This article provides an in-depth interpretation of the “ASN Kidney Health Guidance on Potassium and Phosphorus Food Additives” (JASN 36: 2244-2258, 2025), developed by the American Society of Nephrology (ASN), aimed at providing scientific evidence and clinical guidance regarding potassium and phosphorus food additives in the management of chronic kidney disease (CKD). The guidance is based on a literature review and expert opinions, emphasizing the significant impact of food additives on potassium and phosphorus intake and proposing a tiered intervention strategy.
1.Introduction: The Core Role of Dietary Management inCKD and the Importance of Additives
1.1Background and Problem Statement
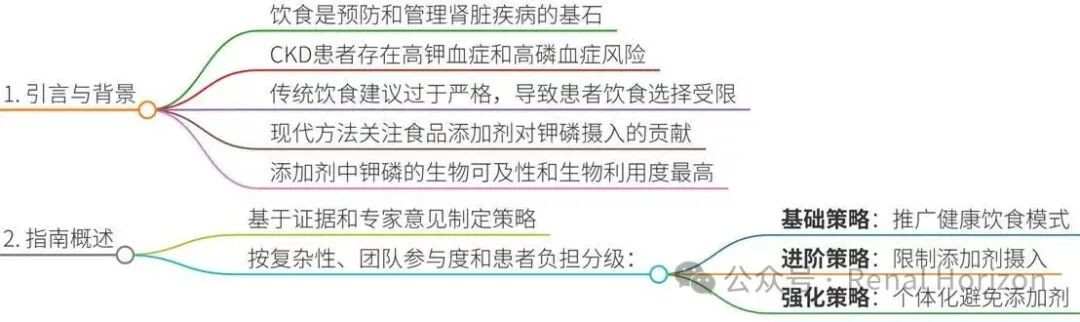
Diet is the cornerstone of preventing and managing kidney disease. As CKD progresses, patients face a high risk of hyperkalemia and hyperphosphatemia, which are key targets of nutritional management and can lead to adverse clinical outcomes.
Traditional recommendations overly restrict potassium- and phosphorus-rich foods, leading patients to feel “there’s nothing to eat“ and conflicting with healthy eating principles. Current management approaches have shifted to focus on the contributions of food additives, considering bioavailability (the amount of nutrients absorbed) and bioaccessibility (the amount available for biological processes after absorption).
1.2Definition and Role of Food Additives
Food additives are compounds added to food to achieve specific technical functions (such as improving sensory properties or extending shelf life). The US FDA has approved over 2500 various additives, among which potassium- and phosphorus-containing additives are widely used in processed foods.
Potassium additives (such as potassium chloride) partially replace sodium salt in sodium reduction strategies, which may be beneficial for cardiovascular health but pose a risk of hyperkalemia for CKD patients; phosphorus additives are ubiquitous and pose health concerns for CKD patients.
1.3The Necessity of Guidelines
Despite the ubiquity of additives, their uniform harm to CKD patients is not clearly defined, necessitating nuanced education based on individual patient characteristics. The ASN convened an expert working group to provide scientific guidance for kidney health professionals.
2.Guidance Overview: Tiered Strategies and Clinical Pathways
2.1Strategy Classification Based on Complexity and Patient Burden
Basic Strategies: Can be implemented by a wide range of healthcare professionals, focusing on healthy dietary patterns (such as balanced diets, limiting processed foods, controlling portions) to indirectly reduce exposure to additives. Suitable for most patients, with low information burden but potentially low compliance.
Advanced and Enhanced Strategies: Require detailed education from registered dietitians, including label reading and food substitutions, offering high flexibility but with a heavy information burden and requiring higher health literacy.
