Chronic inflammatory diseases of the upper and lower airways refer to chronic conditions involving inflammation of the upper and/or lower airways, including: (1) diseases primarily affecting the upper airways: such as allergic rhinitis (AR), non-allergic rhinitis (NAR), chronic rhinosinusitis (CRS), upper airway cough syndrome (UACS), nasal polyps, and adenoid hypertrophy; (2) diseases primarily affecting the lower airways: such as bronchial asthma (commonly referred to as asthma), bronchiectasis, chronic obstructive pulmonary disease (COPD), chronic cough, and diffuse panbronchiolitis (DPB); (3) diseases with coexisting inflammation of the upper and lower airways: such as aspirin-exacerbated respiratory disease (AERD), primary ciliary dyskinesia, sinus bronchial syndrome (SBS), allergic bronchopulmonary aspergillosis (ABPA), cystic fibrosis, necrotizing granulomatous vasculitis, eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome, CSS), and relapsing polychondritis. Coexisting diseases of upper and lower airway inflammation are often related to genetic factors. In China, the incidence is not as high as in Europeans or Caucasians, but it is not rare.
The aforementioned diseases are interrelated to varying degrees in genetics, immunology, anatomy, epidemiology, pathophysiology, clinical presentation, and treatment strategies. However, due to the division of disciplines, these diseases are clinically categorized under respiratory medicine, pediatrics, otorhinolaryngology, allergy, dermatology, and gastroenterology. Specialists often focus more on the manifestations and diagnoses of diseases in their respective fields, frequently overlooking the manifestations and management of these diseases in other areas, significantly affecting the comprehensive understanding and systematic management of these diseases by physicians from various specialties. Therefore, the Asthma Group of the Respiratory Branch of the Chinese Medical Association convened experts from related fields such as respiratory medicine, otorhinolaryngology, pediatrics, and allergy, combining the latest evidence-based medical literature from both domestic and international sources to formulate this consensus, aiming to assist primary care physicians in making correct diagnoses and reasonable management of chronic inflammatory diseases of the upper and lower airways, thereby improving efficacy, avoiding duplicate medication, reducing adverse drug reactions, and alleviating the economic burden on patients (for various detection and evaluation methods mentioned in this consensus, please refer to “Part Four: Practical Detection and Evaluation Methods for Upper and Lower Airway Inflammation”).
Note
This consensus consists of four parts, and this article is the first part.
Part One: Chronic Inflammatory Diseases Primarily Affecting the Upper Airways
1. Overview of AR
Allergic rhinitis (AR) is an IgE-mediated inflammation of the nasal mucosa characterized primarily by eosinophils (EOS) after contact with inhaled allergens. It is a type I hypersensitivity reaction. The prevalence of AR in Asia can be as high as 38%. Typical clinical symptoms include nasal congestion, clear rhinorrhea, paroxysmal sneezing, and nasal itching, which may be accompanied by ocular symptoms such as itchy and watery eyes. Key physical findings include pale, swollen nasal mucosa, turbinate edema, and watery nasal secretions. Some patients with AR may have concomitant asthma, chronic cough, and other lower airway diseases.
2. Diagnosis
The diagnosis is based on typical symptoms, physical signs, and positive allergen test results. Classification is based on the duration of symptoms, categorized as intermittent or persistent. However, the revised practice guidelines for the diagnosis and treatment of rhinitis published by the American Academy of Allergy, Asthma & Immunology still advocate for categorizing based on the timing of allergen exposure, maintaining the terms seasonal, perennial, and transient. Based on the severity of symptoms, such as whether sleep abnormalities occur, and whether daytime activities, leisure, and exercise, learning, and work are limited, as well as the prominence of nasal symptoms, AR is classified into mild and moderate-to-severe. Common auxiliary examination methods include allergen testing (skin prick tests, serum-specific IgE tests), nasal smear or lavage cytology, nasal provocation tests, nasal resistance measurements, exhaled nitric oxide (FeNO) testing, visual analog scale (VAS), and quality of life scoring (AQIQ). These examinations are primarily used to confirm the diagnosis of AR, identify allergens, and assess disease severity and treatment efficacy.
3. Treatment
The treatment goal is to achieve overall control of clinical symptoms and signs, and to reduce the risk of comorbidities and complications.
1. Patient Education:
As an important component of treatment, patient education is key to improving adherence and efficacy. Physicians should pay close attention to patients’ understanding of the disease and treatment. Educational content should include: possible causes and influencing factors of the disease, methods to reduce allergen exposure, medical knowledge related to AR and asthma, treatment goals and methods, the purpose and significance of combination therapy, the necessity and importance of long-term adherence to treatment, medication precautions, and potential adverse drug reactions.
