Introduction by Good Doctor
The adenoid, also known as the pharyngeal tonsil, is located at the junction of the nasopharynx and the posterior wall of the pharynx. Like the tonsils, it is a part of the lymphatic tissue and plays an important role in the immune function of the body. The ear, nose, and throat are interconnected, and the adenoid is at the center of these interconnected pathways. In children, the nasopharyngeal cavity is relatively small, and when pharyngeal infections and repeated inflammatory stimuli occur, pathological hyperplasia occurs, referred to as adenoid hypertrophy.

The diagnosis of adenoid hypertrophy should be based on a comprehensive assessment of clinical history, nasal endoscopy, or imaging examinations. For infants and toddlers who are difficult to cooperate with nasal endoscopy and imaging examinations, clinical history analysis and the physician’s experience are very important, as most diagnoses can rely on symptoms and signs. For preschool children who can cooperate with examinations, nasal endoscopy or imaging examinations should be relied upon for confirmation. Regarding the diagnostic methods for adenoid hypertrophy, since CT and X-ray examinations can affect children, it is recommended that children over 5 years old should be diagnosed through nasal endoscopy. In the diagnosis of adenoid hypertrophy, the most important thing is to identify the cause of the hypertrophy, as only by identifying the cause can targeted treatment be carried out, which is key to the success of non-surgical treatment.
1. Anatomy of the Adenoid
The adenoid, also known as the adenoid tissue, is a mass of lymphatic tissue located at the top of the nasopharynx, at the base of the sphenoid bone and the external slope of the occipital bone. (It has no lymphatic drainage, and the lymphoid mucosal epithelium covering its surface has an immune barrier function, producing T and B lymphocytes.) It exists at birth and gradually grows, reaching its maximum size around 5-6 years of age, and gradually degenerates and atrophies after 10 years. The adenoid, along with the palatine tonsils, lingual tonsil tissue, and the lymphatic tissue of the posterior pharyngeal wall, forms the pharyngeal lymphatic ring, which is the first line of defense for the respiratory tract.


2. Causes
Children are prone to acute rhinitis, acute tonsillitis, and influenza. If these occur repeatedly, the adenoid can rapidly hypertrophy, exacerbating nasal obstruction and hindering nasal drainage. The secretions from rhinitis and sinusitis further irritate the adenoid, creating a vicious cycle. This condition is more common in children and often coexists with chronic tonsillitis.
3. Symptoms
(1) Ear Symptoms
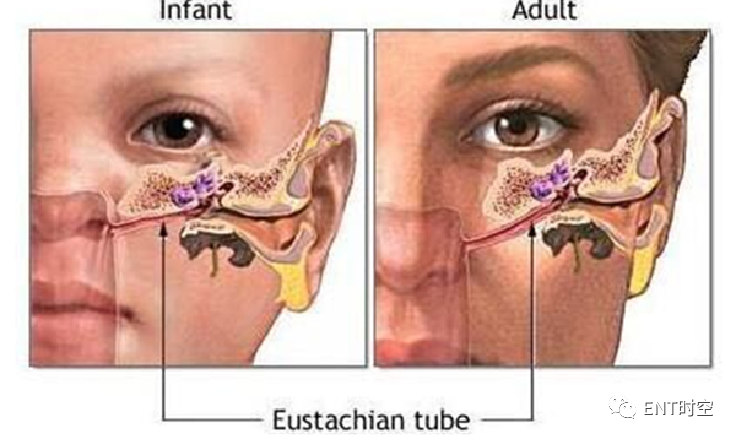
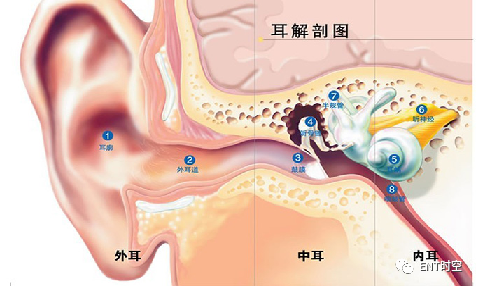
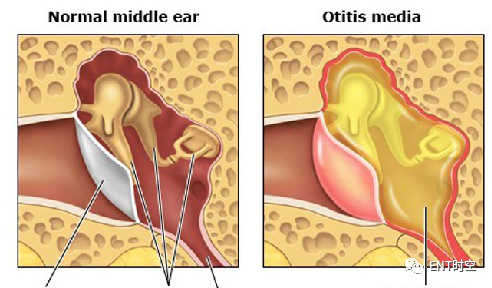
Obstruction of the eustachian tube orifice leads to serous otitis media, resulting in hearing loss and tinnitus.
