource use, the more likely strong recommendations should be considered. Conversely, weak recommendations (conditional recommendations) should be considered. The assessment of the level of evidence in this guideline refers to the above GRADE grading guidelines and uses the 2011 edition of the Oxford Centre for Evidence-Based Medicine grading as an auxiliary tool for specific implementation of evidence grading (Appendix 1). In the method of converting evidence into recommendations, the expert group mainly referred to the aforementioned GRADE guidelines for grading recommendations and made corresponding modifications to the grading scheme based on ASCO guidelines (Appendix 2). Finally, the strength of recommendations is divided into three levels: strong recommendation, moderate recommendation, and weak recommendation. Strong recommendations indicate that the expert group has high confidence that the recommendation reflects the best clinical practice, and the vast majority, if not all, target users should adopt this recommendation. Moderate recommendations indicate that the expert group has moderate confidence that the recommendation reflects the best clinical practice, and most target users will adopt this recommendation, but attention should be paid to consider shared decision-making between doctors and patients during implementation. Weak recommendations indicate that the expert group has some confidence that the recommendation reflects the best clinical practice, but it should be applied conditionally to the target population, emphasizing shared decision-making between doctors and patients.
2 Screening and Diagnosis
2.1 Screening and Monitoring of High-Risk Groups for Liver Cancer Screening and monitoring of high-risk groups for liver cancer are key to early detection, diagnosis, and treatment of liver cancer, which is crucial for improving the efficacy of liver cancer treatment. Rapid and convenient identification of high-risk groups for liver cancer is a prerequisite for implementing large-scale screening, while stratified assessment of population liver cancer risk is the basis for formulating different liver cancer screening strategies. In China, high-risk groups for liver cancer mainly include those with hepatitis B virus (HBV) and/or hepatitis C virus (HCV) infection, excessive alcohol consumption, non-alcoholic fatty liver disease, liver cirrhosis caused by other reasons, and a family history of liver cancer, especially males over 40 years old. Currently, although antiviral treatments for HBV and HCV can significantly reduce the risk of liver cancer occurrence, they cannot completely avoid the occurrence of liver cancer. The aMAP score (age-Male-AlBi-Platelets score), a liver cancer risk assessment model developed by Chinese scholars suitable for various chronic liver diseases and ethnic groups, can conveniently classify liver disease populations into low-risk (0-50 points), moderate-risk (50-60 points), and high-risk (60-100 points) groups, with annual incidence rates of liver cancer in each group being 0-0.2%, 0.4-1.0%, and 1.6-4.0%, respectively, which helps to determine high-risk groups for liver cancer. Early screening for liver cancer using liver ultrasound imaging and serum alpha-fetoprotein (AFP) is recommended for high-risk groups to undergo at least one examination every six months. By implementing a new model of integrated screening in communities and hospitals, efforts should be made to screen as much as possible and treat early.
2.2 Imaging Examination for Liver Cancer Various imaging examination methods each have their characteristics, and comprehensive application and complementary advantages should be emphasized for a thorough evaluation.
2.2.1 Ultrasound Imaging Ultrasound imaging has advantages such as convenience, real-time imaging, non-invasiveness, and no radiation exposure, making it the most commonly used imaging method for liver examination in clinical practice. Routine gray-scale ultrasound imaging can sensitively detect intrahepatic space-occupying lesions early, differentiate them as cystic or solid, and preliminarily judge whether they are benign or malignant. At the same time, gray-scale ultrasound imaging can comprehensively screen for metastases in other organs in the liver or abdominal cavity, as well as assess the involvement of intrahepatic blood vessels and bile ducts. Color Doppler flow imaging can observe the blood supply status of lesions, assist in judging the benign or malignant nature of lesions, demonstrate the relationship between lesions and important intrahepatic blood vessels, and assess the effectiveness of local treatment after liver cancer. Contrast-enhanced ultrasound can dynamically observe changes in blood perfusion of liver tumors in real-time, differentiate between different types of liver tumors, and can sensitively detect hidden small lesions during surgery, guide local treatment in real-time, and assess the effectiveness of local treatment after surgery. Ultrasound-guided elastography can quantitatively assess the hardness of liver tumors and the degree of fibrosis/scarring in surrounding liver tissue, providing useful information for planning reasonable liver cancer treatment. The combined application of multimodal ultrasound imaging technology plays an important role in the precise preoperative diagnosis, intraoperative localization, and postoperative assessment of liver cancer.
2.2.2 CT and MRI Dynamic contrast-enhanced CT and multiparametric MRI scans are the preferred imaging examination methods for clarifying the diagnosis of patients with abnormal liver ultrasound imaging and/or serum AFP screening. CT/MR dynamic enhancement three-phase scans include: arterial late phase (portal vein begins to enhance; typically scanned about 35 seconds after contrast injection), portal vein phase (portal vein is fully enhanced; hepatic veins visible with contrast filling; liver parenchyma usually reaches peak enhancement; typically scanned 60-90 seconds after contrast injection), and delayed phase (both portal vein and hepatic vein are enhanced but lower than the portal vein phase; liver parenchyma shows enhancement but lower than the portal vein phase; typically scanned 3 minutes after contrast injection). Hepatocyte-specific magnetic resonance contrast agent (Gd-EOB-DTPA) dynamic enhancement four-phase scans include: arterial late phase (same as above), portal vein phase (same as above), transitional phase (signal intensity of liver blood vessels and liver parenchyma is the same; liver enhancement is produced by the synergistic action of intracellular and extracellular effects; typically scanned 2-5 minutes after Gd-EOB-DTPA injection), and liver-specific phase (liver parenchyma signal is higher than hepatic vessels; contrast agent is excreted via the biliary system; typically scanned 20 minutes after Gd-EOB-DTPA injection).
