The emergence of T-DXd represents a significant breakthrough in the treatment of HER2-positive and HER2-low expressing breast cancer. However, like any effective anti-cancer therapy, acquired resistance remains a major challenge affecting the long-term benefits for patients. Since the launch of Trastuzumab emtansine in 2013, five HER2 ADCs have been approved:Table 1: Approved HER ADCs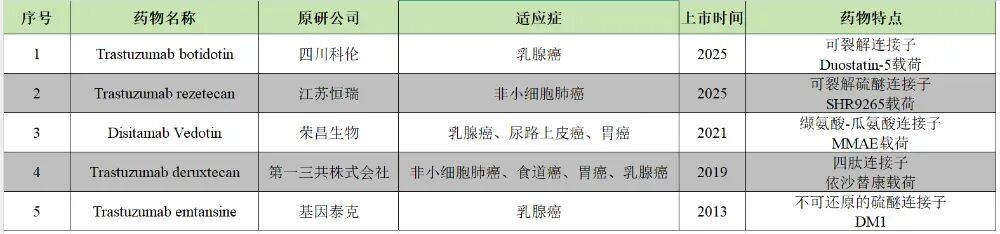 As clinical applications deepen, some shortcomings of ADCs, especially resistance, are gradually exposed. For example, Trastuzumab emtansine is prone to primary and acquired resistance, mainly due to compensatory activation of the HER2 signaling pathway and decreased antibody-dependent endocytosis efficiency.So, when developing a new ADC, should we take a fast-follow approach or base it on clinical shortcomings to create a first-in-class or better-in-class product? Today, we will analyze the resistance mechanisms of T-DXd (Trastuzumab Deruxtecan) and what preparations we need to make from the perspective of overcoming HER2 ADC resistance.Mutations in the HER2 gene binding domain lead to resistance.We conducted gene sequencing on 451 patients who had received T-DXd treatment and identified three noteworthy HER2 mutations:V597M and Q213*: These were found in pre-treatment samples, and these patients had poor responses to T-DXd, progressing quickly, indicating primary resistance.P593R: This mutation was found in samples from patients who responded to T-DXd for 32 months but progressed afterward, indicating acquired resistance.
As clinical applications deepen, some shortcomings of ADCs, especially resistance, are gradually exposed. For example, Trastuzumab emtansine is prone to primary and acquired resistance, mainly due to compensatory activation of the HER2 signaling pathway and decreased antibody-dependent endocytosis efficiency.So, when developing a new ADC, should we take a fast-follow approach or base it on clinical shortcomings to create a first-in-class or better-in-class product? Today, we will analyze the resistance mechanisms of T-DXd (Trastuzumab Deruxtecan) and what preparations we need to make from the perspective of overcoming HER2 ADC resistance.Mutations in the HER2 gene binding domain lead to resistance.We conducted gene sequencing on 451 patients who had received T-DXd treatment and identified three noteworthy HER2 mutations:V597M and Q213*: These were found in pre-treatment samples, and these patients had poor responses to T-DXd, progressing quickly, indicating primary resistance.P593R: This mutation was found in samples from patients who responded to T-DXd for 32 months but progressed afterward, indicating acquired resistance. Figure 1: HER2 Mutation SitesKnowing which mutation sites are involved, we then used molecular dynamics simulations to calculate the impact of these mutations on binding affinity. The results showed that the V597M mutation weakens the binding of HER2 to T-DXd.In MCF10A cells with low HER2 expression, we inserted either wild-type or mutant HER2. Western Blot and flow cytometry demonstrated that both wild-type and V597M mutant HER2 could express equal high levels of HER2 protein on the cell membrane after induction. This rules out the issue of protein expression levels; the problem lies in the “quality” of the protein.We labeled T-DXd with a dye that fluoresces in acidic environments, pHrodo. When the drug is endocytosed into acidic lysosomes, it emits red fluorescence. In cells expressing wild-type HER2, the drug endocytosis efficiency is very high; however, in cells expressing the V597M mutant, despite having a significant amount of HER2 on the membrane, the drug cannot enter.If we compare HER2 to a door lock, when the “lock” is functioning, the drug can enter smoothly; when the “lock” is broken, the drug is blocked outside.