2.2Clinical Pathways for Risk Assessment and Intervention
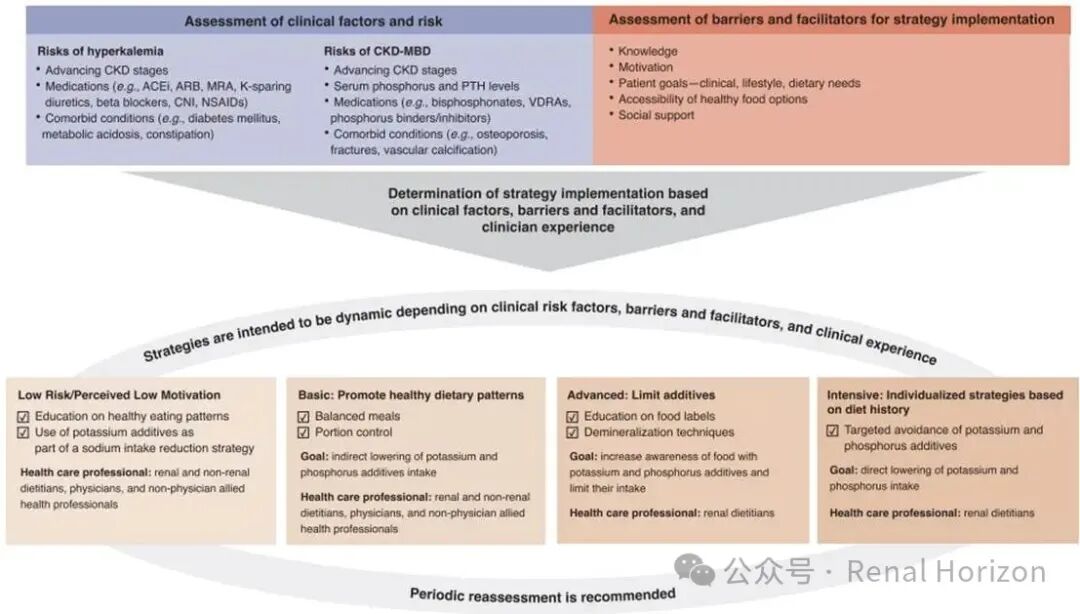
The guidelines propose clinical pathways (Figure 1), assessing hazard risks based on patient risk factors (such as eGFR, medication use, comorbidities) and matching appropriate strategies. The pathways integrate CKD-MBD indicators, medication impacts (such as ACEI, ARB) and individualized factors.
The pathways emphasize regular reassessment to adapt to CKD progression.
2.3Food Classification and Additive Definitions
The guidelines adopt the NOVA classification system (Table 1), defining unprocessed foods, minimally processed foods, processed foods, and ultra-processed foods. Additives are primarily found in processed and ultra-processed foods, with basic strategies encouraging minimally processed foods and advanced strategies directly targeting additives.
For example, ultra-processed foods are industrial formulations containing extracts or synthetic additives, with high concentrations of potassium and phosphorus additives.
3.Potassium Additives: Risks and Management Evolution
3.1Physiological Basis of Dietary Potassium and Potassium Homeostasis
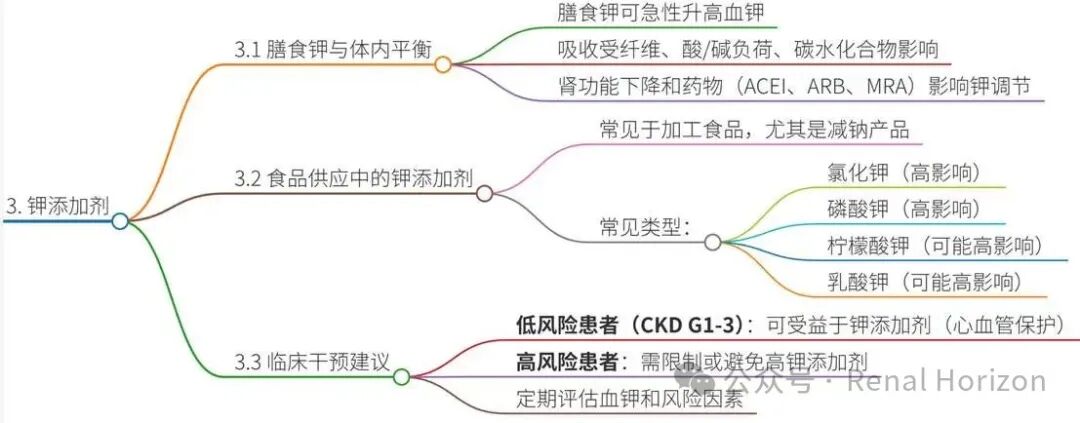
Potassium intake is associated with cardiovascular and kidney health, but CKD patients have impaired potassium regulation mechanisms (such as insulin and aldosterone-dependent cellular shifts, weakened renal excretion mechanisms). Medications (such as ACEI, ARB) further compromise potassium homeostasis, increasing the risk of hyperkalemia.