Currently, liver CT plain scans and dynamic enhancement scans are not only commonly applied in clinical diagnosis and staging of liver cancer but are also used to evaluate the efficacy of local treatment for liver cancer, especially advantageous for observing the deposition of iodized oil after transcatheter arterial chemoembolization (TACE). Radiomics technology based on preoperative CT can also be used to predict the efficacy of first TACE treatment. At the same time, CT post-processing technology can be used for three-dimensional vascular reconstruction, liver volume and liver tumor volume measurement, and evaluation of metastases in other organ tissues such as lungs and bones, and has been widely applied in clinical practice.
Multiparametric MRI of the liver has advantages such as no radiation exposure, high tissue resolution, and multi-directional multi-sequence multi-parameter imaging capabilities, and its combined imaging technology that integrates morphology and function (including diffusion-weighted imaging) has become the preferred imaging technology for clinical detection, diagnosis, staging, and efficacy evaluation of liver cancer. Multiparametric MRI has superior detection and diagnostic capabilities for liver cancer with a diameter ≤2.0 cm compared to dynamic contrast-enhanced CT. Multiparametric MRI has advantages over dynamic contrast-enhanced CT in evaluating whether liver cancer invades the portal vein, hepatic vein trunk, and its branches, as well as lymph node metastasis in the abdominal cavity or retroperitoneal space. When evaluating the efficacy of local treatment for liver cancer using multiparametric MRI scans, it is recommended to use the modified response evaluation criteria in solid tumors (mRECIST) combined with T2-weighted imaging and diffusion-weighted imaging for comprehensive judgment.
Imaging diagnosis of liver cancer mainly relies on the enhancement pattern of dynamic contrast-enhanced scans. Dynamic contrast-enhanced CT and multiparametric MRI arterial phase (mainly in the arterial late phase) show homogeneous or heterogeneous significant enhancement of liver tumors, while portal vein phase and/or delayed phase enhancement of liver tumors is lower than that of liver parenchyma. “Fast in” refers to non-annular enhancement, while “fast out” refers to non-peripheral clearance. “Fast in” is observed in the arterial late phase, while “fast out” is observed in the portal vein phase and delayed phase. Gd-EOB-DTPA can only show “fast out” signs in the portal vein phase, and transitional phase and liver-specific phase “fast out” signs can serve as auxiliary malignant signs.
Gd-EOB-DTPA-enhanced MRI shows: liver tumors significantly enhance in the arterial phase, while enhancement in the portal vein phase is lower than that of liver parenchyma, and liver-specific phase often shows significantly low signal. 5%-12% of well-differentiated small liver cancers may show slightly higher signals in the liver-specific phase. Multiparametric MRI scans for liver cancer, especially in diagnosing tumors with a diameter ≤2.0 cm/<1.0 cm, emphasize that comprehensive judgment should still be combined with other signs (such as capsule-like enhancement, intermediate signals in T2-weighted imaging, and diffusion restriction) and threshold growth [growth of the maximum diameter of the lesion by 50% (inclusive) within 6 months]. Capsule-like enhancement is defined as: smooth, uniform, clear boundaries, mostly or completely surrounding the lesion, especially showing annular enhancement in the portal vein phase, delayed phase, or transitional phase.
Gd-EOB-DTPA-enhanced MRI examination combined with low signal in the liver-specific phase, arterial phase enhancement, and diffusion restriction signs can significantly improve the diagnostic sensitivity of liver cancer with a diameter <1.0 cm, especially in patients with cirrhosis, and is strongly recommended to use this method, which also helps to differentiate high-grade dysplastic nodules and other precancerous lesions.
Based on clinical data mining of liver cancer CT and/or MRI information, establishing a fused model can help improve clinical decision-making (patient treatment plan selection, efficacy evaluation, and prediction, etc.). For preoperative prediction of microvascular invasion (MVI) in liver cancer, imaging signs are highly specific but have low sensitivity, and nomograms and radiomics models are potential breakthroughs for preoperative prediction of MVI.