2. Pharmacotherapy:
(1) Intranasal corticosteroids (INCS): These are the first-line medications for AR, such as budesonide (64 μg/spray), fluticasone propionate (50 μg/spray), and mometasone furoate nasal spray (50 μg/spray). Mechanism: They reduce the number of inflammatory cells and the release of inflammatory mediators, thereby decreasing the level of inflammation and alleviating clinical symptoms. However, they do not have a direct effect on allergens and sensitization processes. Due to the difficulty in avoiding allergen exposure, control of inflammation by medication gradually weakens or disappears after discontinuation, thus requiring a certain duration of continuous treatment with INCS. The 2010 AIAR guidelines indicated that reasonable use of INCS does not affect children’s growth and does not lead to adverse reactions such as cataracts in the elderly or avascular necrosis of the femoral head. Administration: Depending on the medication, nasal spray 1-2 times/day for 2-4 weeks or longer, then gradually adjust to the lowest maintenance dose based on whether symptoms are fully controlled; (2) Antihistamines (H1 receptor antagonists): Second-generation antihistamines can reduce CNS excitability and adverse reactions such as drowsiness, fatigue, dizziness, and dry mouth caused by first-generation antihistamines, effectively controlling symptoms like nasal and eye itching and sneezing, and are recommended as first-line medications by multiple guidelines. Commonly used are loratadine, levocetirizine, and cetirizine. The 2015 American guidelines for AR treatment (AGAR2015) state that these medications are contraindicated in children under 5 years of age. Administration: The dosage varies by medication. For example, loratadine 10 mg, taken once daily at bedtime; (3) Nasal decongestants: Can be used for severe nasal congestion for <3-7 days; children should use them diluted; (4) Leukotriene receptor antagonists (LTRAs) can partially alleviate symptoms such as nasal congestion and rhinorrhea caused by increased leukotrienes during the inflammatory process. For example, montelukast sodium, which has good overall safety and tolerability. Administration: Adults 10 mg, children 4 or 5 mg, taken once daily for at least 2-4 weeks, and extended as appropriate if lower airway inflammation is present. However, using LTRA alone is not as effective as using INCS alone.
3. Physiological saline nasal irrigation:
This treatment method can clear allergens and inflammatory factors from the nasal cavity, reduce mucosal edema, promote ciliary movement, and reduce the need for local medication. Studies have shown that using physiological saline nasal irrigation alone for 3 months has a short-term efficacy comparable to that of saline irrigation combined with intranasal corticosteroids. Administration: 75 ml per side per session, 1-2 times/day. Physiological saline close to body temperature can reduce cold stimulation and is more acceptable to children. Patients should be instructed on the correct irrigation method to avoid excessive force pushing water into the middle ear.
4. Specific immunotherapy (SIT):
Currently, SIT in China involves subcutaneous immunotherapy and sublingual immunotherapy primarily using dust mites. Through prolonged repeated exposure to allergen extracts, the immune system gradually reduces sensitivity to allergens and develops tolerance, achieving symptom control or relief. SIT may be a method to modify the natural course of allergic diseases. (1) Treatment method: The World Health Organization’s global guidelines for the treatment of allergic diseases emphasize that subcutaneous or sublingual immunotherapy should be continued for at least 3 years. (2) Indications: ① Patients are allergic primarily to mites; ② Conventional drug treatment cannot effectively control symptoms or has not achieved sustained relief; ③ Drug treatment causes significant adverse reactions; ④ Patients are unwilling to undergo long-term drug treatment; ⑤ Fear of hormone treatment. SIT can be started early in high-risk groups for asthma (e.g., children with AR over 5 years old). During the initial phase of SIT, symptoms may worsen due to increased allergen exposure, so local medications should continue. (3) Contraindications: If SIT triggers or worsens asthma symptoms, it is not recommended: ① Patients with severe asthma not controlled by large or combined drug use; ② Patients currently receiving treatment with β-blockers or angiotensin-converting enzyme inhibitors (increased adverse reactions, affecting the effectiveness of epinephrine in emergencies); ③ Patients with severe cardiovascular diseases; ④ Patients with immunodeficiency diseases; ⑤ Pregnant women, especially in early pregnancy; if pregnancy occurs during SIT treatment, SIT can be continued; ⑥ Patients with malignant tumors; ⑦ Patients with psychological disorders or those who cannot fully understand the risks and limitations of SIT treatment. (4) Types and severity of adverse reactions: The main adverse reactions of subcutaneous immunotherapy include wheal, itching, redness, swelling, and even necrosis at the injection site. For severe local adverse reactions, the next injection dose should be halved. The main adverse reactions of sublingual immunotherapy include sublingual itching and swelling, and gastrointestinal reactions such as abdominal pain and diarrhea may occur due to swallowing. For severe reactions, the last tolerated dose should be repeated, and after achieving tolerance, the dose can be gradually increased. Systemic adverse reactions to allergen immunotherapy can generally be categorized as mild, moderate, severe (non-fatal), and anaphylactic shock based on the timing of occurrence, airway obstruction, and cardiovascular reaction severity.
