Click the “Chinese Journal of Practical Surgery” above to subscribe!


Professor Zhou Weiping
[Cite This Article] Gu Fangming, Zhou Weiping. Imaging Diagnosis of Intrahepatic Cholangiocarcinoma [J]. Chinese Journal of Practical Surgery, 2020, 40(6): 738-740.
Imaging Diagnosis of Intrahepatic Cholangiocarcinoma
Gu Fangming, Zhou Weiping
Chinese Journal of Practical Surgery, 2020, 40(6): 738-740
Abstract
The rapid development of imaging technology has improved the accurate diagnosis and staging of intrahepatic cholangiocarcinoma (ICC), providing a basis for precise clinical treatment of ICC. Ultrasound examination is the first-line screening method for ICC, which is simple and economical, but lacks specificity. CT and MRI are still the main imaging methods for diagnosing ICC. MRI has advantages such as good soft tissue resolution and multi-directional imaging, while magnetic resonance cholangiopancreatography (MRCP) technology can further clarify the relationship between the tumor and surrounding bile ducts. MRI generally has a higher diagnostic accuracy for ICC compared to CT, but CT is more intuitive in displaying ICC related to intrahepatic bile duct stones. PET-CT combined with CT and MRI can improve the diagnostic accuracy of ICC and compensate for the shortcomings of CT and MRI in diagnosing regional lymph node metastases and distant metastases.
Funding: National Natural Science Foundation Innovative Group (No. 81521091); National Natural Science Foundation General Project (No. 81972704)
Author Affiliation: Department of Hepatobiliary Surgery, Navy Medical University, Shanghai 200438
Corresponding Author: Zhou Weiping, E-mail: [email protected]
Intrahepatic cholangiocarcinoma (ICC) originates from the epithelial cells of the secondary bile ducts and above in the liver and is the second largest primary malignant tumor of the liver, following hepatocellular carcinoma, with an increasing incidence year by year. ICC is commonly classified into four types: mass-forming, intraductal growing, periductal infiltrating, and mixed type (a combination of mass-forming and periductal infiltrating), with mass-forming and mixed types accounting for approximately 90% of ICC. Due to the lack of specific clinical symptoms, early diagnosis of ICC remains challenging. Even with curative surgery, the 5-year survival rate post-operation is still low. Currently, with the rapid development of imaging technology, the accurate diagnosis and staging of ICC have been greatly improved, providing a basis for precise treatment of ICC. This article will focus on the imaging diagnosis of mass-forming ICC.
1 Ultrasound Imaging Characteristics
Ultrasound examination is the first-line screening method for ICC, which is simple and economical. The ultrasound images of ICC often show irregular shapes with homogeneous low-echo lesions. As the tumor can compress or obstruct surrounding bile ducts, leading to bile accumulation, ultrasound often shows a ring or irregular hypoechoic area around the tumor. The specificity of ultrasound alone for diagnosing ICC is not high, and it is still challenging to distinguish ICC from hepatocellular carcinoma, liver abscess, etc. Ultrasound diagnosis is significantly influenced by the operator’s experience and equipment quality, as well as the tumor’s position and morphology, but clinically, ultrasound-guided multifocal puncture biopsy can be used to obtain a definitive pathological diagnosis. Additionally, contrast-enhanced ultrasound can show the tumor’s blood supply perfusion, which can assist in diagnosing ICC, but it also lacks specificity.
2 CT and MRI Characteristics
CT and MRI are still the main imaging methods for diagnosing ICC. The CT scan of ICC often shows uneven low-density lesions, with enhancement around the tumor in the arterial phase and sustained enhancement in the portal venous phase, sometimes with centripetal mild to moderate enhancement. The MRI characteristics of ICC typically show uneven low signals on T1-weighted imaging and uneven high or slightly high signals on T2-weighted imaging, with enhancement patterns similar to those of CT. The enhancement characteristics of ICC are primarily related to the infiltrative growth pattern of ICC. The tumor periphery consists of a large number of tumor cells and a small amount of fibrous tissue, resulting in relatively abundant blood supply, hence the enhancement in the arterial phase; while the tumor interior mainly consists of fibrous tissue, with some necrotic areas, causing the contrast agent to enter the fibrous stroma slowly, leading to sustained enhancement in the portal phase and delayed enhancement in the delayed phase. Both enhanced CT and MRI can clarify the relationship between the tumor and the hepatic hilum and peripheral vessels, providing a basis for clinical judgment on whether the lesion can be completely resected.