Potassium absorption is modulated by dietary components (such as fiber, acid load), and the anions in additives (such as chlorides, citrates) may affect bioavailability and cardiovascular physiology.
3.2Ubiquity of Potassium Additives in the Food Supply
In studies from the US and EU, 14.7%-37.6% of foods contain potassium additives. For example, potassium added to sodium-reduced meat products can reach 210-1500 mg/100g (5-38 mmol). USDA database analysis shows that menus containing potassium additives have a 66% higher potassium content than those without additives (1874 mg/day).
Common potassium additives include potassium chloride (sodium salt substitute), potassium phosphate, potassium citrate, and potassium lactate (Table 2), which may significantly affect serum potassium levels.
3.3Intervention Strategies: A Risk-Based Tiered Approach
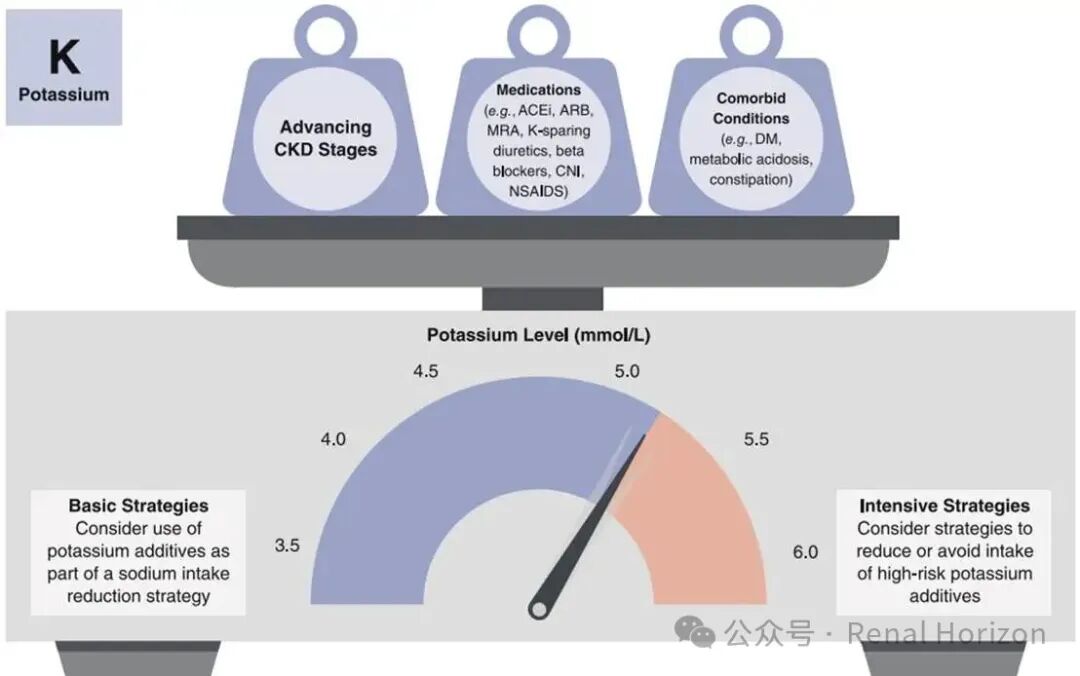
For low-risk patients in CKD G1-3, potassium additives may be safe and beneficial; however, as eGFR declines or medication use increases, risk-benefit ratios need to be reassessed. Figure 3 illustrates factors determining intervention intensity, such as serum potassium levels, medication use, and CKD stage.