Mechanism (4 points):
1. Mechanical obstruction or dysfunction of the eustachian tube. The eustachian tube may be compressed and obstructed by the hypertrophied adenoid, causing negative pressure in the tympanic cavity and resulting in mucosal effusion;
2. Eustachian tube reflux. The enlarged adenoid can obstruct the choana, leading to increased pressure in the nasopharynx during swallowing, causing pharyngeal secretions to reflux into the middle ear;
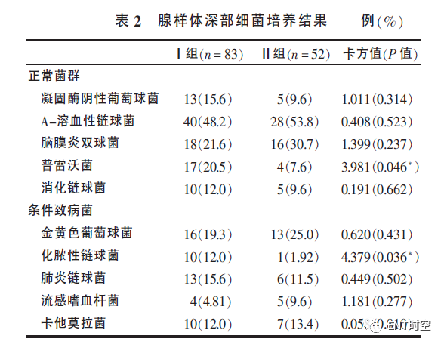
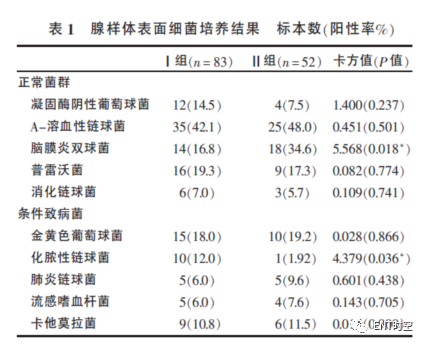
3. The adenoid serves as a reservoir for bacteria. Various pathogens, including bacteria, chlamydia, and viruses, can be found in the effusion from the middle ear;
4. Abnormal immunity of the adenoid, including local immune abnormalities and dysfunction. The immune dysfunction of the adenoid makes the nasopharyngeal mucosa prone to infections and edema. Some scholars have confirmed that the adenoid can release inflammatory mediators, such as prostaglandins, histamine, leukotrienes, and platelet-activating factors, which can increase vascular permeability, causing edema of the eustachian tube and middle ear mucosa, leading to SOM.

som
Impedance audiometry is an objective method to assess middle ear function. Type B tympanograms often indicate a large or viscous amount of effusion in the tympanic cavity, while Type C often indicates the presence of both gas and liquid in the tympanic cavity, indicating eustachian tube dysfunction.
(2) Nasal Symptoms
Often coexisting with rhinitis and sinusitis, symptoms include nasal congestion and rhinorrhea. Speech may have a nasal quality, and during sleep, snoring occurs, with severe cases presenting with sleep apnea.

 (3) Pharyngeal, Laryngeal, and Lower Respiratory Tract SymptomsDue to secretions flowing down and irritating the respiratory tract mucosa, it often causes nighttime coughing and is prone to bronchitis.(4) Adenoid FaciesLong-term mouth breathing can lead to abnormal facial bone development, elongated jaw, high-arched palate, malocclusion, protruding upper incisors, thick lips, lack of expression, resulting in what is known as “adenoid facies.”
(3) Pharyngeal, Laryngeal, and Lower Respiratory Tract SymptomsDue to secretions flowing down and irritating the respiratory tract mucosa, it often causes nighttime coughing and is prone to bronchitis.(4) Adenoid FaciesLong-term mouth breathing can lead to abnormal facial bone development, elongated jaw, high-arched palate, malocclusion, protruding upper incisors, thick lips, lack of expression, resulting in what is known as “adenoid facies.”

(5) Systemic SymptomsChildren may exhibit anorexia, vomiting, digestive disorders, leading to malnutrition. Due to respiratory difficulties and insufficient lung expansion, chest deformities may occur. Nighttime breathing difficulties can keep children in a state of chronic hypoxia, leading to endocrine dysfunction and growth and developmental disorders. Parents may notice symptoms such as inattention, mood swings, night terrors, bruxism, night sweats, and bedwetting.Adenoid hypertrophy is one of the most common causes of obstructive sleep apnea hypopnea syndrome (OSAHS). Loud snoring and breath-holding during sleep are the two main symptoms, while mouth breathing, excessive sweating during sleep, morning headaches, daytime sleepiness, and learning difficulties are also common symptoms.