3 Staging
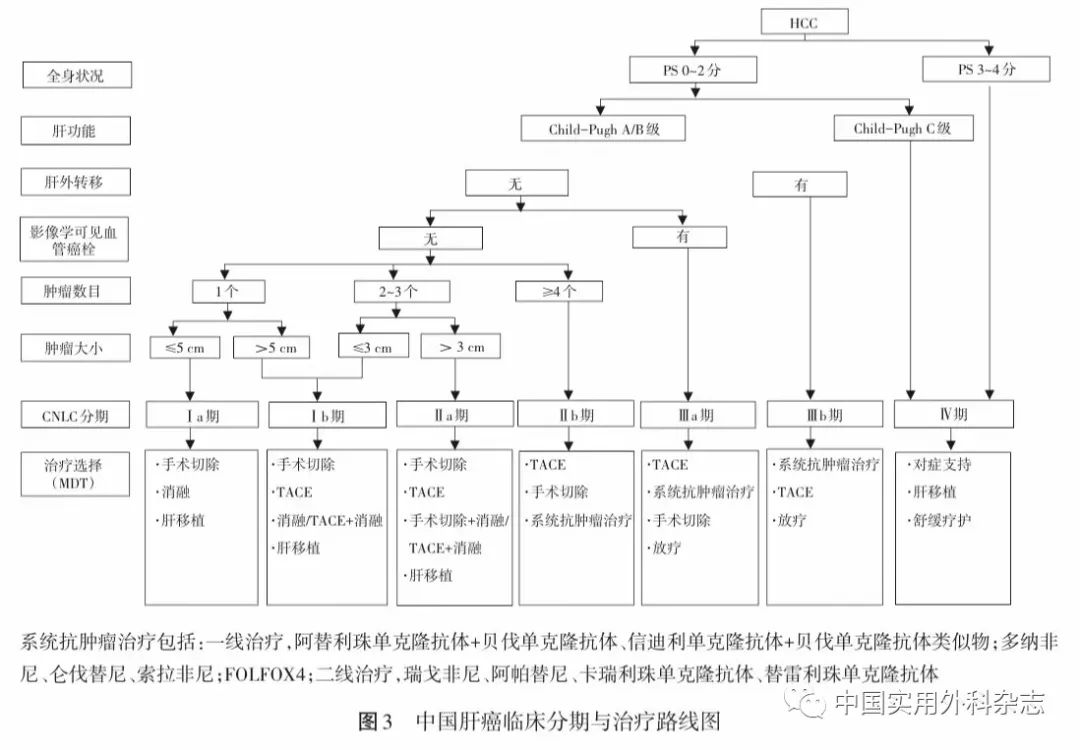
The staging of liver cancer is crucial for the selection of treatment plans and prognosis assessment. There are various staging schemes abroad, such as BCLC, TNM, JSH, and APASL. Combining the specific national conditions and practical accumulation in China, a staging scheme for liver cancer in China (China liver cancer staging, CNLC) has been established based on the patient’s performance status (PS), liver tumor, and liver function condition, including: CNLC stage I a, I b, II a, II b, III a, III b, and IV, with specific staging scheme descriptions in the figure.
CNLC stage I a: PS 0~2 points, liver function Child-Pugh A/B grade, single tumor, diameter ≤5 cm, no radiologically visible vascular cancer thrombus and liver metastasis;
CNLC stage I b: PS 0~2 points, liver function Child-Pugh A/B grade, single tumor, diameter >5 cm, or 2-3 tumors, maximum diameter ≤3 cm, no radiologically visible vascular cancer thrombus and liver metastasis;
CNLC stage II a: PS 0~2 points, liver function Child-Pugh A/B grade, 2-3 tumors, maximum diameter >3 cm, no radiologically visible vascular cancer thrombus and liver metastasis;
CNLC stage II b: PS 0~2 points, liver function Child-Pugh A/B grade, ≥4 tumors, regardless of tumor diameter, no radiologically visible vascular cancer thrombus and liver metastasis;
CNLC stage III a: PS 0~2 points, liver function Child-Pugh A/B grade, regardless of tumor condition, radiologically visible vascular cancer thrombus without liver metastasis;
CNLC stage III b: PS 0~2 points, liver function Child-Pugh A/B grade, regardless of tumor condition, regardless of whether there is radiologically visible vascular cancer thrombus, with liver metastasis;
CNLC stage IV: PS 3~4 points, or liver function Child-Pugh C grade, regardless of tumor condition, regardless of whether there is radiologically visible vascular cancer thrombus, regardless of whether there is liver metastasis.
4 Treatment
The treatment of liver cancer is characterized by multidisciplinary participation and coexistence of various treatment methods. Common treatment methods include liver resection, liver transplantation, ablation therapy, TACE, radiotherapy, systemic anti-tumor therapy, and various means. Choosing a reasonable treatment method for patients with liver cancer at different stages can maximize efficacy. The choice of a reasonable treatment method needs support from high-level evidence-based medicine. Currently, standardized comprehensive therapy with ordered combinations has the best long-term efficacy for liver cancer, but there is a certain contradiction between the current departmental diagnosis and treatment system based on different treatment methods and the realization of standardized comprehensive therapy. Therefore, liver cancer diagnosis and treatment must pay attention to the multidisciplinary team (MDT) treatment model, especially for the diagnosis and treatment of difficult and complex cases, to avoid the limitations of single-department treatment, promote discipline communication, and improve overall efficacy. It is recommended that liver cancer MDT management should work around the core quality control indicators for liver cancer diagnosis and treatment established by the National Health Commission, but also consider the differences in regional economic levels and the medical capabilities and conditions of each hospital.
4.1 Surgical Treatment Surgical treatment of liver cancer is an important means for liver cancer patients to achieve long-term survival, mainly including liver resection and liver transplantation.
4.1.1 Basic Principles of Liver Resection (1) Thoroughness: Complete removal of tumors with no residual tumor at the cutting edge. (2) Safety: Retaining sufficient volume and functional liver tissue (with good blood supply and good blood and bile flow) to ensure postoperative liver function compensation, reduce surgical complications, and lower mortality.
4.1.2 Preoperative Assessment of the Patient’s Overall Condition and Liver Reserve Function Before surgery, a comprehensive evaluation of the patient’s overall condition, liver reserve function, and liver tumor condition (staging and location) should be conducted, often using the performance status score (ECOGPS) proposed by the Eastern Cooperative Oncology Group to assess the patient’s overall condition; using the Child-Pugh grading of liver function, indocyanine green (ICG) clearance test, or transient elastography to measure liver stiffness to assess liver reserve function. Research results suggest that selected liver cancer patients with concomitant portal hypertension can still undergo liver resection, and their postoperative long-term survival is better than that of other treatments. Therefore, more precise evaluation of the degree of portal hypertension (such as hepatic venous pressure gradient measurement) is helpful to screen suitable patients for surgical resection. If the expected remaining liver tissue volume is relatively small, the remaining liver volume should be measured using CT, MRI, or three-dimensional reconstruction of the liver, and the percentage of remaining liver volume to standardized liver volume should be calculated. It is generally believed that Child-Pugh A liver function and ICG 15-minute retention rate (ICG-R15) <30% are necessary conditions for performing surgical resection; the remaining liver volume should account for more than 40% of the standardized liver volume (for those with chronic liver disease, liver parenchymal damage, or cirrhosis) or more than 30% (for those without liver fibrosis or cirrhosis), which are also necessary conditions for performing surgical resection. For patients with liver function damage, more remaining liver volume should be preserved.