Strategies are divided into basic, advanced, and enhanced (Table 3):
-
Basic Strategies: Balanced diet, home-cooked meals, substituting unhealthy foods (e.g., replacing processed meats with fresh meats), controlling portions.
-
Advanced Strategies: Avoid potassium-based salt substitutes, read labels to identify potassium additives, avoid injectable additives.
-
Enhanced Strategies: Individualized dietary analysis targeting high-risk additives (such as potassium chloride, potassium phosphate).
3.4Application of Food Literacy Models
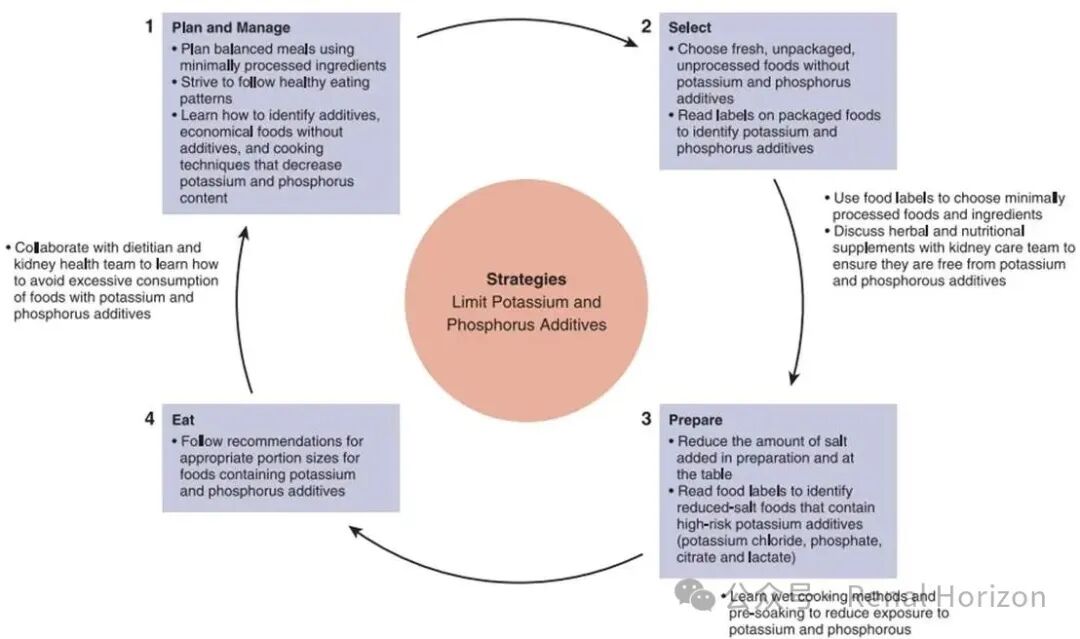
Figure 2 illustrates the food literacy conceptual model, emphasizing the application of strategies at the individual level, including planning, selecting, preparing, and consuming food to support patients in implementing restriction strategies.