Some ICC cases are caused by long-term intrahepatic bile duct stones, and CT is relatively easier to distinguish than MRI. ICC often coexists with small foci adjacent to the main tumor, and MRI, especially in the T2-weighted phase, can display these more clearly than CT. The DWI sequence of MRI also aids in the detection of ICC and intrahepatic metastatic lesions. Reports suggest that enhanced MRI with gadoxetic acid can better detect small intrahepatic lesions of ICC.
The “shrinkage of the liver capsule” sign is a characteristic imaging manifestation of ICC, which is related to the infiltrative growth of the tumor, the presence of a large amount of fibrous tissue inside, and the pulling effect on the liver capsule. Local dilation of the bile duct around the tumor is also an important feature of ICC, often due to the tumor growing around or along the bile duct, leading to local narrowing and dilation of the bile duct lumen. Magnetic resonance T2-weighted imaging shows bile duct dilation more clearly than CT. The MRCP technique can display the entire bile duct tree, providing imaging evidence for distinguishing between extrahepatic and hilar bile duct tumors, in addition to clarifying the relationship between the tumor and surrounding bile ducts.
3 PET-CT Characteristics
PET-CT examination is a new radiological technology that combines anatomical and functional imaging. It reflects both morphological changes of the tumor and its metabolic characteristics and is increasingly used for tumor diagnosis, staging, and prognostic analysis.
Although PET-CT is not a mandatory examination item for ICC in some guidelines, more and more research results confirm its important clinical value in diagnosing ICC, as it is simple and clear, allowing even non-radiology medical staff to identify lesions effectively.
PET-CT is mainly based on the principle of increased uptake of 18F-FDG by tumor cells, primarily using standardized uptake value (SUV) for semi-quantitative analysis of attenuation-corrected images. Sabaté-Llobera et al. found a certain correlation between SUV values and CA19-9, carcinoembryonic antigen (CEA), which can assist in clarifying the diagnosis of ICC. Yoh et al. indicated that the SUVmax of ICC tumors is significantly correlated with tumor size and number, but not with the T and N staging of the American Joint Committee on Cancer (AJCC). Multivariable COX regression analysis shows that a high SUVmax predicts poor prognosis after ICC surgery.
Compared to traditional imaging examinations CT and MRI, PET-CT does not have advantages in diagnosing tumor size, subfoci, vascular cancer thrombosis, and bile duct invasion, but it has unique advantages in diagnosing lymph node and distant metastasis.
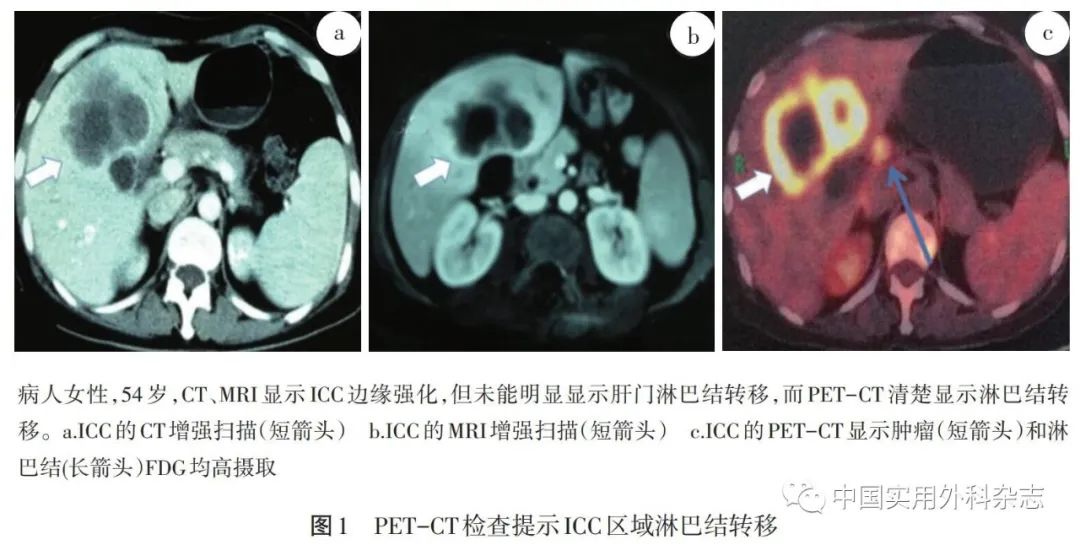
Traditional imaging techniques CT and MRI typically diagnose lymph node metastasis when the shortest diameter of the lymph node is >1 cm. The author conducted a retrospective analysis of 90 ICC surgical patients regarding the relationship between lymph node size and metastasis, finding that the proportion of large lymph nodes with metastasis significantly increased, yet some were still negative for metastasis. For lymph nodes with a shortest diameter <1 cm, nearly 10% still had metastasis. Therefore, lymph node size alone is insufficient for diagnosing metastasis. In PET-CT examinations, when the lymph node SUVmax ≥ 2.5, it is defined as positive, indicating lymph node metastasis. In this study, the accuracy of PET-CT in diagnosing ICC lymph node metastasis (86.7%) was higher than that of CT (62.2%) and MRI (68.9%). The reason is that the FDG uptake value is not affected by lymph node size, allowing for clearer imaging under high SUV conditions.
