Follow us
Click on the blue text above to follow us
Testing Project Information
Testing Item: Myositis Antibody Spectrum Testing for 19 Items (Mi-2, Ku, PM-Scl100, PM-Scl75, Jo-1, SRP, PL-7, PL-12, EJ, Ro-52, TIF1γ, MDA5, NXP2, HMGCR, SAE, OJ, KS, ZO, HA)
Medical Advice Information
Advice Code: JYJYK4055,
Advice Name: Myositis Antibody Spectrum Testing
Advice Price: 800 yuan
Advice Search: You can search using initials, advice name, or advice code.
Advice Classification: Medical Laboratory – Clinical Immunology
Collection and Submission Requirements
No need for fasting. Use a red top tube for blood collection of 3ml, and submit as soon as possible after sampling.
Specimens are accepted within 24 hours.
Severe hemolysis or hyperlipidemia can affect results.
Report Time
Testing on Tuesdays and Fridays (excluding holidays).
Samples submitted before 8:30 on Tuesdays and Fridays will receive reports the same day.
Samples submitted after 8:30 on Tuesdays and Fridays will receive reports on the next testing day.
Consultation Contact
Clinical Immunology Group, Medical Laboratory, Internal Phone2741.

Why Test for Myositis Antibody Spectrum?
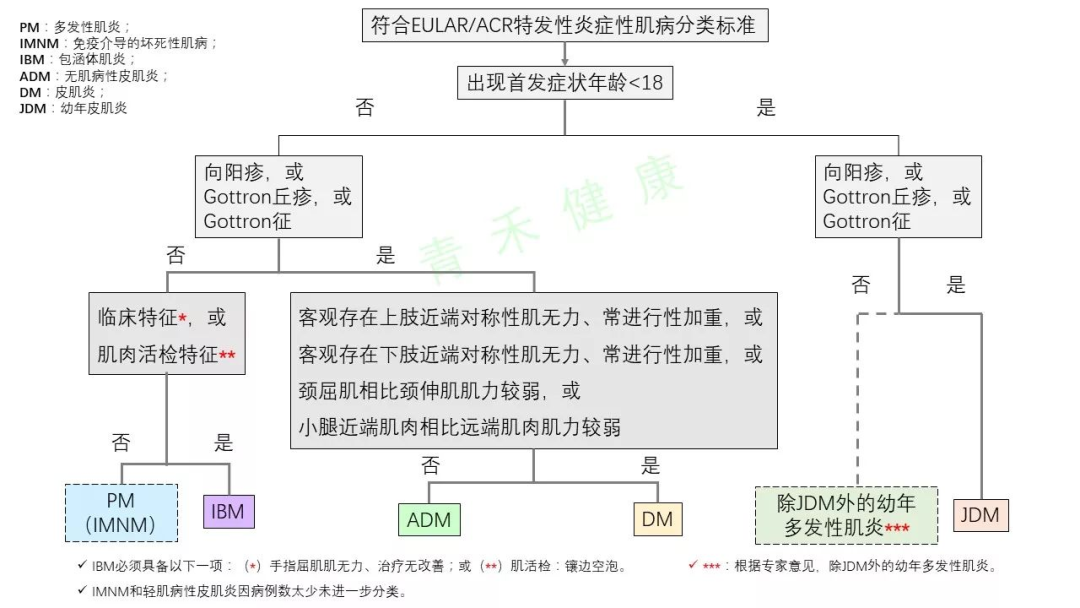
Idiopathic Inflammatory Myopathy (IIM) is an autoimmune disease mediated by T cells, primarily attacking muscle fibers expressing major histocompatibility complex I (MHCI). It presents with a variety of clinical manifestations and has significant heterogeneity, mainly classified into five types: (1) Dermatomyositis; (2) Antisynthetase Syndrome; (3) Immune-mediated Necrotizing Myopathy; (4) Polymyositis; (5) Sporadic Inclusion Body Myositis. The first three subtypes are the most common clinically.