4. Major Hazards
1. Adenoid facies2. Prone to bronchitis 3. Can cause mental fatigue and sluggish response in children4. Affects children’s growth and development
5. Diagnosis




Nasal Pharynx Lateral X-ray
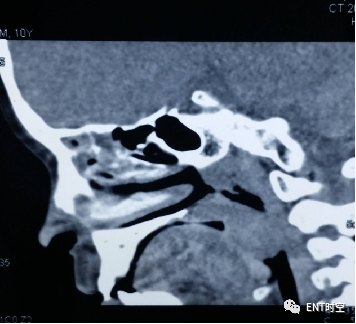
Using lateral projection of the nasopharynx, instruct the patient to inhale, slightly raise the chin to reduce the overlap of the mandible with the nasopharynx. The requirements for the lateral X-ray of the nasopharynx are: the X-ray must be taken during inhalation, as the soft palate is at its lowest position during inhalation, maximizing the anteroposterior diameter of the nasopharynx. The narrowing of the nasopharynx during exhalation, when the soft palate is raised, is a false appearance.
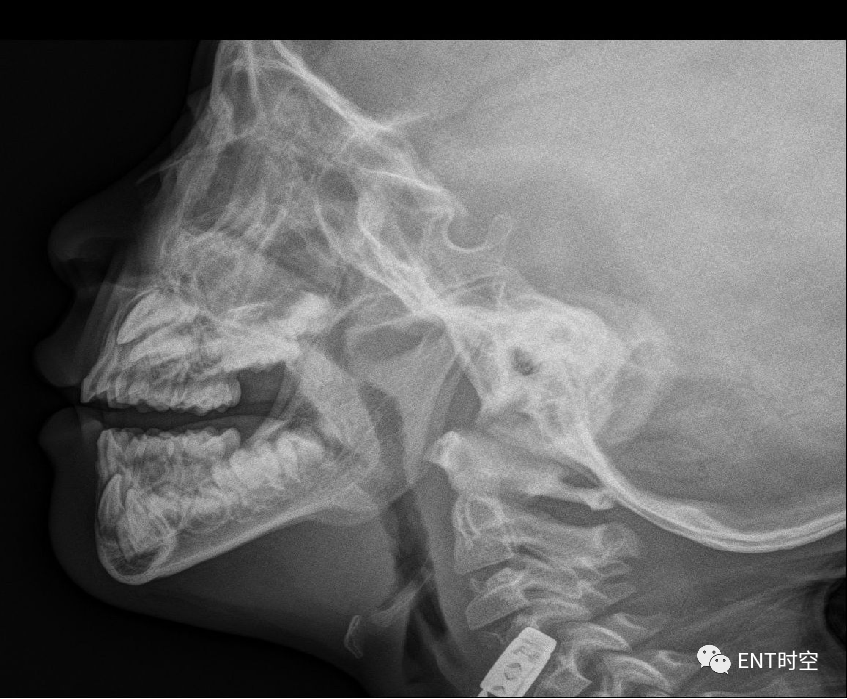
X-ray findings: The soft tissue of the posterior wall of the nasopharynx shows varying degrees of thickening, protruding into the nasopharynx, appearing arc-shaped or hill-like, with clear boundaries, compressing and narrowing the nasopharynx to varying degrees.
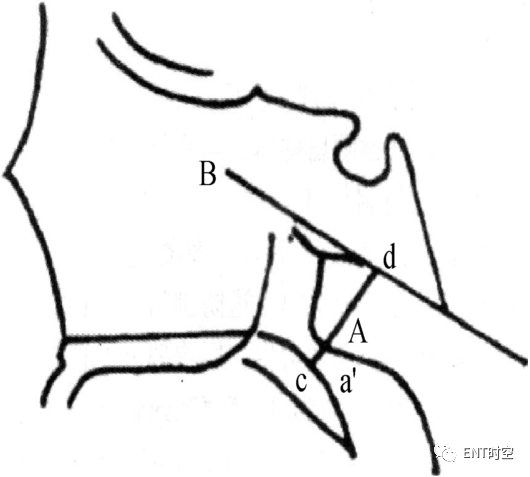
Using the method employed by Li Donghui et al., a line B is drawn along the external slope of the occipital bone, and a perpendicular line a’d is drawn from the most protruding point of the adenoid (the narrowest point of the airway) to line B, which represents the thickness of the adenoid (defined as value A). The line cd, which extends from a’d to the junction of the nasopharynx and the palate, represents the width of the nasopharynx at the most protruding point of the adenoid (defined as value N). The A/N ratio represents the ratio of adenoid thickness to nasopharyngeal width.