4.1.3 Indications for Liver Cancer Resection (1) For liver cancer patients with good liver reserve function at CNLC stage I a, I b, and II a, the preferred treatment is surgical resection. Previous research results show that for liver cancers with a diameter ≤3 cm, there is no statistically significant difference in efficacy between surgical resection and radiofrequency ablation; however, recent research results indicate that the local recurrence rate after surgical resection is significantly lower than that after radiofrequency ablation, and the long-term efficacy of surgical resection is better. Even for recurrent liver cancer, the prognosis of surgical resection is still better than that of radiofrequency ablation. (2) For patients with CNLC stage II b liver cancer, surgical resection is generally not the preferred choice, while non-surgical treatment based on TACE is preferred. If the tumor is limited to the same segment or same side of the liver, or if intraoperative ablation can be performed on lesions outside the resection range, surgical resection may achieve better results than other treatments, thus surgical resection is also recommended, but it requires more cautious preoperative multidisciplinary assessment.
(3) For patients with CNLC stage III a liver cancer, the vast majority should not be the preferred choice for surgical resection, while non-surgical treatment based on systemic anti-tumor therapy is preferred. If the following conditions are met, surgical resection can also be considered: (1) those with portal vein branch cancer thrombus (Cheng’s type I/II), if the tumor is limited to half of the liver or the same side of the liver, surgical resection of the tumor can be considered, and portal vein embolization can be performed afterward, followed by TACE treatment, portal vein chemotherapy, or other systemic anti-tumor therapies; portal vein main trunk cancer thrombus (Cheng’s type III) has a high short-term recurrence rate after surgery, and most patients have poor postoperative survival, so it is not an absolute indication for surgical resection. For resectable liver cancer patients with portal vein cancer thrombus, preoperative three-dimensional conformal radiotherapy can improve postoperative survival. (2) Those with bile duct cancer thrombus but liver lesions can also be resected. (3) Some liver cancer patients with invasion of hepatic veins but liver lesions can be resected.
4.1.4 Standards for Radical Resection of Liver Cancer (1) Intraoperative judgment criteria: (1) No visible cancer thrombus in hepatic veins, portal veins, bile ducts, or inferior vena cava; (2) no adjacent organ invasion, no lymph node metastasis or distant metastasis; (3) the distance from the liver cutting edge to the tumor boundary is ≥1 cm; if the distance is <1 cm, then the pathological examination of the liver cutting surface shows no residual tumor cells, i.e., the cutting edge is negative.
(2) Postoperative judgment criteria: (1) Ultrasound, CT, or MRI examinations (must have at least two of these) performed 1-2 months after surgery do not find tumor lesions; (2) if preoperative serum tumor markers such as AFP, DCP, etc. were elevated, then quantitative measurement of serum tumor markers should be required to drop back to normal range 2 months after surgery. The rate of decline in serum tumor markers such as AFP after resection can predict the thoroughness of surgical resection early.
4.1.5 Surgical Resection Techniques Common liver resection techniques include intrahepatic and extrahepatic blood flow control techniques, liver dissection techniques, and hemostatic techniques. Preoperative three-dimensional visualization technology for individualized liver volume calculation and virtual liver resection helps design more precise resection ranges and paths to protect the remaining liver while achieving the goal of radical tumor resection.
In recent years, laparoscopic liver surgery has developed rapidly. Laparoscopic liver resection has the advantages of less trauma and faster recovery, and its oncological effect is comparable to open liver resection in selected patients. Although the indications and contraindications for laparoscopic liver resection are generally similar to those for open surgery, it is still recommended to carefully evaluate and cautiously carry out the procedure based on tumor size, location, number, underlying liver disease, and the technical level of the surgical team. For large liver cancers, multiple liver cancers, liver cancers located in difficult positions, and those adjacent to important ducts, it is recommended that this treatment be performed by experienced physicians after strict selection. The use of laparoscopic ultrasound examination combined with indocyanine green fluorescence tumor imaging can help detect small lesions and mark the resection range to achieve tumor-negative margins.
Both anatomical and non-anatomical resections are commonly used liver resection techniques, and both require sufficient margins to achieve good oncological outcomes. For liver cancer cases with MVI, anatomical resection has a lower local recurrence rate compared to non-anatomical resection, although there is no difference in overall survival. Research results have found that wide margins (≥1 cm) for liver resection yield better outcomes than narrow margins, especially for patients with predicted MVI preoperatively. For large liver cancers, the anterior approach liver resection method can be used to free the liver from surrounding ligaments. For multiple liver cancers, surgical resection combined with intraoperative ablation therapy can be used.
For patients with portal vein cancer thrombus, portal vein embolization should be performed temporarily to prevent cancer thrombus dissemination. For patients with hepatic venous cancer thrombus or inferior vena cava cancer thrombus, total hepatic blood flow occlusion can be performed to remove the cancer thrombus as a whole as much as possible. For liver cancer with bile duct cancer thrombus, simultaneous resection of the liver tumor and bile duct is recommended to obtain the opportunity for radical resection.