The epidemiology of IIM is not well documented in large-scale clinical data. Among them, the incidence of polymyositis and dermatomyositis is0.5-1.0/10 thousand. Females are more affected than males, and it can occur at any age. Without treatment, it typically does not improve spontaneously but can benefit from immunotherapy. The estimated mortality rate is20-30%, with the highest mortality rate in the first year of illness. Adult patients often die from severe progressive muscle weakness, swallowing difficulties, malnutrition, or respiratory failure due to aspiration pneumonia or recurrent lung infections.
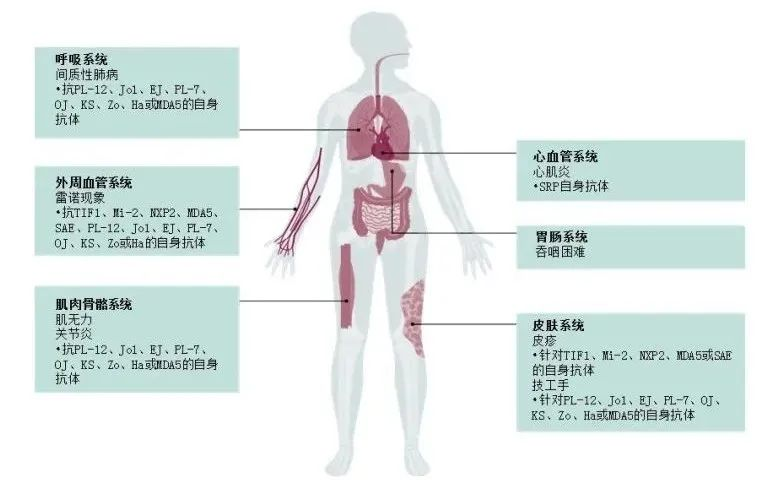
Laboratory testing is crucial for early diagnosis and treatment of the disease. Abnormal electromyography, inflammation in muscle biopsy, elevated muscle injury markers in the blood, presence of autoantibodies, and response to glucocorticoid therapy are indicators.IIM myositis-related autoantibody testing aids in early diagnosis and differential diagnosis and can provide strong evidence for guiding therapeutic medication.

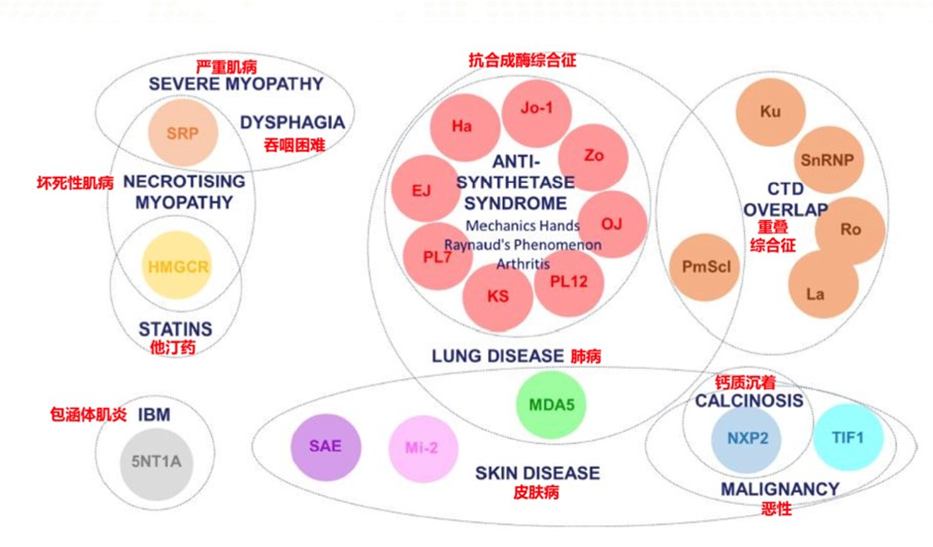
Clinical Significance of Autoantibodies is as follows
AntiJo-1 Antibody: Has strong specificity for diagnosing polymyositis and dermatomyositis, with a positive rate of about25% in polymyositis and7.1% in dermatomyositis. In patients with PM/DM with interstitial lung disease, the positive rate can be as high as60%. Typical symptoms of patients positive for antiJo-1 include polyarthritis, joint pain, non-invasive degenerative arthritis, tenosynovitis, pulmonary fibrosis, or pulmonary fibrosis, and scleroderma-related symptoms may also be occasionally associated. This syndrome is named antisynthetase syndrome, as other antibodies against aminoacyl-tRNA synthetases exhibit similar clinical symptoms, with75% having interstitial lung disease,70% having polyarthritis,60% having Raynaud’s phenomenon,71% having mechanic’s hands,87% having fever, and occasionally associated with subacute onset and rapidly progressive hypoxemia, responding well to treatment but prone to relapse.