X-ray Diagnosis Criteria for Adenoid HypertrophyNormal adenoids appear as a soft tissue shadow with a narrow anterior and a wide posterior edge at the posterior wall of the nasopharynx, with a smooth surface. Luo Kaiyi et al. reported that thickening of the soft tissue of the posterior wall of the nasopharynx exceeding 13mm is significant for diagnosis; Zhang Baohua et al. found that an A/N ratio ≤ 0.66 is normal, 0.66 < A/N < 0.75 indicates moderate hypertrophy, and A/N ≥ 0.75 indicates severe hypertrophy. FUJIOKA et al. suggested that an A/N ratio greater than 0.59 indicates adenoid enlargement; some scholars also classify adenoid hypertrophy as grade I when it exceeds one-third of the airway, grade II when it exceeds two-thirds, and grade III when it nearly completely obstructs the airway. Based on previous research results, an A/N ratio > 0.60 is diagnosed as adenoid hypertrophy, with 0.60 < A/N ≤ 0.70 indicating mild hypertrophy, 0.70 < A/N ≤ 0.80 indicating moderate hypertrophy, and A/N > 0.80 indicating severe hypertrophy.
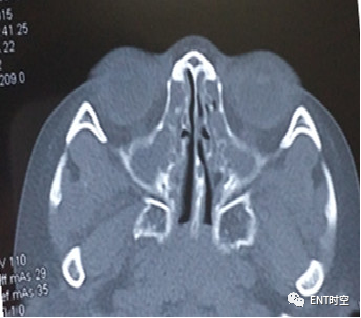
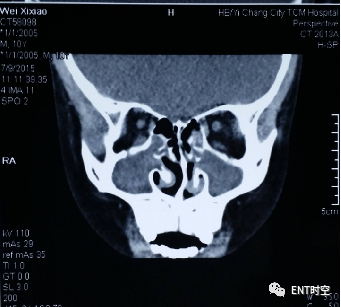
AH combined with CRS
6. Treatment
(1) Non-Pharmacological TreatmentPay attention to nutrition, prevent colds, enhance the body’s immunity, and actively treat primary diseases. As children grow older, the adenoid will gradually atrophy, and the condition may improve or symptoms may completely disappear.(2) Pharmacological TreatmentSome children often have rhinitis and sinusitis. After appropriate treatment, nasal ventilation improves, and clinical symptoms can be alleviated. Control nasal sinus and nasal cavity inflammation
- Oral medications (antibiotics, antihistamines, mucolytics, traditional Chinese medicine)
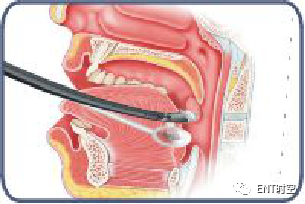
- Negative pressure replacement
- Inhalation therapy
- Corticosteroids
(1) Goldbart (PEDIATRICS USA): In children with sleep-disordered breathing, antibodies to leukotrienes (LTs) in the lymphatic tissue of the upper airway are elevated. Leukotriene receptor antagonists can bind to leukotriene receptors, thereby inhibiting the non-specific inflammatory response of the adenoid, causing it to shrink. Montelukast sodium chewable tablets (Singulair) by Merck, UK, for children over 2 years old.(2) The use of corticosteroids can bind to corticosteroid receptors in the adenoid, inhibiting the activity of lymphocytes, reducing inflammatory responses in the nasal cavity and nasopharynx, and modulating the bacterial colonies of the adenoid, leading to a reduction in adenoid tissue. PEDIATRICS USA
- Affect the synthesis and release of inflammatory mediators by antagonizing early inflammatory responses in the nasal cavity, such as histamine, bradykinin, and prostaglandins. Control nasal inflammation, alleviating symptoms such as nasal congestion, sneezing, and rhinorrhea.
- By regulating cytokines, eosinophils, and neuropeptides, reduce the number of lymphocytes involved in the immune response, controlling chronic inflammation in the nasal cavity and nasopharynx.
- Promote the synthesis of intracellular anti-inflammatory proteins.