Figure 1: HER2 Mutation SitesKnowing which mutation sites are involved, we then used molecular dynamics simulations to calculate the impact of these mutations on binding affinity. The results showed that the V597M mutation weakens the binding of HER2 to T-DXd.In MCF10A cells with low HER2 expression, we inserted either wild-type or mutant HER2. Western Blot and flow cytometry demonstrated that both wild-type and V597M mutant HER2 could express equal high levels of HER2 protein on the cell membrane after induction. This rules out the issue of protein expression levels; the problem lies in the “quality” of the protein.We labeled T-DXd with a dye that fluoresces in acidic environments, pHrodo. When the drug is endocytosed into acidic lysosomes, it emits red fluorescence. In cells expressing wild-type HER2, the drug endocytosis efficiency is very high; however, in cells expressing the V597M mutant, despite having a significant amount of HER2 on the membrane, the drug cannot enter.If we compare HER2 to a door lock, when the “lock” is functioning, the drug can enter smoothly; when the “lock” is broken, the drug is blocked outside.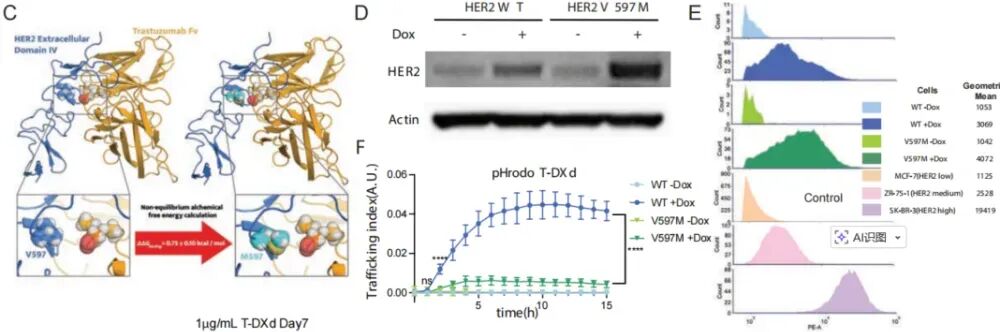 Figure 2: V597M Mutation Weakens HER2 Binding to T-DXdWithout the drug entering, it naturally cannot kill the cells. Cell viability assays clearly show that in cells expressing wild-type HER2, T-DXd strongly inhibits cell growth; whereas in cells expressing V597M or P593R mutants, T-DXd is almost ineffective.
Figure 2: V597M Mutation Weakens HER2 Binding to T-DXdWithout the drug entering, it naturally cannot kill the cells. Cell viability assays clearly show that in cells expressing wild-type HER2, T-DXd strongly inhibits cell growth; whereas in cells expressing V597M or P593R mutants, T-DXd is almost ineffective.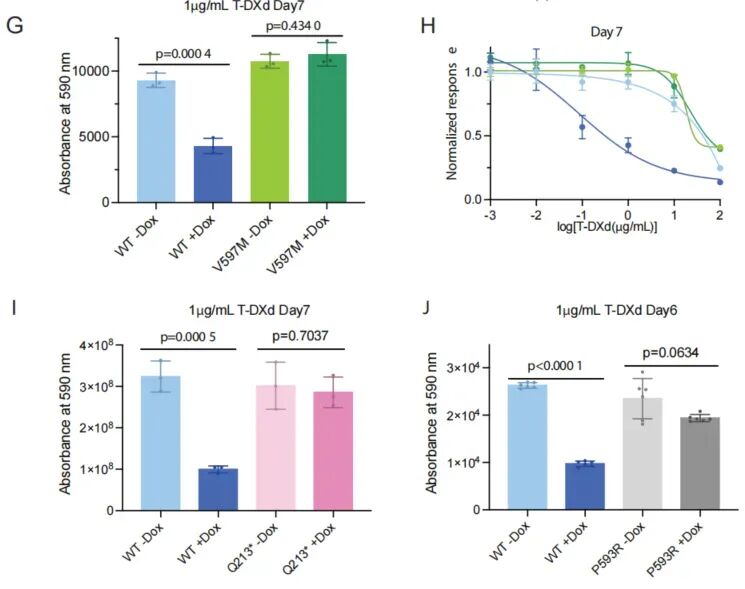 Figure 3: HER2 Mutation Sites Lead to Reduced Efficacy of T-DXdLoss of HER2 expression leads to resistance.This is a more common mechanism of resistance. If the first part is about the “lock being broken,” this part is about directly removing the “door” (HER2 protein).We analyzed 102 paired tumor samples before and after treatment and found a striking phenomenon: 49% of patients had significantly decreased HER2 protein levels in their tumors at disease progression; among them, more than half had completely lost HER2 expression.