For liver cancer that is found to be unsuitable for surgical resection during intraoperative exploration, intraoperative arterial and portal vein catheter chemotherapy or other local treatment measures may be considered, or subsequent TACE treatment or systemic anti-tumor treatment after surgical trauma recovery may be performed.
4.1.6 Comprehensive Treatment Strategy Focused on Surgery Based on previous extensive case data, although the overall survival of patients with intermediate and advanced liver cancer (CNLC II b, III a, III b) after surgery is not satisfactory, surgical resection can still benefit some patients in the absence of other effective treatment methods. Currently, significant progress has been made in systemic anti-tumor therapy and comprehensive treatment, and the effects of systemic anti-tumor therapy and/or local treatment in controlling tumors can provide more possibilities for radical resection, reduce postoperative recurrence, and improve prognosis. Therefore, it is necessary to re-evaluate the strategy of direct surgical resection for patients with intermediate and advanced liver cancer. Exploring new strategies for comprehensive treatment focused on surgery for patients with intermediate and advanced liver cancer has become a recent focus.
4.1.6.1 Conversion Therapy for Potentially Resectable Liver Cancer Conversion therapy is one of the pathways for patients with unresectable liver cancer to achieve radical resection and long-term survival. For potentially resectable liver cancer, it is recommended to adopt a multi-modal, high-intensity anti-tumor treatment strategy to promote conversion, while ensuring the safety and quality of life of patients.
(1) Conversion therapy targeting tumors: (1) Systemic anti-tumor therapy: The standalone or combined application of systemic anti-tumor therapy is one of the main methods for conversion therapy of intermediate and advanced liver cancer. The depth, speed, and duration of liver cancer relief, as well as organ-specific relief, are important factors influencing subsequent treatment decisions. More exploration is needed on the impact of different drug combinations on liver tissue and subsequent surgical safety. (2) Local treatment: Including TACE, hepatic arterial infusion chemotherapy (HAIC), and other local treatment methods create opportunities for initial unresectable liver cancer patients to undergo potential surgical resection and can translate into survival benefits. Radiotherapy combined with HAIC and HAIC combined with TACE can further improve conversion rates. The combination of systemic anti-tumor therapy and local treatment is expected to achieve higher tumor relief and higher conversion resection rates.
(2) Conversion therapy for insufficient remaining liver volume: (1) Portal vein embolization (PVE): The half of the liver where the tumor is located is embolized to promote compensatory hyperplasia of the remaining liver before tumor resection. The success rate of PVE is 60%-80%, and the complication rate is 10%-20%. The remaining liver hyperplasia time after PVE is relatively long (usually 4-6 weeks), and more than 20% of patients may lose the opportunity for surgery due to tumor progression or insufficient remaining liver hyperplasia. (2) Staged liver resection with liver partition and portal vein ligation (ALPPS): Suitable for patients whose expected remaining liver volume is <30%-40% of the standard liver volume. In recent years, various improved ALPPS techniques have emerged, mainly focusing on the first-stage liver partition operation (partial partitioning and partitioning using radiofrequency ablation, microwave, hemostatic clips, etc.) and laparoscopic minimally invasive approaches for ALPPS. Preoperative assessment is crucial, taking into account the degree of cirrhosis, patient age, and short-term ability to tolerate two surgeries. ALPPS surgery can improve the resection rate of liver cancer in a short time, and its ability to rapidly induce hyperplasia of the remaining liver is superior to PVE; due to the short interval between the two surgeries, it can minimize the risk of tumor progression, achieving a tumor resection rate of 95%-100%. Research results show that ALPPS treatment for large or multiple liver cancers is superior to TACE.
4.1.6.2 Neoadjuvant Therapy According to the definition of the National Cancer Institute, neoadjuvant therapy is treatment aimed at shrinking tumors before the main treatment (usually surgery). Common neoadjuvant therapies include systemic anti-tumor therapy, interventional therapy, radiotherapy, etc., with the goal of reducing postoperative recurrence and prolonging survival. For resectable intermediate and advanced liver cancer (CNLC II b, III a), neoadjuvant therapy can transform liver cancer with poor oncological characteristics into liver cancer with better oncological characteristics, thereby reducing postoperative recurrence and prolonging survival. For patients with resectable liver cancer with portal vein cancer thrombus, preoperative three-dimensional conformal radiotherapy can improve efficacy. However, for liver cancer that is technically resectable, preoperative TACE does not extend patient survival. Strategies involving immunotherapy and targeted drugs, either alone or in combination, are being actively explored for preoperative or perioperative treatment of resectable liver cancer, with the potential to further enhance surgical efficacy. However, for earlier stages of liver cancer (CNLC I a, I b, II a), whether preoperative treatment can improve patient survival and reduce recurrence still requires clinical research confirmation.
4.1.6.3 Adjuvant Therapy The recurrence and metastasis rate of tumors after liver resection can be as high as 40%-70% within 5 years, which is related to the possible existence of small disseminated lesions or multicentric occurrences before surgery. Therefore, all patients need close follow-up after surgery. For patients at high risk of recurrence, two randomized controlled studies have confirmed that postoperative TACE treatment can reduce recurrence and prolong survival. Another randomized controlled study found that postoperative treatment with Huai Er granules can reduce recurrence and prolong patient survival. For liver cancer patients with HBV infection, nucleoside analog antiviral treatment can not only control underlying liver disease but also help reduce the recurrence rate after surgery. For HCV-infected liver cancer patients, direct-acting antiviral agents (DAAs) can achieve sustained virological response, and currently, there is no conclusive data indicating whether DAA treatment is associated with increased or decreased risk of postoperative tumor recurrence, differences in recurrence timing, or invasiveness of recurrent liver cancer. Additionally, for patients with portal vein cancer thrombus, postoperative portal vein catheter chemotherapy combined with TACE can also prolong patient survival. Although clinical randomized studies suggest that alpha-interferon can reduce recurrence and prolong survival, this remains controversial. Reports have found that the expression of liver cancer miR-26a is related to the efficacy of alpha-interferon treatment, and this result also needs further multi-center randomized controlled trials for validation.