5. Surgical treatment:
The ARIA2010 guidelines and AGAR2015 guidelines both state that “AR is an allergic disease, and surgical treatment is meaningless.” For severe nasal congestion, the cause should be identified. If it is due to severe nasal septum deviation, turbinate hypertrophy (primarily bony), adenoid hypertrophy in children, or nasal cavity stenosis, and there is no improvement in nasal congestion after medical control of nasal inflammation, surgery may be considered after careful evaluation. The surgical goal is to improve nasal ventilation function, with the principle of preserving the nasal mucosa in managing the turbinates.
The treatment plan for AR should reflect individualization: (1) In children with AR accompanying adenoid hypertrophy and tonsillar hypertrophy: while treating the nasal condition, LTRA should be added, and nasal ventilation function should be evaluated after continuous use for 3 months. If mouth-breathing assistance is no longer needed, and snoring significantly reduces or disappears, surgery can be deferred. If there is no improvement in nasal ventilation function, otitis media with effusion, or nasal-sinusitis after standardized medication treatment, surgical removal of the adenoids is reasonable. For tonsils with degree III hypertrophy, simultaneous bilateral tonsillectomy is recommended during adenoid surgery. For those with otitis media with effusion, tympanostomy tubes are recommended simultaneously.
(2) If clinical symptoms are primarily sneezing, nasal itching, and eye itching, the duration of antihistamine use may be appropriately extended. (3) For those with impaired or lost sense of smell, short-term oral corticosteroids may be used.
4. Diagnosis and Management of AR in Children Under 6 Years
The prevalence of AR in children has significantly increased in recent years. According to the latest data, the overall prevalence of AR in children in eight major cities in China is 9.8%, with the prevalence of rhinitis in preschool children ranging from 10.8% to 20.1%. The prevalence of AR in children gradually increases with age, with the lowest prevalence in children under 2 years old and the highest in children aged 6 to 11 years. Among boys in the same age group, the prevalence of AR is significantly higher than that in girls. Epidemiological studies show that about 40% of children with AR also have asthma.
1. Diagnosis:
Diagnosis is based on typical symptoms, physical signs, and positive allergen test results. The symptoms and signs of AR in children are similar to those in adults. A few children may exhibit specific signs, such as: (1) allergic salute: children often rub their noses upward due to nasal itching or congestion; (2) allergic shiner: shadows under the lower eyelids due to poor venous return; (3) allergic crease: horizontal wrinkles on the nasal skin caused by frequent upward rubbing of the nose tip.
In children under 5 years old, skin testing may be influenced by excessive sensitivity to disinfectants and irritants, and serum-specific IgE testing is usually required. Serum total IgE levels are influenced by various factors including parasitic infections, allergens, and racial differences, and should not be used as a basis for diagnosing AR, but can assess the immune system’s sensitivity to allergens. Very high serum total IgE levels may help predict the risk of AR developing into asthma. For objective assessment of efficacy, please refer to Part Four.
2. Treatment:
The principle of treatment should follow the “combined prevention and treatment, four-in-one” approach, which includes environmental control, medication, immunotherapy, and patient education. (1) Environmental control: Avoid contact with allergens and irritants. (2) Pharmacotherapy: The treatment principles and plans for AR in children are the same as those for adults. INCS is the first-line medication for AR in children, with good safety and tolerability and no adverse effects on growth and development.
Inhaled corticosteroids can directly act on the nasal mucosa without requiring the child’s cooperation. It is important to note that nasal nebulization should use a nebulizer with oscillating waves, which can directly generate aerosolized medication with oscillating characteristics, making it easier to penetrate the sinus openings and achieve good deposition in the sinuses (specific methods can refer to the “Expert Consensus on the Application of Nebulization Therapy in Respiratory Diseases”). Use nebulized medications such as budesonide suspension, 0.25-0.5 mg, twice daily. In principle, nasal decongestants are not recommended for children; if necessary, they should be diluted and used for a short period (<5-7 days). For children with AR accompanied by cough, asthma, or other lower airway inflammation, LTRA can be added. An important treatment method for AR in children is warm saline nasal irrigation, recommended 1-2 times/day. Depending on the device used and the child’s age, it is suggested to spray 1-2 sprays per side, or 50 ml per side per day.
(3) Immunotherapy: It can be used for children over 5 years old, with a total treatment course of no less than 3 years. Specific precautions can refer to the adult AR section. (4) Patient education: Treatment of AR in children is implemented by parents, so education for the parents of affected children is crucial. Parents should be made aware of the recurrent and chronic nature of the disease and its impact on the lower airways, thereby increasing treatment adherence.
5. Diagnosis and Management of AR Accompanied by Lower Airway Inflammatory Diseases
AR is often accompanied by asthma, chronic cough, COPD, and other chronic inflammatory diseases of the lower airways. Epidemiological research data show that 40% of AR patients have asthma, and AR is partly responsible for the onset and difficulty in controlling asthma. AR and allergic asthma share common risk factors and triggers, have the same allergens, and similar treatment methods. The inflammatory features of both are characterized by increased EOS, and both may have elevated exhaled nitric oxide (FeNO) and neurogenic inflammatory mediators. Most cases of nasal inflammation in children are related to allergic factors, and a significantly high proportion of children with AR will develop asthma, with the incidence of comorbidities such as sinusitis and adenoid hypertrophy far exceeding that in adults. Numerous studies have proven that effective control of AR can significantly improve lower airway inflammation, benefiting asthma control and markedly reducing the frequency of asthma attacks and emergency visits. Early and proactive control of AR helps reduce the occurrence and progression of lower airway diseases in children. The diagnosis and management process for AR accompanied by lower airway chronic inflammatory diseases is shown in Figure 1.