AntiPL-7 Antibody: Recognized as a serum marker antibody for polymyositis (PM) and dermatomyositis (DM), with a positive rate of3%~4% in myositis patients, holding significant clinical value for diagnosingPM/DM, mainly seen in the antisynthetase syndrome subtype of myositis.
AntiPL-12 Antibody: Also a serum marker antibody for polymyositis (PM) and dermatomyositis (DM), with a positive rate of3% in myositis patients, holding significant clinical value for diagnosingPM/DM, mainly seen in the antisynthetase syndrome subtype of myositis, and is rare in non-myositis patients.
AntiEJ Antibody: Anti-glycyl tRNA synthetase antibody, found in myositis, interstitial lung disease, arthritis, Raynaud’s disease, mechanic’s hands, and fever.
AntiSRP Antibody: Present in5% of Caucasian adult polymyositis/ dermatomyositis,8%~13% of African adult polymyositis/ dermatomyositis, and2% of JDM patients, mainly seen in IMNM. Associated diseases include necrotizing autoimmune myopathy.
AntiMi-2 Antibody: An anti-tRNA synthetase antibody that appears only in adultsDM, juvenile typeDM,PM/DM andPM patient serum, particularly highly specific forDM. The positive rate of this antibody in adult dermatomyositis is11%~59%, and in juvenile dermatomyositis (JDM) it is4%~10%. Myositis patients positive for antiMi-2 antibodies have relatively mild conditions and may present with joint pain, arthritis, Raynaud’s phenomenon, andILD among other clinical manifestations.
AntiMDA-5 Antibody: Anti-melanoma differentiation-associated gene5, commonly associated with dermatomyositis and interstitial lung disease. This antibody has high diagnostic value for rapidly progressive ILD related to myositis, with a sensitivity of77% (95%Cl,64%~87%) and specificity of86% (95%Cl,79%~90%), and an area under the curve of0.89 (95%Cl,0.63~0.98). Myositis patients positive for this antibody have poorer pulmonary disease outcomes and significantly lower cumulative survival rates compared to antibody-negative patients (P=0.007). Additionally, the positive rate of antiMDA5 antibodies shows regional differences, with the positive rate in the Chinese population significantly higher than that in the Japanese population.
AntiTIF1-γ Antibody: Serum anti-transcription intermediary factor1-γ antibody, commonly seen in dermatomyositis and malignant tumors. It is a specific antibody for dermatomyositis, appearing in both adult and pediatric patients, with a frequency of13%~31% in adult polymyositis/ dermatomyositis and22%~29% in JDM. Since TIF1 protein plays a key role in tumor development, these antibodies may arise from abnormal anti-tumor immunity in the body.
AntiHMGCR Antibody: Hydroxymethylglutaryl-CoA reductase, associated with necrotizing autoimmune myopathy. The positive rate of this antibody is5.4%, most patients develop gradually, presenting with muscle weakness. This antibody can serve as both a diagnostic marker and a prognostic marker for the disease. The main clinical features of patients positive for antiHMGCR antibodies are muscle weakness and swallowing difficulties, and clinical screening for tumors and long-term immunosuppressive treatment should be conducted for these patients.