4.5.4 Efficacy Evaluation of Systemic Anti-Tumor Therapy For patients undergoing systemic anti-tumor therapy, most currently use the response evaluation criteria in solid tumors (RECIST) 1.1 for efficacy evaluation. For patients receiving anti-angiogenic targeted therapy, mRECIST can be applied in conjunction. For patients receiving immune checkpoint inhibitor therapy, the immune tumor response evaluation criteria (iRECIST) can also be applied.
4.6 Treatment of Spontaneous Rupture of Liver Cancer Spontaneous rupture of liver cancer is a potential fatal complication of liver cancer, and conservative treatment alone has a very high in-hospital mortality rate, but it is not a determining factor affecting the long-term survival of patients. Therefore, after initial successful rescue, a comprehensive assessment of the patient’s hemodynamics, liver function, overall condition, and whether the tumor is resectable should be conducted to formulate an individualized treatment plan.
For patients with resectable liver tumors, good liver reserve function, and stable hemodynamics, surgical resection is the first choice. For patients with poor liver reserve function, unstable hemodynamics, and no surgical conditions, TAE can be selected. Due to emergency conditions, when liver function and tumor status cannot be fully assessed, TAE can be performed first, combined with subsequent evaluation to select appropriate treatment plans. If a two-stage surgical resection can be performed, significant survival benefits can be obtained.
Spontaneous rupture of liver cancer is a high-risk recurrence factor after surgery; during surgery, the abdominal cavity should be thoroughly washed, and auxiliary treatments should be provided after surgery; for patients with pure peritoneal metastasis, active radical resection can be considered.
5 Declaration
The compilation of this guideline is independent of any sponsoring organization, and all authors have committed that the content of the compilation is unrelated to whether funding was received.
Appendix 1 Level of Evidence (Oxford Centre for Evidence-Based Medicine 2011 Edition)
Appendix 2 Strength of Recommendations
Appendix 3 Introduction of Novel Markers and Molecular Typing for Liver Cancer
In recent years, “liquid biopsy” including circulating cell-free microRNA, circulating tumor cells (CTC), circulating tumor DNA (ctDNA), etc., has shown significant value in early diagnosis and efficacy evaluation of tumors. Liquid biopsy for liver cancer has also made considerable progress, potentially offering higher sensitivity and specificity compared to commonly used serological molecular markers such as serum AFP.
CTC detection can become a new clinical tool for predicting prognosis and evaluating efficacy in liver cancer. Reports indicate that peripheral blood EpCAM+ CTCs have stem cell-like properties and are independent predictors of early recurrence after liver cancer resection; detection of CTCs can predict recurrence and progression after TACE treatment and radiotherapy; CTCs from different sites can predict different types of metastases; dynamic monitoring of CTCs can be used to monitor tumor recurrence after liver transplantation. ctDNA, which is specific mutated DNA fragments released by tumors into peripheral blood, can reflect genomic information of tumors and can be used for early diagnosis, monitoring tumor progression, and response to treatment. Reports indicate that ctDNA has superior sensitivity and specificity for early diagnosis of liver cancer compared to serum AFP, and can also reflect dynamic changes after liver cancer surgery. Specific genetic epigenetic modification characteristics, such as methylation, can also be used for early diagnosis of liver cancer.
Research on genomics, transcriptomics, epigenomics, and proteomics provides a basis for molecular typing of liver cancer, which reflects different biological backgrounds of liver cancer and has important implications for predicting efficacy and treatment selection for liver cancer patients. Currently, Chinese liver cancer patients can be classified into three subtypes: metabolism-driven, microenvironment-disordered, and proliferation-driven; or three proteomic subtypes, namely S-I, S-II, and S-III.