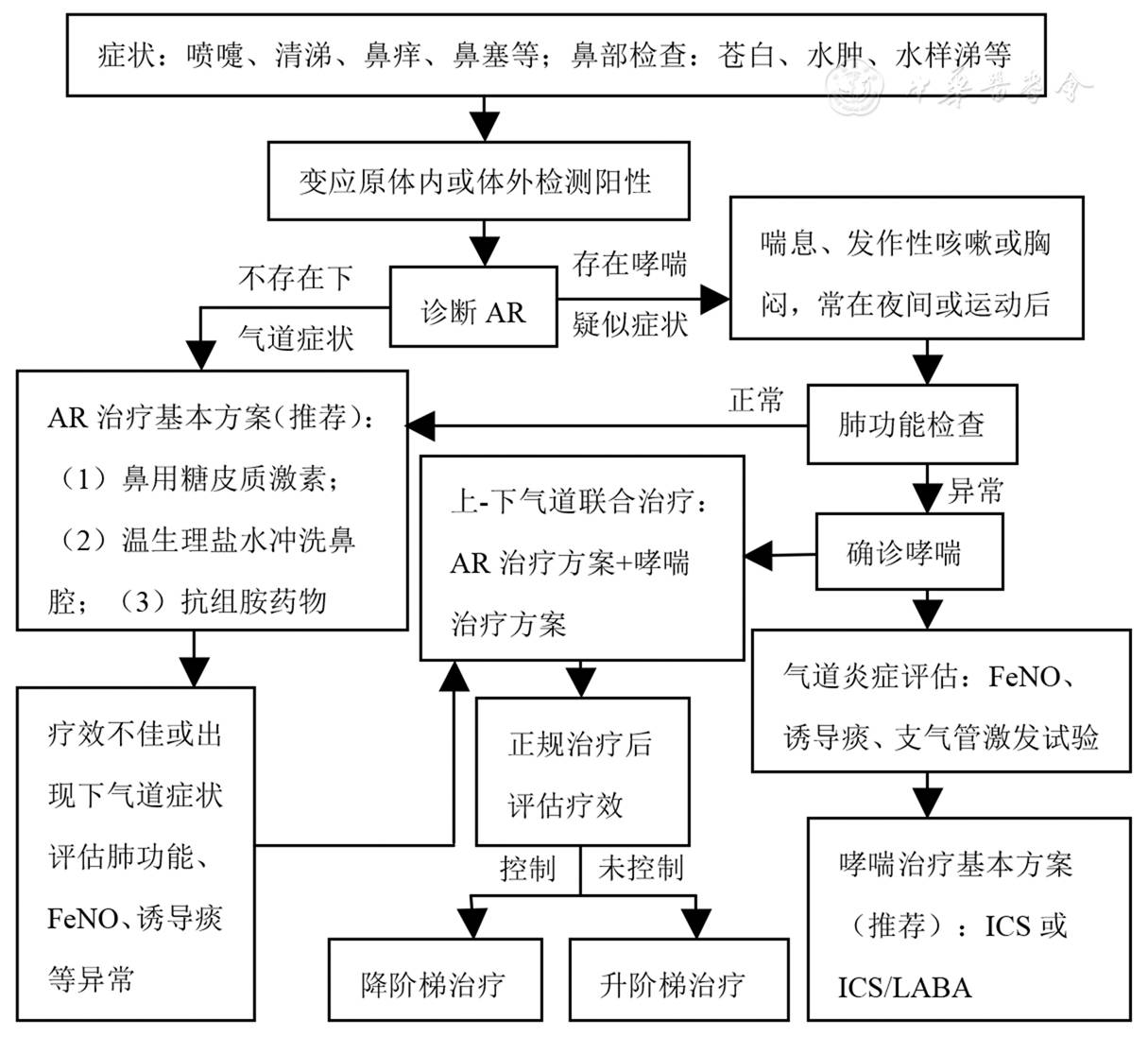
Figure 1: Diagnosis and Management Process for AR Accompanied by Lower Airway Chronic Inflammatory Diseases
A study in Norway involving 1.7 million children found that children born via cesarean section have a 52-fold higher probability of developing asthma compared to those born vaginally. Therefore, strict control of cesarean sections should be implemented, and breastfeeding should be promoted to increase early probiotic intake in infants. The first 1-3 years of life, especially the first year, is a critical period for the gradual establishment of the infant immune system. Efforts should be made to increase exposure to various microorganisms in the natural environment, avoid tobacco smoke exposure, refrain from overusing antibiotics, and promote dietary diversity, which may help reduce the incidence of AR and asthma. For those already affected by AR, allergen exposure should be minimized. The diagnosis of AR-asthma syndrome helps various specialists enhance their understanding of the connections between the upper and lower airways. Based on the clinical symptoms of patients with both AR and asthma, and positive allergen test results, it indicates that both sites are allergic diseases. Studies have shown that among AR patients without lower airway symptoms, 70.8% may exhibit abnormal indicators of lower airway inflammation. Therefore, for patients presenting with “isolated” AR, attention should be paid to inquiring about early clinical manifestations of lower airway diseases and timely testing for lower airway inflammation indicators to avoid missed diagnoses or delayed treatment. The AGAR2015 guidelines first included whether AR patients have accompanying asthma, chronic cough, atopic dermatitis, sleep disturbances, conjunctivitis, CRS, otitis media, and adenoid hypertrophy as observation items to increase vigilance for AR-related diseases and complications.