Corticosteroid Equivalence
- Dexamethasone 0.75mg = Prednisone 5mg = Methylprednisolone 4mg = Hydrocortisone 20mg;
- Inhaled corticosteroids:Beclomethasone 25 = Hydrocortisone 20 = Prednisone 5 = Methylprednisolone 5 = Methylprednisolone 4 = Triamcinolone 4 = Betamethasone 0.8 = Dexamethasone 0.75 = Clobetasol 0.5
- Dipropionate beclomethasone 1000ug = Budesonide 800ug = Fluticasone propionate 500ug Example: 5mg DXM = 30mg pred = 40mg Methylprednisolone = 125mg Succinic Hydrocodone: 64ug*120

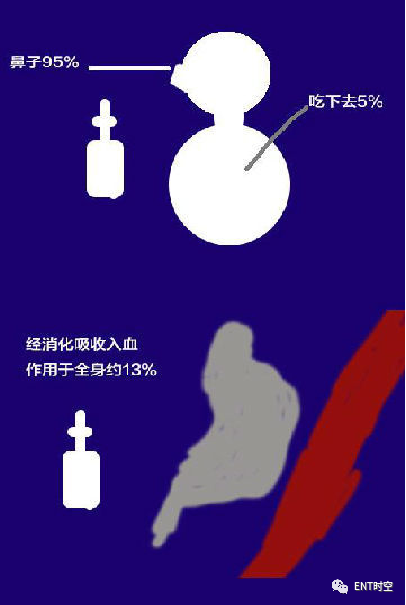

As shown in the above figure, the commonly used nasal corticosteroids have a dosage of about 1% of the oral or injected dosage, and the actual amount of the drug that can be utilized systemically is less than 0.1% of the dosage used. Therefore, nasal corticosteroids have been approved by the FDA for use in children over 3 years old, and current research data shows that using the recommended doses of nasal corticosteroids (continuously for two years) has no effect on children’s growth. Thus, the safety of nasal corticosteroids is very high. Conversely, the improvement in nasal congestion and quality of sleep has a positive effect on the growth of children.Nasal corticosteroids1. Triamcinolone, Budesonide (Rhinocort by AstraZeneca, Sweden) and Dipropionate Beclomethasone (Berkner by GlaxoSmithKline, UK): 6 years old2. Mometasone furoate (Nasonex by Merck, USA): 3 years old3. Fluticasone propionate (Flovent by GlaxoSmithKline, UK): 4 years oldPrinciples:1. The dosage should be strictly controlled,2. Choose the best efficacy—systemic bioavailability ratio, and select the minimum effective dose based on the degree of symptom relief. The specific method is: 2 sprays per nostril. Nasonex is once a day, while the other three are twice a day, with a total amount of 200 micrograms/day.(3) Surgical TreatmentAdenoidectomy can be performed simultaneously with tonsillectomy or separately; for those not suitable for surgery, radiation therapy may be considered (though rarely applied). In recent years, some have suggested using plasma therapy for adenoid hypertrophy, which is simple and minimally painful.(1) Timing of Surgery
- Children with repeated nasal congestion, snoring, and breath-holding, and breathing difficulties due to adenoid hypertrophy
- Children with serous otitis media complications
- Children with recurrent sinusitis and cough
- Adults with confirmed adenoid hypertrophy causing snoring
(2) Surgical Method SelectionA. Adenoid Curettage1. The surgery is relatively quick and can be performed under local anesthesia.2. The surgical field cannot be directly visualized, thus it is a blind curettage.3. Difficulties in hemostasis.4. Residual tissue may remain.5. Damage to surrounding tissues.6. Requires skilled assistance.

B. Endoscopic Electrocautery Removal1. The surgical field is clearly visible, allowing suction and cutting simultaneously.2. No damage to normal tissue, resulting in a neat and smooth wound.3. Avoids residual tissue.4. Hemostasis is easier, with less postoperative bleeding.C. Plasma Removal Method1. The probability of bleeding during and after surgery is lower; plasma is a non-contact hemostatic method that can only be used for surface hemostasis, with a coagulation depth of only 2-3mm. For deep hemostasis, bipolar electrocoagulation or electrosurgery is required.2. Complete removal, though there is a small chance of recurrence due to insufficient removal depth.3. Faster postoperative recovery.
Preoperative CarePatients often experience varying degrees of fear and anxiety before surgery, displaying agitation and emotional instability, such as crying and refusal to eat. Therefore, different intervention methods should be employed for children of different ages, providing encouragement and guidance to enhance the child’s sense of safety and trust, while also strengthening communication with family members to briefly explain the disease and the importance of treatment. Proper psychological care for family members is essential to gain their cooperation and support.