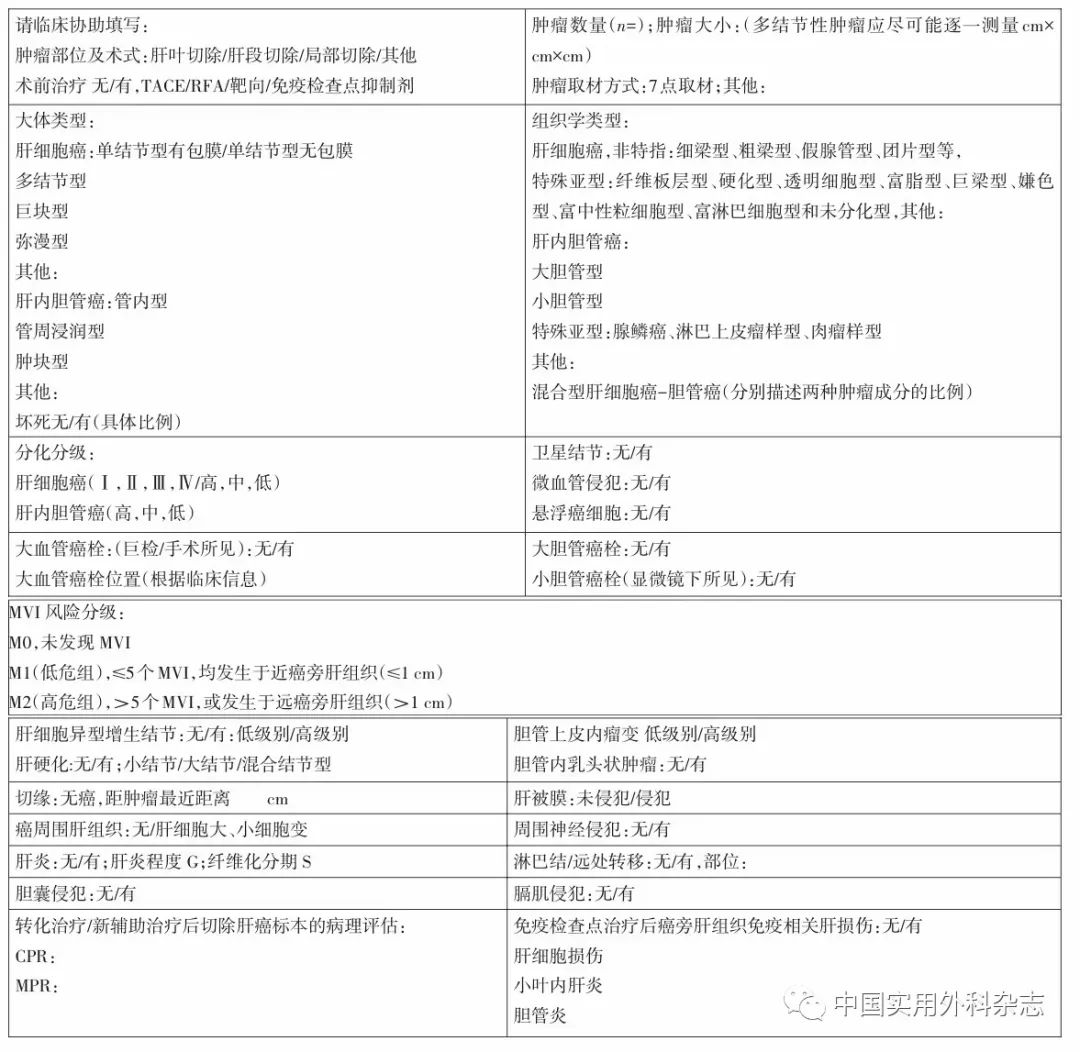
Appendix 4 Recommended Pathological Diagnosis Report and Main Description Indicators for Liver Cancer
Appendix 5 Classification of Portal Vein Cancer Thrombus
Cheng’s Classification:
Type I: Portal vein cancer thrombus invades the portal vein branches of liver lobes or segments.
Type II: Portal vein cancer thrombus invades the left or right branch of the portal vein.
Type III: Portal vein cancer thrombus invades the main trunk of the portal vein.
Type IV: Portal vein cancer thrombus invades the superior mesenteric vein.
Type I0: Pathological diagnosis of portal vein microvascular invasion postoperatively.
Vp classification by the Japanese Liver Cancer Research Society:
Vp1: Portal vein cancer thrombus is limited to the secondary branches of the portal vein or beyond.
Vp2: Portal vein cancer thrombus invades the secondary branches of the portal vein.
Vp3: Portal vein cancer thrombus invades the primary branches of the portal vein.
Vp4: Portal vein cancer thrombus invades the main trunk of the portal vein or contralateral primary branches.
Appendix 6 Progress in Transcatheter Arterial Chemoembolization Treatment
(1) HAIC: As a method of intra-arterial chemotherapy, HAIC currently lacks a unified technical standard, and there is considerable variability in efficacy. A multi-center RCT phase II clinical trial in Japan (the SCOOP-2 trial) compared cisplatin HAIC sequential with sorafenib versus standard sorafenib monotherapy in patients with advanced liver cancer, and the results showed that the median survival time of the HAIC combined treatment group was 10 months, compared to 15.2 months in the standard sorafenib monotherapy group, indicating that the efficacy was not ideal. The HAIC combined treatment group had 23% of patients unable to receive any further treatment due to deterioration of their general condition. A multi-center randomized phase III trial (the SILIUS trial) not only confirmed the negative results of the aforementioned prospective randomized phase II trial but also tested different HAIC regimens (low-dose cisplatin-fluorouracil) combined with sorafenib against sorafenib monotherapy in Japanese patients with advanced liver cancer, which also yielded negative results. Therefore, most Japanese experts discussed that standalone chemotherapy or combined targeted therapy has no proven efficacy, and HAIC is not suitable as a treatment for advanced liver cancer. In recent years, Chinese scholars have improved HAIC efficacy using the mFOLFOX-based infusion regimen. Research has shown that HAIC treatment is superior to sorafenib treatment for liver cancer patients who have developed resistance to multiple TACE treatments, those with portal vein cancer thrombus, those with high recurrence risk post-surgery, and those with liver metastases. For liver cancer patients with portal vein cancer thrombus (CNLC stage III a), HAIC combined with sorafenib treatment is significantly more effective than sorafenib monotherapy. Similar to TACE, mFOLFOX-HAIC helps to convert some tumors with a maximum diameter of >7 cm that are initially unsuitable for surgical resection, but it is generally recommended that at least 4 or more HAIC treatments be completed to achieve conversion opportunities.