Treatment for patients with AR accompanied by lower airway chronic inflammatory diseases: (1) Pharmacotherapy: Treatment plans can refer to Figure 1; (2) SIT: Immunotherapy should only be adopted after asthma has achieved complete control. If AR patients exhibit only nasal symptoms without significant lower airway symptoms, but show increased EOS in induced sputum, abnormal FeNO, and positive airway provocation tests, and these abnormal indicators improve following standardized treatment for AR, the addition of lower airway treatment medications can be deferred. Conversely, especially for patients with lower airway symptoms, intervention treatment for lower airway inflammation should be conducted simultaneously, such as inhaled corticosteroids (ICS) or inhaled corticosteroids/long-acting β2 agonists (ICS/LABA).
Assessment of efficacy for AR accompanied by lower airway inflammation: (1) Assess the efficacy of AR/asthma; (2) Assess the control of lower airway inflammation; (3) Assess patient adherence: Patients’ adherence to treatment plans is the most important factor influencing efficacy, which stems from their complete understanding of the disease and treatment.
Management of patients with AR accompanied by airway inflammation: Otorhinolaryngologists should pay attention to lower airway issues in the diagnosis and treatment of AR, emphasizing joint control of lower airway inflammation while treating rhinitis. For patients with significantly abnormal indicators of lower airway inflammation, collaboration with respiratory medicine specialists should be conducted to evaluate and formulate a comprehensive and reasonable treatment plan.
2. NAR
1. Overview
The etiology of non-allergic rhinitis (NAR) is multifactorial, with a wide range of pathophysiological involvement and no clear patterns. The clinical manifestations and signs of NAR often do not differ significantly from those of AR, and negative allergen-specific immunological test results are characteristic of NAR. NAR accounts for 50%-60% of rhinitis cases, but there is no consensus on its classification. Currently, common classifications of NAR include infectious rhinitis (acute and chronic) and other types of NAR. From a clinical perspective, it can be divided into drug-induced rhinitis, gustatory rhinitis, hormone-induced rhinitis, infectious rhinitis, NAR with eosinophilia syndrome, occupational rhinitis, geriatric rhinitis, atrophic rhinitis, and vasomotor rhinitis. Recent studies have found that pharyngeal reflux may be one of the important causes of NAR. None of the aforementioned causes fall under type I hypersensitivity. The impact of NAR on the lower airways is similar to that of AR, but to a lesser extent.
2. Diagnosis
The diagnosis of NAR is based on the patient’s nasal clinical symptoms and signs, along with negative allergen-specific immunological reactions. Diagnosing NAR should aim to investigate the etiology (e.g., structural, drug-related, occupational, etc.). The eosinophilia syndrome is characterized by increased EOS and severe nasal symptoms, which may be more pronounced than AR and often accompanies olfactory disorders and lower airway inflammation. The cause remains unclear and may represent a genetically heterogeneous syndrome or be related to sensitivity to aspirin.
3. Treatment
Due to the multifactorial etiology of NAR, treatment plans should be formulated after efforts to identify the underlying cause, including both anti-inflammatory treatment (similar to AR) and individualized treatment targeting the cause.
1. Anti-inflammatory treatment:
Methods refer to those for AR. For NAR patients where the underlying cause cannot be identified or avoided, prolonged nasal irrigation is recommended.
2. Individualized treatment targeting the cause:
(1) For NAR induced by medications (nasal decongestants): The relevant medication should be discontinued promptly, and short-term oral corticosteroids can be used to alleviate mucosal damage caused by the medication. (2) For eosinophilia syndrome: It often presents with severe nasal inflammation, more frequently accompanied by olfactory disturbances and lower airway inflammation. It responds well to INCS treatment. For persistent or recurrent symptoms, intermittent oral corticosteroids may be used. It is recommended to take prednisone 20-25 mg/day (with caution in cases of gastrointestinal ulcers, hypertension, etc.) once in the morning, for approximately 7 days per course. (3) Occupational: Patients should be advised to avoid the pathogenic environment (e.g., exposure to chemicals, toxins, irritating dust, etc.). (4) Structural: For patients with severe nasal congestion due to poor nasal structure, surgical treatment may be considered after strict assessment of surgical indications and methods. (5) Endocrine-related: Symptoms in patients with endocrine changes (e.g., menstruation, pregnancy, hypothyroidism, acromegaly) may improve with changes or interventions in endocrine status. (6) Geriatric: Clear rhinorrhea (which may appear as dripping during meals) is a common clinical symptom, often related to autonomic dysfunction, with poor response to medication.