PET-CT has significant advantages over CT and MRI in diagnosing distant metastasis of ICC, as it can comprehensively display the systemic metastasis of lesions. The author analyzed the distant metastasis of 100 non-surgical ICC patients, finding that PET-CT indicated 92 cases with local lymph node metastasis. There were 23 cases with single-site distant metastasis and 77 cases with metastasis at more than two sites. Among the 100 patients, the most common distant metastasis sites were: supraclavicular lymph nodes, bone metastasis, mediastinal lymph nodes, hilar lymph nodes, and the lungs. The accuracy of PET-CT in displaying distant metastasis (98.4%) was much higher than that of CT and MRI (61.6% and 65.3%), due to: (1) PET-CT itself is a systemic examination, while CT and MRI are often limited to one area. (2) The imaging characteristics of PET-CT make it easier to indicate metastasis in lymph nodes and bones. Thus, PET-CT examination aids in the accurate clinical staging of ICC, allowing patients to receive treatment strategies different from the original plan, significantly reducing the occurrence of ineffective surgeries.
In recent years, PET-MR has also gradually been used in the clinical diagnosis and staging of tumors, but reports on its application in ICC are limited.
4 Combined Diagnosis with Multiple Imaging Techniques
Ultrasound is the first-line examination method for screening ICC. MRI has good soft tissue resolution and multi-directional imaging advantages, and its diagnostic accuracy for ICC is generally higher than that of CT; however, CT is more intuitive in displaying ICC related to intrahepatic bile duct stones. PET-CT combined with CT and MRI can improve the diagnostic accuracy of ICC and compensate for the shortcomings of CT and MRI in diagnosing regional lymph node metastases and distant metastases.
The combined diagnosis with multiple imaging techniques helps further improve the diagnostic accuracy of ICC. Among them, PET-CT should be regarded as a routine and necessary imaging examination for diagnosing ICC and should also be a standard detection method for preoperative staging of ICC.
References
(Swipe your finger in the box to view)
[1] Lee AJ, Chun YS. Intrahepatic cholangiocarcinoma: The AJCC/UICC 8th edition updates [J]. Chin Clin Oncol, 2018, 7(5): 52.
[2] Pan Qi, Wang Lu. Surgical Scope and Challenges of Intrahepatic Cholangiocarcinoma [J]. Chinese Journal of Practical Surgery, 2016, 36(6): 706-708.
[3] Vijgen S, Terris B, Rubbia-Brandt L. Pathology of intrahepatic cholangiocarcinoma [J]. Hepatobiliary Surg Nutr, 2017, 6(1): 22-34.
[4] Oliveira IS, Kilcoyne A, Everett JM, et al. Cholangiocarcinoma: classification, diagnosis, staging, imaging features, and management [J]. Abdom Radiol (NY), 2017, 42(6): 1637-1649.
[5] Chen T, Chang X, Lv K, et al. Contrast-enhanced ultrasound features of intrahepatic cholangiocarcinoma: a new perspective [J]. Sci Rep, 2019, 9(1): 19363.