Figure 3: HER2 Mutation Sites Lead to Reduced Efficacy of T-DXdLoss of HER2 expression leads to resistance.This is a more common mechanism of resistance. If the first part is about the “lock being broken,” this part is about directly removing the “door” (HER2 protein).We analyzed 102 paired tumor samples before and after treatment and found a striking phenomenon: 49% of patients had significantly decreased HER2 protein levels in their tumors at disease progression; among them, more than half had completely lost HER2 expression.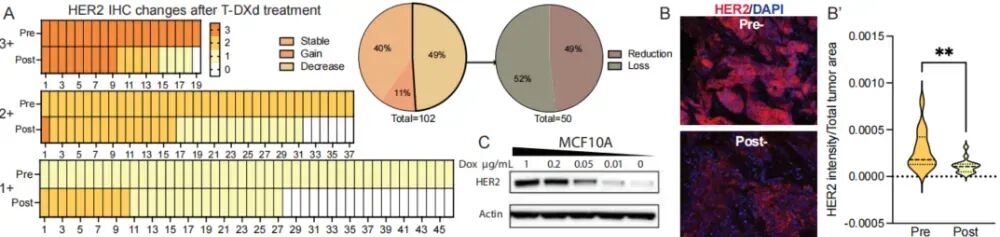 Figure 4: Loss of HER2 ExpressionWhy is this happening? Researchers constructed a very clever “inducible” cell model, MCF10A. By adding different concentrations of doxycycline, they can precisely control HER2 expression levels like a dimmer switch, from IHC 3+ (high) down to 2+, 1+, and all the way to 0.
Figure 4: Loss of HER2 ExpressionWhy is this happening? Researchers constructed a very clever “inducible” cell model, MCF10A. By adding different concentrations of doxycycline, they can precisely control HER2 expression levels like a dimmer switch, from IHC 3+ (high) down to 2+, 1+, and all the way to 0.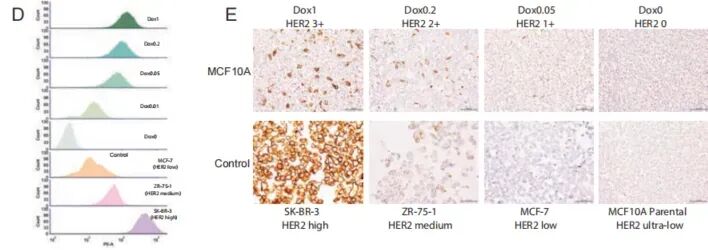 Figure 5: Construction of the MCF10A Cell ModelUsing pHrodo-labeled T-DXd again, the results were completely as expected: the higher the HER2 expression level, the stronger the drug endocytosis fluorescence signal; when HER2 expression dropped to 0, the endocytosis signal also became negligible. This directly proves that HER2 expression levels are positively correlated with T-DXd internalization efficiency.
Figure 5: Construction of the MCF10A Cell ModelUsing pHrodo-labeled T-DXd again, the results were completely as expected: the higher the HER2 expression level, the stronger the drug endocytosis fluorescence signal; when HER2 expression dropped to 0, the endocytosis signal also became negligible. This directly proves that HER2 expression levels are positively correlated with T-DXd internalization efficiency.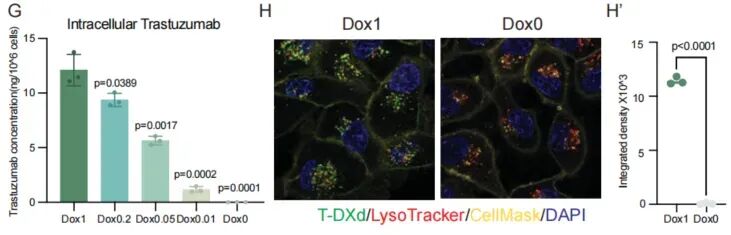 Figure 6: Correlation Between HER2 Expression and T-DXd Internalization EfficiencyUsing ELISA to directly detect intracellular T-DXd concentrations, the results again confirmed that as HER2 expression decreased, the amount of drug “eaten” by the cells significantly reduced. Through confocal microscopy, we directly observed that in cells with high and zero HER2 expression, the intracellular T-DXd levels were vastly different.
Figure 6: Correlation Between HER2 Expression and T-DXd Internalization EfficiencyUsing ELISA to directly detect intracellular T-DXd concentrations, the results again confirmed that as HER2 expression decreased, the amount of drug “eaten” by the cells significantly reduced. Through confocal microscopy, we directly observed that in cells with high and zero HER2 expression, the intracellular T-DXd levels were vastly different.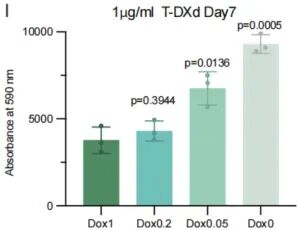 Figure 7: T-DXd Levels in Cells with High and Zero HER2 ExpressionAs HER2 expression levels decrease, the ability of T-DXd to inhibit cell growth sharply declines. The IC50 value changes from 0.06 μg/mL at high HER2 expression to 42.22 μg/mL at zero HER2 expression, indicating a more than 700-fold increase in resistance. This demonstrates in vitro that the loss of HER2 observed clinically is sufficient to cause complete resistance to T-DXd.