4. NAR Accompanied by Lower Airway Chronic Inflammatory Diseases
NAR has a certain relationship with asthma and chronic cough and is also a high-risk factor for asthma onset and a difficult-to-control aspect. The abnormal indicators of lower airway inflammation in NAR patients are similar to those in AR, but to a lesser degree. NAR with eosinophilia syndrome, occupational, environmental, and reflux types can all simultaneously affect the upper and lower airways. Controlling the underlying cause and treating nasal inflammation can significantly improve lower airway inflammation. The positivity rates of lower airway inflammation-related indicators in NAR patients are comparable to those in AR. The diagnosis and treatment process for patients with lower airway inflammatory diseases is similar to that shown in Figure 1.
3. CRS
1. Overview
Chronic rhinosinusitis (CRS) refers to chronic inflammation of the nasal and sinus mucosa lasting more than 12 weeks, with symptoms that may not completely alleviate or may worsen. This condition is a common, frequently occurring, and easily recurrent disease in otorhinolaryngology. The prevalence of CRS ranges from 5% to 15%. A 2015 survey in seven cities in China showed that the prevalence of CRS in adults was 8%, while the diagnosis rate by specialists was only 2%-4%. The causes of CRS remain unclear. The European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2012 indicated that the causes of CRS with and without nasal polyps may be related to gastroesophageal reflux (evidence rating B), while other possible causes include allergies, poor nasal structure, obstructive drainage, odontogenic infections, systemic factors, trauma, and foreign bodies (evidence ratings C, D). The incidence of asthma among CRS patients is 20%, with a high proportion of airway hyperreactivity (27.2%) among CRS patients without a history of asthma. CRS is closely related to delayed-onset asthma, with 20.0% to 31.9% of CRS patients developing asthma.
2. Diagnosis
The main symptoms include nasal congestion and purulent nasal discharge, while secondary symptoms include facial pressure, reduced or lost sense of smell. Key physical signs include purulent discharge from the middle nasal meatus or olfactory cleft, congested and edematous nasal mucosa, or the presence of nasal polyps. CT scans of the sinuses show changes in the ostiomeatal complex or sinus mucosa, with soft tissue density in the nasal cavity and sinuses.
3. Treatment
1. Patient Education:
CRS is a complex and easily recurrent disease, and it is often closely related to lower airway diseases. Patients’ understanding of the disease and treatment is key to improving adherence and reducing recurrence.
2. Pharmacotherapy:
(1) INCS: First-line treatment medication, with significant anti-inflammatory and anti-edema effects, should be administered for at least 3 months, with nasal spray 1-2 times/day. Budesonide suspension nebulization is also an optional treatment; literature reports indicate that 1 mg/2 ml nebulized once or twice daily can effectively improve CRS symptoms. (2) Oral corticosteroids: Can be used preoperatively for 3-5 days to reduce local angiogenesis and vascular permeability, thereby reducing intraoperative bleeding and surgical time. (3) Antibiotics: Recommended only when pathogenic examinations of purulent discharge or secretions in chronic sinusitis patients reveal Staphylococcus aureus, Pseudomonas aeruginosa, or other pathogens (EPOS 2012 recommends amoxicillin-clavulanate orally for no less than 2 weeks). There are differing opinions on the use of macrolide antibiotics. In patients with normal serum IgE levels and low EOS counts, without polyps, who experience recurrence after surgery, or have persistent inflammation, they may be used judiciously, but close attention should be paid to drug resistance and adverse reactions. (4) Leukotriene antagonists: Suitable for CRS patients with concomitant asthma. (5) Nasal irrigation: EPOS lists nasal irrigation as an A-class recommendation for CRS without polyps, as it can clear allergens and secretions from the nasal cavity, improve mucociliary clearance function, and reduce post-nasal drip. Warm saline is recommended. After nasal and sinus surgery, a short-term use of 3% hypertonic saline may alleviate nasal mucosal edema, but its irritation to the nasal mucosa is higher than that of saline, leading to electrolyte imbalances in mucous membranes; therefore, long-term use is not recommended.
3. Surgical treatment:
If symptoms do not improve after 3 months of pharmacotherapy, endoscopic surgery may be performed. The surgical goal is to remove irreversible lesions and restore nasal and sinus ventilation and drainage functions, aiding drug delivery to the sinus cavities to control mucosal inflammation, while preserving nasal and sinus mucosa as much as possible. If the patient has significant structural abnormalities, they should be addressed simultaneously. Patients with difficult-to-treat CRS who have concomitant asthma or aspirin intolerance have a higher recurrence rate postoperatively and require intensified long-term follow-up and management, including enhanced postoperative medication, systemic and local anti-inflammatory treatment to reduce recurrence.