Postoperative CareBefore surgery, assist the doctor in conducting routine blood tests, liver and kidney function tests, chest X-rays, and ECGs. Explain the preoperative and postoperative precautions to the patient and family, instructing them to refrain from eating or drinking before surgery, and maintain oral hygiene. Administer atropine and hemostatic medications 30 minutes preoperatively. Patients under local anesthesia should be in a semi-reclined position, while those under general anesthesia should be in a lateral position to allow oral secretions to drain and for postoperative observation, ensuring airway patency. After awakening from general anesthesia, place the patient in a semi-reclined position to reduce head congestion and wound bleeding. Bed rest for 1-2 days postoperatively is recommended, followed by light activity, and avoiding vigorous exercise within one week after surgery.Postoperative pain is inevitable, but the duration varies. For pain relief, apply cold compresses to the neck, and encourage deep breathing and listening to music to distract the child’s attention. For postoperative mouth breathing, dry mouth, and pain, guide family members to provide small amounts of water frequently to moisten the throat and alleviate pain caused by dryness.Care for Fever: Monitor temperature changes postoperatively; a mild increase in temperature may occur within 1-2 days post-surgery. Most children experience varying degrees of fever, with temperatures between 37.3-38.0 degrees Celsius, indicating a reactive increase. Explain the reasons to the patient and family, encouraging the child to drink more water and fresh milk. If the temperature exceeds 38.5 degrees Celsius, inform the physician and check for local infections and complications.Observation of Bleeding: For patients who have not yet regained consciousness, pay special attention to frequent swallowing movements, as any indication of bleeding should be promptly reported to the physician for examination and management. Once awake, encourage minimal talking, avoid forceful coughing, and gently expel secretions, as the presence of blood-streaked secretions on the day of surgery is normal. On the second day post-surgery, the formation of a white protective membrane on the posterior pharyngeal wall should not be touched or removed to avoid bleeding.Dietary Guidance:Standard fasting for 4 to 6 hours postoperatively. During this period, the patient should lie flat with their head turned to one side, especially paying attention to frequent swallowing movements.The next day post-surgery, the diet should transition to cold liquid foods, with small, frequent meals, such as thin porridge, broken noodles, and steamed eggs, encouraging the patient to speak. On the third to seventh day post-surgery, dietary care should transition to warm and cool foods, advising family members to avoid very hot or hard foods to prevent burns or injury to the wound. Upon discharge, instruct to maintain a soft diet that is cool or warm, avoiding hard, spicy, fried, or excessively hot foods, and to limit the intake of fruits and juices to avoid irritating the wound and affecting healing, while ensuring adequate nutrition.Discharge Guidance:After discharge, instruct follow-up appointments at 1-6 months, guiding the child and family to exercise and enhance immunity. Avoid irritating foods, refrain from vigorous exercise, and prevent upper respiratory infections and colds.
Postoperative Complications
1. Primary Bleeding:
Within 24 hours post-surgery, if the child exhibits repeated swallowing movements and bleeding is noted in the mouth, or if bright red blood-tinged secretions are present in the throat or nose, it should be considered primary bleeding. This is often caused by residual adenoid tissue or vascular injury in the nasopharynx, premature eating, or coughing. Additionally, pressure from the surgical instrument may create an uneven force during hemostasis.
Estimation of Bleeding Volume
Gross calculation method: By observing changes in Hct before and during bleeding, the volume of blood loss can be estimated, which correlates positively with hb and hct, and is independent of body weight.
Calculation method:
Total blood loss = Preoperative blood volume * (Preoperative HCT – Postoperative HCT)
Preoperative blood volume = Preoperative body weight * 1000ml/kg * 8%
2. Secondary Bleeding:
Infection, coughing, or eating hard, brittle foods can cause secondary bleeding. 
Methods for Postoperative Hemostasis
- Mucosal constrictors and pressure hemostasis.
- Electrocautery hemostasis should be avoided too early, as it may cause excessive scab formation in the same area, leading to repeated scabbing and early detachment of the scab, resulting in bleeding.
- Ice compresses on the forehead and both sides of the neck.
- Principle: Hemostasis + Adequate Antibiotics
3. Infection:Primarily localized wound infections. Due to the unique location of the adenoid, bacteria can easily accumulate, and disinfection is difficult to achieve; the postoperative wound is directly connected to the outside environment, making it prone to infection.
-
Preoperative mouth rinses with antiseptic solutions.
-
Administer medications during the perioperative period.
-
Rinse mouth with antiseptic solution after eating.
-
Negative pressure replacement.
4. Eustachian Tube Injury:Caused by deviation of the curette from the midline, leading to scarring or narrowing of the orifice of the eustachian tube, resulting in functional impairment, subsequently causing hearing loss, effusion in the tympanic cavity, and serous otitis media. Regular follow-ups, medication treatment, and eustachian tube inflation can restore normal function in adulthood, with voice therapy for A-type.5. Pharyngeal Wall Injury and Mild Palate ParalysisCaused by rough handling, leading to tearing of the mucosa in the nasopharynx and oropharynx, leaving large scars that cause dryness in the oropharynx. Mild palate paralysis is rare and usually results from damage to the pharyngeal and palatal muscles.Tonsillectomy combined with adenoidectomy can result in nasopharyngeal reflux and pronounced open nasal speech. Postoperative instructions include blowing balloons and playing musical instruments.6. Asphyxia:A severe complication that can lead to death if not managed promptly, with removed adenoid tissue falling into the mouth or airway. The child’s head should be tilted downward to encourage coughing and expelling the tissue. If unsuccessful, laryngoscopy should be performed to retrieve the foreign body.7. Intracranial Complications:During adenoidectomy, non-degenerated craniofacial sacs may spread into the cranial cavity, leading to intracranial infections such as meningitis.8. Others:
- Loose or lost teeth: Long-term mouth breathing can lead to malocclusion, with uneven forces on the teeth from the mouth opener, causing them to loosen or fall out. Use gauze to protect and handle gently.