Figure 7: T-DXd Levels in Cells with High and Zero HER2 ExpressionAs HER2 expression levels decrease, the ability of T-DXd to inhibit cell growth sharply declines. The IC50 value changes from 0.06 μg/mL at high HER2 expression to 42.22 μg/mL at zero HER2 expression, indicating a more than 700-fold increase in resistance. This demonstrates in vitro that the loss of HER2 observed clinically is sufficient to cause complete resistance to T-DXd.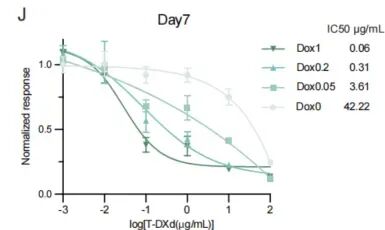
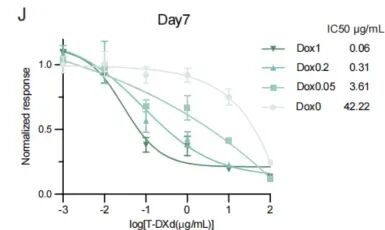 Figure 8: Loss of HER2 Leads to T-DXd ResistanceStrategies to Overcome Resistance—”Multi-Pathway Delivery”Since resistance arises because the HER2 pathway is blocked, what should we do? We can take another route or pursue multiple pathways simultaneously. Although tumor cells may lose HER2, they remain sensitive to the payload carried by T-DXd. The key issue is how to deliver the payload inside.In HER2-low expressing resistant cells, if we directly add a little bit of DXd payload, the cells can be killed. This indicates that the cells are afraid of the payload; they just dislike the “delivery” of T-DXd.If we choose another target, TROP2, with a payload similar to that of T-DXd, we can use the ADC—Datopotamab Deruxtecan. The efficacy of Dato-DXd is not affected by HER2 expression levels; it follows the TROP2 pathway. Low doses of T-DXd and low doses of Dato-DXd combined yield effects equivalent to or even superior to high doses of either drug alone. Why? Because combination therapy delivers the payload to the cells through both HER2 and TROP2 channels simultaneously, resulting in higher overall payload delivery efficiency.
Figure 8: Loss of HER2 Leads to T-DXd ResistanceStrategies to Overcome Resistance—”Multi-Pathway Delivery”Since resistance arises because the HER2 pathway is blocked, what should we do? We can take another route or pursue multiple pathways simultaneously. Although tumor cells may lose HER2, they remain sensitive to the payload carried by T-DXd. The key issue is how to deliver the payload inside.In HER2-low expressing resistant cells, if we directly add a little bit of DXd payload, the cells can be killed. This indicates that the cells are afraid of the payload; they just dislike the “delivery” of T-DXd.If we choose another target, TROP2, with a payload similar to that of T-DXd, we can use the ADC—Datopotamab Deruxtecan. The efficacy of Dato-DXd is not affected by HER2 expression levels; it follows the TROP2 pathway. Low doses of T-DXd and low doses of Dato-DXd combined yield effects equivalent to or even superior to high doses of either drug alone. Why? Because combination therapy delivers the payload to the cells through both HER2 and TROP2 channels simultaneously, resulting in higher overall payload delivery efficiency.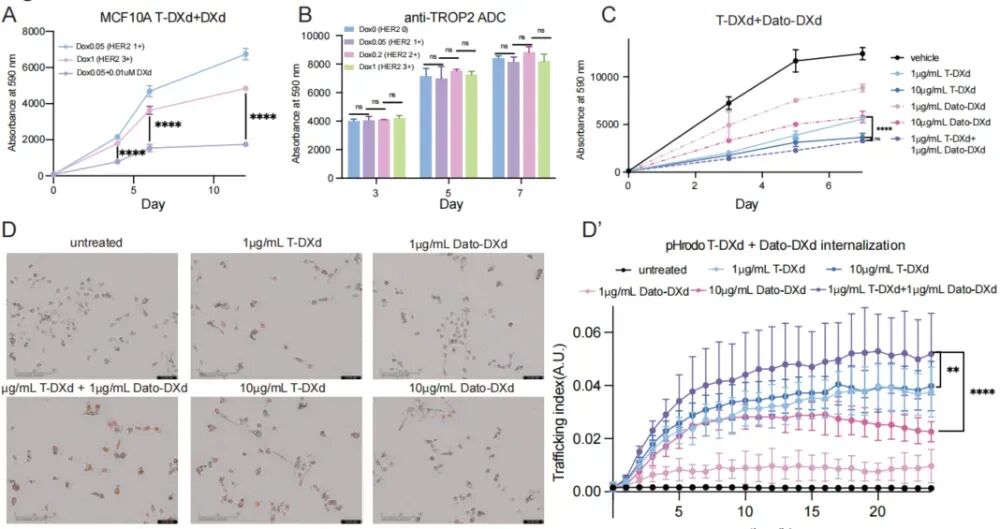 Figure 9: Combination of Dato-DXd and T-DXdAnimal model studies also support this: using T-DXd or Dato-DXd alone only slightly delays tumor growth, while low-dose combination therapy leads to significant tumor shrinkage, and the mice do not show significant weight loss, indicating manageable toxicity.ConclusionIn-depth analysis of resistance mechanisms: The two core mechanisms of clinical resistance to T-DXd—target mutations and target loss—both operate by impairing the initial steps of drug binding and internalization.Treatment strategy: The “multi-target ADC sharing payload” strategy has great clinical translational potential. In the future, the application of ADCs may no longer be a solo act; through clever low-dose combinations, we can enhance efficacy, overcome resistance, and reduce the toxicity associated with high doses of single agents, achieving an effect of “1+1 > 2.” For example, the HER2 & TROP2 dual-target ADCs RB-201 and Catenabio are currently in the research phase. Will they not develop resistance when used alone? We shall see! Furthermore, if we were to initiate a project for a HER2 ADC now, could we find breakthroughs by targeting HER2 mutation sites and dual-target ADCs?References:Chen W, et al. Trastuzumab Deruxtecan (T-DXd) Resistance via Loss of HER2 Expression and Binding. Cancer Discov.Burke CM, et al. Anti-tumor activity of trastuzumab deruxtecan in pediatric solid tumors with variable HER2 expression. Mol Cancer Ther.Wekking D, et al. Multidisciplinary clinical guidelines in proactive monitoring, early diagnosis, and effective management of trastuzumab deruxtecan (T-DXd)-induced interstitial lung disease (ILD) in breast cancer patients. ESMO Open.
Figure 9: Combination of Dato-DXd and T-DXdAnimal model studies also support this: using T-DXd or Dato-DXd alone only slightly delays tumor growth, while low-dose combination therapy leads to significant tumor shrinkage, and the mice do not show significant weight loss, indicating manageable toxicity.ConclusionIn-depth analysis of resistance mechanisms: The two core mechanisms of clinical resistance to T-DXd—target mutations and target loss—both operate by impairing the initial steps of drug binding and internalization.Treatment strategy: The “multi-target ADC sharing payload” strategy has great clinical translational potential. In the future, the application of ADCs may no longer be a solo act; through clever low-dose combinations, we can enhance efficacy, overcome resistance, and reduce the toxicity associated with high doses of single agents, achieving an effect of “1+1 > 2.” For example, the HER2 & TROP2 dual-target ADCs RB-201 and Catenabio are currently in the research phase. Will they not develop resistance when used alone? We shall see! Furthermore, if we were to initiate a project for a HER2 ADC now, could we find breakthroughs by targeting HER2 mutation sites and dual-target ADCs?References:Chen W, et al. Trastuzumab Deruxtecan (T-DXd) Resistance via Loss of HER2 Expression and Binding. Cancer Discov.Burke CM, et al. Anti-tumor activity of trastuzumab deruxtecan in pediatric solid tumors with variable HER2 expression. Mol Cancer Ther.Wekking D, et al. Multidisciplinary clinical guidelines in proactive monitoring, early diagnosis, and effective management of trastuzumab deruxtecan (T-DXd)-induced interstitial lung disease (ILD) in breast cancer patients. ESMO Open.
Disclaimer: This article is based on existing public data and literature reports and does not have any conflicts of interest with any organization or individual. For clinical medication, please refer to clinical authoritative guidelines or consult clinical doctors for treatment. It does not constitute any investment advice. If there are any copyright issues, please contact the medical academic within 30 days of publication. Unauthorized reproduction of original content on other platforms is prohibited.©2021 Medical Academic. All rights reserved.