4.Phosphorus Additives: Hidden Risks and Management Necessity
4.1The Importance of Phosphorus and Homeostatic Mechanisms
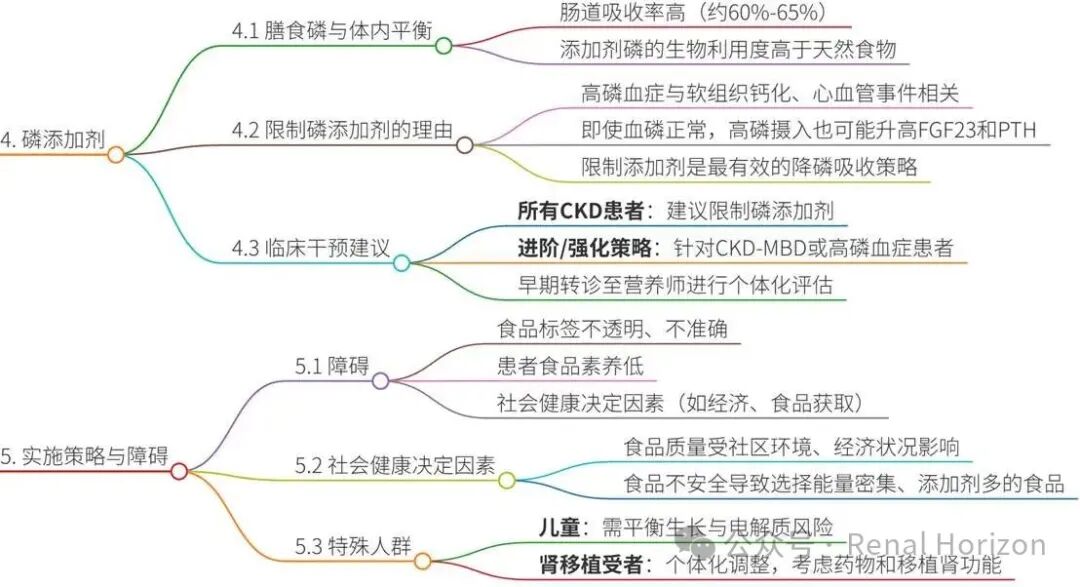
Phosphorus is an essential nutrient, but excess is associated with soft tissue calcification, cardiovascular disease, and bone disease. CKD patients commonly experience hyperphosphatemia in late stages, but even with normal serum phosphorus, high dietary phosphorus may stimulate FGF23 and PTH, leading to adverse outcomes.
Intestinal phosphorus absorption includes both active and passive pathways, with the bioavailability of inorganic phosphorus in additives (60%-65%) being higher than that of natural phosphorus (e.g., plant sources), with passive absorption dominating, making limiting additives an effective strategy.
4.2Health Risks and Evidence of Phosphorus Additives
Epidemiological studies show a correlation between high dietary phosphorus and mortality, but the relationship between serum phosphorus and dietary intake is weak. Clinical trials indicate that replacing foods with phosphorus additives with additive-free foods can improve hyperphosphatemia and reduce FGF23 and PTH.
Phosphorus additives are prevalent in processed foods, with 56% of products containing at least one phosphorus additive (such as sodium phosphate, modified starch). Additives contribute approximately 600-700 mg/day of phosphorus, but labeling information is incomplete, leading to underestimation of intake.
4.3Intervention Strategies: Early Intervention and Individualization
Even with normal serum phosphorus, CKD patients may benefit from reducing phosphorus additives to prevent mineral and bone disease (CKD-MBD). Figure 4 illustrates factors determining intervention intensity, such as CKD progression and CKD-MBD biomarkers.
Strategies are divided into basic, advanced, and enhanced (Table 4):
-
Basic Strategies: Balanced diet, home-cooked meals, substituting high-additive foods (e.g., replacing dark soda with light soda), controlling portions.
-
Advanced Strategies: Identifying additives containing the word “phosphorus“ (such as phosphates), avoiding injectable additives, and limiting phosphorus in supplements.
-
Enhanced Strategies: Identifying non-traditional additives (such as lecithin) and conducting individualized dietary record analysis.

5.Implementation Strategies: Multi-Faceted Barriers and Solutions
5.1Implementation Barriers
-
Label Opacity: Potassium and phosphorus additive labels are not required to quantify, and phosphorus additive names may not include the word “phosphorus“ (e.g., modified starch), making it difficult for patients and professionals to identify.
-
Low Food Literacy: Patients face challenges in dietary planning, label reading, and cultural differences. Social determinants (such as economic status, food access) affect dietary quality, with low-income groups relying more on processed foods.
-
Special Population Needs: Children need to balance growth with nutritional thresholds; kidney transplant recipients have unique risks due to medications (such as calcineurin inhibitors).