- Rotatory subluxation of the atlas-axis (atlantoaxial rotatory subluxation):
- Type 1 is common; rough handling during surgery or postoperative edema and infection can lead to atlantoaxial rotatory subluxation. Additionally, developmental abnormalities of the odontoid process in some children may also contribute to its occurrence. Therefore, timely control of pre- and post-surgical infections and gentle handling are essential, along with thorough preoperative communication.
- Once it occurs, continuous traction and cervical immobilization can restore normal function.
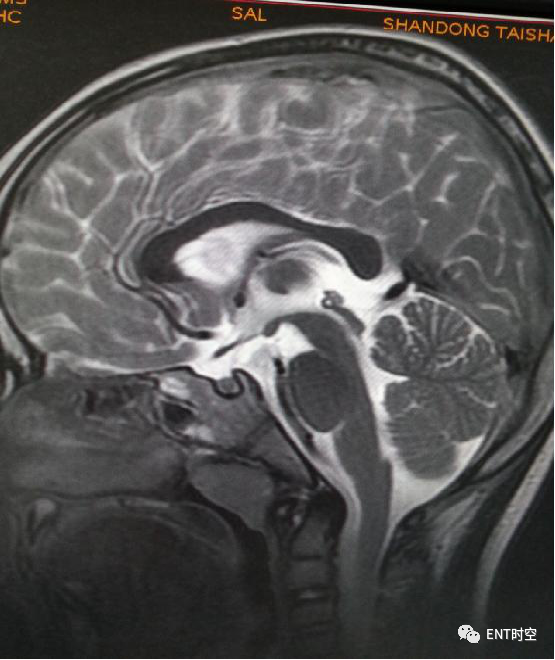
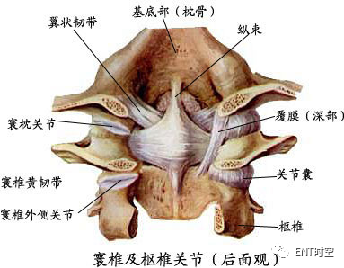
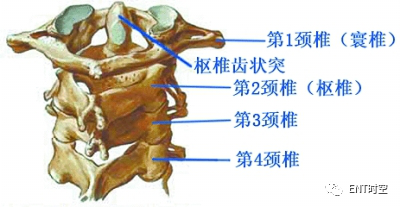
Atlas-Axis AnatomyAtlantoaxial subluxation refers to the subluxation of the atlas-axis joint. The atlas is the first cervical vertebra, ring-shaped, and articulates with the odontoid process of the axis through its posterior central notch, forming the atlantoaxial joint. The transverse ligament maintains the stability of the atlantoaxial joint, while the alar ligament assists the transverse ligament, and the blood supply to the atlantoaxial joint and its ligaments comes from the vessels of the nasopharynx.
Causes of Subluxation1. Excessive hyperextension during surgery, with the child struggling or turning their head too violently.2. Inflammation of the pharyngeal wall and occipital area may cause vascular congestion, ligament laxity, or detachment of ligament attachment points, weakening the supporting role of the ligaments, leading to atlantoaxial instability. Inflammation may also cause joint capsule edema, fluid accumulation, and local bone decalcification and loosening, leading to muscle spasms, ligament laxity, or detachment of ligament attachment points, resulting in pathological displacement between the atlas and axis. This type of secondary change due to nasopharyngeal inflammation is more common in children.Children with postoperative fever and significant bleeding areas have a higher incidence of cervical subluxation, indicating that local infection and repeated electrocautery hemostasis can alter atlantoaxial stability. Repeated hemostatic procedures not only increase the area of electrocautery but also deepen it, leading to local inflammatory responses, which may result in atlantoaxial instability. Postoperatively, if children maintain a certain position due to pain, it may predispose them to cervical subluxation. Excessive bleeding or oozing is often due to inexperienced use of cutting instruments, associated with rapid, excessive, or deep removal of tissue.Thus, proficient use of cutting instruments and judicious removal of adenoid tissue may be one strategy to reduce the incidence of cervical subluxation. Additionally, extending the duration of cotton ball compression during hemostasis may allow electrocautery to target single bleeding points, or even avoid electrocautery altogether. In the past four years, we have minimized the area of electrocautery during surgery, and no cervical subluxation has occurred since, suggesting that excessive electrocautery area may be related to cervical subluxation.