(2) Preoperative predictive models for TACE prognosis: (1) The “Six-and-twelve” model: The sum of tumor size and number ≤6, >6 and ≤12, >12. This model provides individualized prognostic assessment and risk stratification for patients undergoing TACE treatment for liver cancer, with significant differences in median survival time among patients with different risk stratifications. Therefore, using the “Six-and-twelve” model can provide reference values for postoperative expected survival for liver cancer patients undergoing TACE, assisting patients in choosing different treatment methods. (2) The prognostic nomogram for TACE includes factors such as portal vein invasion, tumor number, tumor capsule, serum AFP, aspartate transaminase, ICG-R15, etc. This model has been validated in 868 liver cancer patients, achieving a C-index of 0.755 related to predicting survival. Therefore, using these two models can provide reference values for postoperative expected survival for liver cancer patients undergoing TACE, assisting patients in choosing different treatment methods. (3) The “TACE-predict” model is an individualized prognostic assessment and risk stratification model applicable preoperatively and recalibrated postoperatively for the TACE liver cancer population. Research has found that tumor number and diameter, AFP, bilirubin, vascular invasion, and etiology are prognostic factors for patients preoperatively, while tumor number and diameter, AFP, bilirubin, vascular invasion, and imaging response are prognostic factors for patients postoperatively. Thus, the Pre-TACE-Predict model and Post-TACE-Predict model were established, which can calculate the survival probability of patients preoperatively and postoperatively, respectively. The predictive ability of the Pre-TACE-Predict model and Post-TACE-Predict model is superior to that of HAP and mHAP III scores. The Post-TACE-Predict model can further assess prognosis and risk stratification for patients after TACE, which has significant implications for guiding clinical practice.
(3) TACE/HAIC combined with targeted molecular therapy and immunotherapy: The TACTICS phase II clinical study shows that TACE combined with sorafenib significantly improves PFS compared to TACE alone, but the final OS did not reach statistical significance. TACE/HAIC may affect the tumor microenvironment, and combined with targeted molecular drugs or immunotherapy has shown promising treatment prospects, but most studies are currently small sample sizes with low levels of evidence-based medicine, requiring further multi-center, large-sample, high-quality clinical studies for clarification.
4.4 External Radiotherapy
External radiotherapy is divided into external beam radiotherapy and internal radiotherapy. External radiotherapy uses radiation (photons or particles) generated by radiotherapy equipment to irradiate tumors from outside the body. Internal radiotherapy uses radioactive nuclides implanted inside tumors through body pathways or needle tracks.
4.4.1 External Beam Radiotherapy (1) Indications for external beam radiotherapy: (1) Liver cancer patients at CNLC stage I a or part of CNLC stage I b, if there are no surgical resection or ablation treatment indications or if they are unwilling to undergo invasive treatment, SBRT can be considered as a treatment method. (2) For CNLC stage II a and II b liver cancer patients, TACE combined with external beam radiotherapy can improve local control rates and prolong survival, and is better than TACE alone, sorafenib, or TACE combined with sorafenib. (3) For CNLC stage III a liver cancer patients, preoperative neoadjuvant radiotherapy or postoperative adjuvant radiotherapy can prolong survival for those with resectable liver cancer with portal vein cancer thrombus; for those who cannot be surgically resected, palliative radiotherapy or combined treatment with TACE can prolong survival. (4) For CNLC stage III b liver cancer patients with some oligometastatic lesions, SBRT can prolong survival; external radiotherapy can also alleviate symptoms such as pain, obstruction, or bleeding caused by metastatic lesions in lymph nodes, lungs, bones, brain, or adrenal glands.
4.4.2 Contraindications for External Beam Radiotherapy: Liver cancer patients with diffuse intrahepatic lesions or those at CNLC stage IV are not recommended for external beam radiotherapy.
4.4.3 Principles and Key Points for Implementing External Beam Radiotherapy: The principles of implementing external beam radiotherapy for liver cancer are to comprehensively consider the radiation dose to the tumor, the tolerable dose of surrounding normal tissues, and the radiotherapy technology used. Key points for implementing external beam radiotherapy for liver cancer include: (1) When formulating the radiotherapy plan, liver lesions should be defined in enhanced CT, and if necessary, reference should be made to multiple imaging data such as MRI, allowing some normal liver tissue to be spared during radiotherapy, as this may allow some normal liver tissue to gain hyperplasia. (2) The radiation dose to liver cancer is closely related to patient survival time and local control rates, primarily depending on the tolerable dose of surrounding normal tissues. The recommended doses for stereotactic radiotherapy are generally ≥45-60 Gy/3-10 fractions, while conventional fractionated radiotherapy is generally 50-75 Gy. The dose for neoadjuvant radiotherapy for portal vein cancer thrombus can be 3 Gy × 6 fractions. For patients with image-guided radiotherapy (IGRT) technology, some intrahepatic lesions, cancer thrombi, or metastatic lesions in liver, lymph nodes, lungs, etc. can undergo hypofractionated radiotherapy to improve single-dose delivery, shorten radiotherapy time, and not affect or even enhance efficacy. (3) The tolerable dose of normal tissues must consider: the mode of radiotherapy fractionation, liver function Child-Pugh grading, normal liver (liver-tumor) volume, gastrointestinal congestion, and coagulation function status.
4.4.4 Major Complications of External Beam Radiotherapy: Radiation-induced liver disease (RILD) is a dose-limiting complication of external beam radiotherapy to the liver, classified into typical and atypical types. (1) Typical RILD: Alkaline phosphatase elevation >2 times the upper limit of normal, no jaundice, ascites, or liver enlargement; (2) Atypical RILD: Alkaline phosphatase >2 times the upper limit of normal, alanine transaminase >upper limit of normal or 5 times the pre-treatment level, liver function Child-Pugh score decreases by ≥2 points, but without liver enlargement or ascites. Diagnosing RILD must exclude clinical symptoms and liver function damage caused by tumor progression, viral or drug-related causes.