5.2Multi-Faceted Approaches to Solutions (Table 5)
-
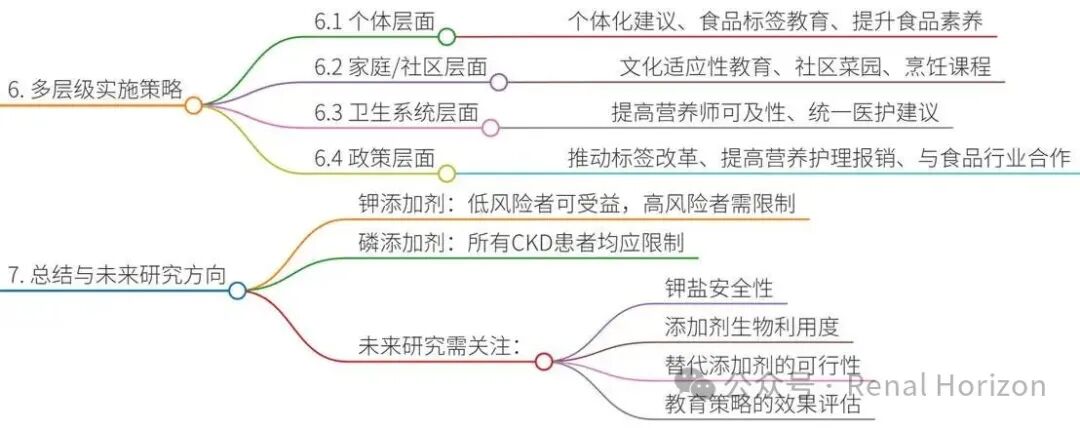
Individual Level: Provide practical advice, label reading education, and food literacy enhancement (such as cooking classes).
-
Family/Community Level/Community Level: Culturally adaptive education, community gardens, access to affordable foods.
-
Healthcare System Level: Early referral to dietitians, unified information dissemination, training healthcare professionals.
-
Policy Level: Advocate for label reform, improve reimbursement for nutritional care, collaborate with food manufacturers to develop alternative additives.
5.3Future Research Directions
-
Randomized controlled trials are needed to evaluate the efficacy of educational strategies; determine the safety of potassium salts; study the bioavailability of additives; analyze food potassium content; explore potassium-phosphorus alternative additives.
6.Conclusion and Insights
6.1Core Information of the Guidelines
Potassium additives may be beneficial for low-risk CKD patients, but high-risk patients should limit their intake; phosphorus additives offer no health benefits, and all CKD patients should restrict their intake. Strategies are based on risk stratification, from basic to enhanced.
6.2Clinical Significance
The guidelines provide practical tools (such as clinical pathways, label reading guides), emphasizing individualization and multidisciplinary collaboration. Implementation requires addressing social determinants to promote equity.
6.3Policy Significance
Calls for accurate labeling and policy support to protect vulnerable populations. The guidelines timely respond to the expansion of processed foods and the potassium salt replacement recommendations from WHO/FDA. This guidance modernizes the framework for CKD management through scientific evidence and tiered strategies, but successful implementation relies on patient education, system support, and policy reform. Future research will strengthen the evidence base and promote practical application.
Mind Map
Note: This article is for academic exchange only and not for any commercial use. Copyright belongs to the original authors and the original publication.
Biruete A, Anderson C, Bernier-Jean A, Clase CM, Clegg D, Crews DC, Denburg M, Hill Gallant KM, Gutierrez OM, Ix JH, Kienholz M, Lambert K, Lee SY, Liebman SE, Nelms CL, Palmer BF, Perwad F, Picard K, St-Jules DE, Terker AS, Uribarri J, Kovesdy CP; ASN Kidney Health Guidance Workgroup on Food Additives. ASN Kidney Health Guidance on Potassium and Phosphorus Food Additives. J Am Soc Nephrol. 2025 Nov 1;36(11):2244-2258. doi: 10.1681/ASN.0000000873. Epub 2025 Sep 18. PMID: 40965988; PMCID: PMC12591684.