AntiSAE1/2 Antibody: The target antigen is small ubiquitin-like modifier-1 (SUMO-1) activating enzyme (SAE) heterodimer SAE1 and SAE2, which is commonly found in8% of dermatomyositis patients. Most positive patients first present with skin lesions, followed by severe swallowing difficulties.
AntiNXP-2 Antibody: Anti-nuclear matrix protein2 antibody, recently identified to be associated with adult dermatomyositis with severe skin calcification. Common diseases include dermatomyositis and malignant tumors. First reported in juvenile dermatomyositis, where it is associated with calcinosis, severe muscle weakness, polyarthritis, joint contractures, and intestinal vasculitis. The positive rate in the serum of children with juvenile myositis is23%~25%, and in adult myositis patients, it is1%~17%.
AntiOJ Antibody: Anti-isoleucyl tRNA synthetase antibody, clinical manifestations include interstitial lung disease, arthritis, Raynaud’s disease, and mechanic’s hands, less common in myositis, more common in dermatomyositis.
AntiKS Antibody: Aspartyl-tRNA synthetase, clinical manifestations include interstitial lung disease, arthritis, Raynaud’s disease, and mechanic’s hands, less common in myositis, some only accompanied by interstitial lung disease.
AntiZo Antibody: Anti-phenylalanyltRNA synthetase antibody, associated diseases includeAntisynthetase syndrome, namely anti-thyroid hormone (antisynthetase) syndrome.
AntiHA Antibody: Anti-tyrosyl tRNA synthetase antibody, associated diseases includeAntisynthetase syndrome, namely anti-thyroid hormone (antisynthetase) syndrome.
AntiSSA/Ro52kD Antibody: Anti-SSA antibody is mainly seen in primary Sjögren’s syndrome, with a positive rate as high as60%~75%. Additionally, antiSSA antibodies are often associated with subacute cutaneous lupus erythematosus, anti-nuclear antibody-negative lupus, neonatal lupus, etc. (SSA antibodies can cross the placenta and cause neonatal lupus syndrome).AntiSSA antibodies are associated with widespread photosensitive dermatitis symptoms.
AntiPM-SCl100 Antibody: Common in overlapping symptoms of polymyositis and systemic sclerosis, with a positive rate of50% in overlapping symptoms; it can also appear solely in polymyositis patients and diffuse scleroderma.
AntiPM-SCl75 Antibody: Common in overlapping symptoms of polymyositis and systemic sclerosis, with a positive rate of50% in overlapping symptoms; it can also appear solely in polymyositis patients and diffuse scleroderma.
AntiKu Antibody: Systemic sclerosis, polymyositis, and other connective tissue diseases such as rheumatoid arthritis(RA), mixed connective tissue disease(MCTD), Sjögren’s syndrome.
Main References:
1.Oldroyd AGS, Lilleker JB, Amin T, et al. British Society for Rheumatology guideline on management of paediatric, adolescent and adult patients with idiopathic inflammatory myopathy.Rheumatology 2022;61(5):1760-1768.
2. Guidelines for Diagnosis and Treatment of Idiopathic Inflammatory Myopathy, Chinese Rheumatology Society 2022.5
——The End——
Previous Highlights
【Introduction to New Projects in Medical Laboratory】–Combined Detection of Human SDC2 and TFPI2 Gene Methylation
【Introduction to New Projects in Medical Laboratory】–Detection of Hepatitis B Virus RNA
【Introduction to New Projects in Laboratory】—Erythropoietin (EPO) Testing
Introduction to New Projects in Medical Laboratory—Detection of 5 Items of Intestinal Carbapenemase Genes
【Introduction to New Projects in Laboratory】–Detection of Programmed Cell Death Protein-1 (PD-1)
All images in the text are copyrighted by their authors. If there is any infringement, please contact for removal.