[6] Lo EC, NRucker A, Federle MP, et al. Hepatocellular carcinoma and intrahepatic cholangiocarcinoma: imaging for diagnosis, tumor response to treatment and liver response to radiation [J]. Semin Radiat Oncol, 2018, 28(4): 267-276.
[7] Min JH, Kim YK, Choi SY, et al. Intrahepatic mass-forming cholangiocarcinoma: Arterial enhancement patterns at MRI and prognosis [J]. Radiology, 2019, 290(3): 691-699.
[8] Kim SA, Lee JM, Lee KB, et al. Intrahepatic mass-forming cholangiocarcinomas: enhancement patterns at multiphasic CT, with special emphasis on arterial enhancement pattern–correlation with clinicopathologic findings [J]. Radiology, 2011, 260(1): 148-157.
[9] Joo I, Lee JM, Yoon JH, et al. Imaging diagnosis of intrahepatic and perihilar cholangiocarcinoma: Recent advances and challenges [J]. Radiology, 2018, 288(1): 7-13.
[10] Kim HJ, Lee SS, Byun JH, et al. Incremental value of liver MR imaging in patients with potentially curable colorectal hepatic metastasis detected at CT: a prospective comparison of diffusion-weighted imaging, gadoxetic acid-enhanced MR imaging, and a combination of both MR techniques [J]. Radiology, 2015, 274(3): 712-722.
[11] Kim R, Lee JM, Shin CI, et al. Differentiation of intrahepatic mass-forming cholangiocarcinoma from hepatocellular carcinoma on gadoxetic acid-enhanced liver MR imaging [J]. Eur Radiol, 2016, 26(6): 1808-1817.
[12] Anupindi SA, Victoria T. Magnetic resonance cholangiopancreatography: techniques and applications [J]. Magn Reson Imaging Clin N Am, 2008, 16(3): 453-466.
[13] Yoh T, Seo S, Morino K, et al. Reappraisal of prognostic impact of tumor SUVmax by (18)F-FDG-PET/CT in intrahepatic cholangiocarcinoma [J]. World J Surg, 2019, 43(5): 1323-1331.
[14] Unterrainer M, Eze C, Ilhan H, et al. Recent advances of PET imaging in clinical radiation oncology [J]. Radiat Oncol, 2020, 15(1): 88.
[15] Bridgewater J, Galle PR, Khan SA, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma [J]. J Hepatol, 2014, 60(6): 1268ss-1289.
[16] Lee Y, Yoo IR, Boo SH, et al. The Role of F-18FDG PET/CT in Intrahepatic Cholangiocarcinoma [J]. Nucl Med Mol Imaging, 2017, 51(1): 69-78.
[17] Sabaté-Llobera A, Gràcia-Sánchez L, Reynés-Llompart G, et al. Differences on metabolic behavior between intra and extrahepatic cholangiocarcinomas at (18)F-FDG-PET/CT: prognostic implication of metabolic parameters and tumor markers [J]. Clin Transl Oncol, 2019, 21(3): 324-333.
[18] Gu Fangming, Wang Zhengguang, Yang Yuan, et al. Clinical value of (18)F-FDG-PET/CT examination in staging intrahepatic cholangiocarcinoma [J]. Chinese Journal of Digestive Surgery, 2019, 18(5): 499-505.
[19] Park TG, Yu YD, Park BJ, et al. Implication of lymph node metastasis detected on 18F-FDG PET/CT for surgical planning in patients with peripheral intrahepatic cholangiocarcinoma [J]. Clin Nucl Med, 2014, 39(1): 1-7.
[20] Lee DH, Lee JM. Whole-body PET/MRI for colorectal cancer staging: Is it the way forward? [J]. J Magn Reson Imaging, 2017, 45(1): 21-35.
[21] Jiang L, Tan H, Panje CM, et al. Role of 18F-FDG PET/CT Imaging in Intrahepatic Cholangiocarcinoma [J]. Clin Nucl Med, 2016, 41(1): 1-7.
(Received on 2020-05-04)
Copyright Statement
This article is an original piece from the “Chinese Journal of Practical Surgery”. For other media, websites, public accounts, etc., if you need to reprint this article, please contact the editorial office of this journal for authorization and clearly indicate in a prominent position under the title that “The original text was published in the ‘Chinese Journal of Practical Surgery’, Volume (Issue): page range.” Thank you for your cooperation!

Click to read the original text and experience the Chinese Journal of Practical Surgery APP.