Type 1 Atlantoaxial Subluxation
Management Principles
-
Avoid excessive shoulder padding during surgery.
-
Postoperatively, avoid high pillows and prolonged fixed neck positions.
-
If subluxation occurs, continuous traction, cervical immobilization, and long-term intravenous antibiotics should be applied.
7. Impact of Surgery
1. Confirmed Impact of Adenoidectomy on Immunity in Children Under 6 Years Old.A. Studies show that children under 6 years old (with simple adenoid hypertrophy) have higher serum immunoglobulin (IgA, IgG) levels than preschool children, while IgM and IgE levels show no difference. This is considered due to the active synthesis and functional stage of immune tissues in preschool children, where the adenoid plays a role in generating antibodies in response to respiratory tract antigens.B. Research by Kiroglu et al. indicates that children with adenoid hypertrophy have significantly higher IgA and IgG levels than normal children, suggesting that the adenoid, as a specialized lymphatic tissue, participates in local immunity in the respiratory tract, generating IgA and IgG in response to repeated external bacterial stimulation, thus exerting anti-infection, neutralizing toxins, and immune-regulatory effects.C. Ivarsson’s research indicates that children with adenoid hypertrophy exhibit IgA and IgG antibody-secreting cells (ACE) in the nasopharyngeal mucosa in response to pathogenic antigens in the respiratory tract, contributing to immune defense.D. Amoros reported that serum IgA and IgG concentrations in children after adenoidectomy decreased but remained within the normal range for pediatric immunity. Some children showed a recovery of immunoglobulins starting four months post-surgery. Our results from measuring serum IgA, IgG, IgM, and IgE levels in children with adenoid hypertrophy suggest that post-surgery, IgA and IgG levels are lower than pre-surgery, although the incidence of recurrent respiratory infections has decreased, the severity of infections has worsened, with increased rates of bronchitis and bronchopneumonia.2. Some children undergoing adenoidectomy exhibit significant hyperplasia of nasopharyngeal lymphatic tissue, and even some previously non-hypertrophied tonsils begin to hypertrophy significantly after adenoid removal, making the outcomes of adenoidectomy less ideal. Therefore, the decision to perform adenoidectomy should consider the overall immune status of the child’s pharyngeal lymphatic ring, requiring more caution.Adenoid hypertrophy in children under 6 years old is often physiological, with lymphatic tissue development being most pronounced, actively participating in immune activities; thus, early removal of the adenoid should be avoided to prevent impairing this important immune organ. For older children, if severe nasal obstruction symptoms accompany conductive hearing loss, recurrent serous otitis media, recurrent nasopharyngeal inflammation, recurrent bronchitis, or even unexplained fever and OSAHS, leading to pathological changes in surrounding tissues or organs, adenoidectomy should be performed promptly. Welcome to Share the Article in Your Circle of Friends This article is compiled by the editor from sources including ENT Time Space, Qiao Zhi Pediatric Massage, Allergy Consultation Platform, etc. Unauthorized reproduction is prohibited. The views expressed in this article are solely those of the author and do not represent the official position of Good Doctor.We hope everyone makes rational judgments and applies the information appropriately. If there are any copyright issues, please contact us.
Welcome to Share the Article in Your Circle of Friends This article is compiled by the editor from sources including ENT Time Space, Qiao Zhi Pediatric Massage, Allergy Consultation Platform, etc. Unauthorized reproduction is prohibited. The views expressed in this article are solely those of the author and do not represent the official position of Good Doctor.We hope everyone makes rational judgments and applies the information appropriately. If there are any copyright issues, please contact us.
End
 Everyone is Watching
Everyone is Watching
Tonsillitis
Adenoid Hypertrophy
Pediatric Suppurative Tonsillitis
Image Description: Tonsil Enlargement Gradation!
Should Tonsils Be Removed or Not?
Should Chronic Tonsillitis Be Removed?
Three Simple Steps | Identify and Treat Pediatric Adenoid Hypertrophy
Imaging Findings and Diagnostic Criteria for Pediatric Adenoid Hypertrophy
The Most Comprehensive Compilation: Non-Surgical Treatment Methods for Adenoid Hypertrophy
The Complete Development Process of the Baby in the Uterus | 3D Images from 0 to 40 Weeks
Sore Throat and Fever ≠ Tonsillitis, Be Careful of These 4 Situations
How Much Do You Know About Non-Surgical Treatment Methods for Adenoid Hypertrophy?