4. Diagnosis and Management of CRS in Children Under 6 Years
CRS is a common disease in childhood, with some studies reporting a prevalence as high as 61.5%. The causes differ from those in adults, with colds being a significant factor. Currently, there are issues in the diagnosis and treatment of pediatric sinusitis, including unclear understanding of the causes, overtreatment, antibiotic misuse, and inappropriate timing and indications for surgery.
1. Diagnosis:
(1) The main symptoms and signs are similar to those in adults, but more frequently include cough, throat clearing, and post-nasal drip, with secondary symptoms such as hearing loss, headache, and lack of concentration. Purulent discharge may be seen in the pharyngeal wall. CT findings are similar to those in adults. Due to the frequent occurrence of colds in children, the sinuses may be simultaneously affected, and CT abnormalities may improve spontaneously following recovery from colds; therefore, the diagnosis of CRS in children should primarily rely on symptoms, and routine nasal sinus CT scans are not recommended. CT may be performed when considering CRS accompanied by adenoid hypertrophy, otitis media with effusion, ineffective medication treatment, or when complications arise to evaluate the need for surgery.
2. Pharmacotherapy:
(1) Antibacterial agents: Pediatric CRS is mostly associated with viral infections, allergies, and inflammatory responses, with bacterial infections being rare; thus, routine use of antibacterial agents is not recommended. If necessary, sensitive antibiotics can be selected based on bacterial culture and sensitivity test reports, or empirically using β-lactamase-resistant antibiotics for no less than 2 weeks. (2) INCS: First-line treatment medication, methods refer to those for adults, with a recommended duration of 3 months. Routine use of systemic steroids is not recommended for children. (3) Nebulized corticosteroids: For CRS accompanied by adenoid hypertrophy and/or otitis media with effusion, nebulized inhalation is recommended. (4) Mucolytic agents: May be used when there is a large amount of purulent discharge, with a treatment duration of no less than 2 weeks. (5) Nasal irrigation: Warm saline irrigation is recommended. (6) Traditional Chinese medicine: Evidence is insufficient and should be used cautiously for adjunctive treatment.
3. Surgical treatment:
Surgery is generally not recommended for children with CRS; however, in cases with adenoid hypertrophy and/or otitis media with effusion, surgical removal of adenoids or tympanostomy may be performed after failure of standardized pharmacotherapy, but strict adherence to indications is necessary.
4. Efficacy assessment:
For children with poor efficacy from CRS pharmacotherapy, attention should be paid to whether adenoid hypertrophy and/or otitis media with effusion are present. In children with severe nasal congestion, mouth breathing, loud snoring, disturbed sleep, and poor hearing, if medication treatment is unsatisfactory, imaging and audiological examinations should be conducted to assess the condition and make timely interventions.
5. Diagnosis and Management Process for CRS Accompanied by Lower Airway Chronic Inflammatory Diseases
1. Diagnosis and Assessment:
CRS is closely related to lower airway chronic inflammatory diseases, such as aspirin intolerance, asthma, bronchiectasis, DPB, and COPD. These patients often exhibit severe CRS symptoms and are prone to recurrence. Therefore, accurately assessing the severity of CRS and whether it coexists with lower airway diseases is crucial for treatment. The diagnosis and management process for CRS accompanied by lower airway chronic inflammatory diseases is shown in Figure 2.
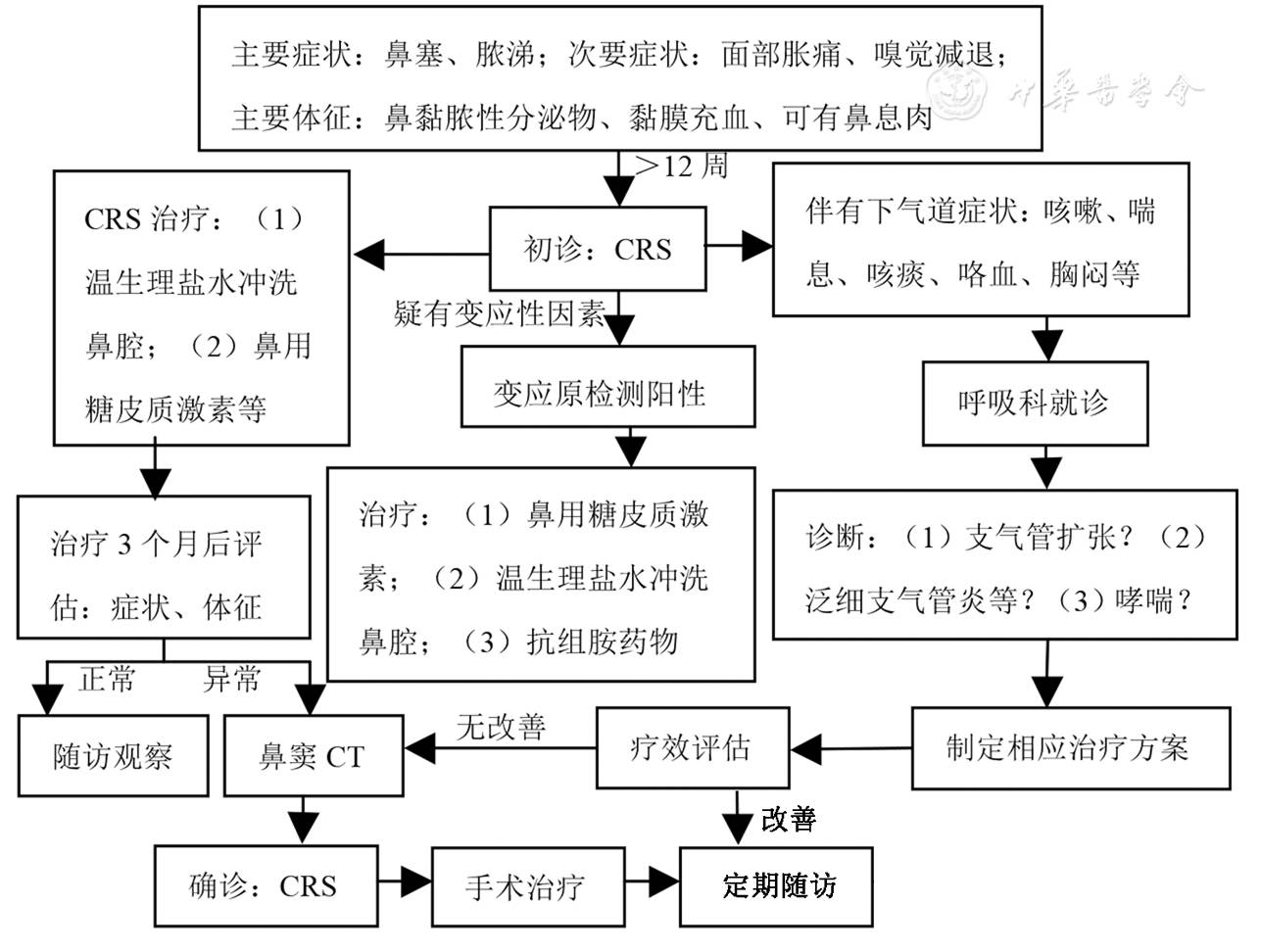
Figure 2: Diagnosis and Management Process for CRS Accompanied by Lower Airway Chronic Inflammatory Diseases
2. Treatment:
(1) For patients with abnormal lower airway inflammation indicators: If ICS treatment is ineffective, montelukast sodium may be added for 3 months, and medication duration should be adjusted based on improvements in lower airway inflammation indicators. (2) For chronic cough: The cause of chronic cough must be clarified; if it is due to UACS, montelukast sodium and cough suppressants may be added, along with nebulized budesonide solution 1-2 mg per dose, 1-2 times/day. If the patient has cough-variant asthma, gastroesophageal reflux, or laryngopharyngeal reflux disease, appropriate treatment plans should be developed. (3) For asthma: The asthma treatment plan should be formulated under the guidance of respiratory medicine specialists.
3. Efficacy assessment:
(1) Clinical symptoms and abnormal examination indicators of the nasal and lower airways should be tracked to assess efficacy. Nasal symptoms are often assessed using VAS scores, while EOS counts in nasal secretions, imaging studies of the sinuses, and nasal endoscopic examinations are routine assessment methods. For lower airway diseases, EOS counts in induced sputum, FeNO, and bronchial provocation tests are standard assessment methods. Specific methods can be found in the assessment section. When CRS is accompanied by lower airway diseases, respiratory specialists should be consulted for treatment recommendations; (2) Postoperative efficacy assessment; (3) Assessment of the efficacy of airway inflammation treatment.
4. Patient Education and Management:
Improve patients’ understanding of CRS, emphasizing its refractory and recurrent nature, making sure they clearly understand the treatment plan, and recommending functional endoscopic nasal surgery when conservative treatment is ineffective, while clearly informing patients of the risks and purposes of surgery, as well as the need for standardized postoperative medication treatment.
6. UACS
1. Overview
Upper airway cough syndrome (UACS) refers to a clinical syndrome characterized primarily by cough, resulting from secretions flowing back from the nasal area to the throat, which directly or indirectly stimulates cough receptors. In 2006, the American guidelines for cough management recommended using UACS instead of post-nasal drip syndrome (PNDS). In China, UACS accounts for approximately 18.6% of chronic cough causes. Strictly speaking, UACS is not an independent disease. Its causes are related to common colds, AR, NAR, CRS, and throat diseases (such as chronic pharyngitis, chronic tonsillitis) as well as pharyngeal reflux. In addition to cough, UACS may also be accompanied by corresponding nasal and throat symptoms and signs. However, isolated throat inflammation-like symptoms do not have diagnostic value for UACS.
2. Clinical Characteristics
1. Symptoms and Signs:
In addition to cough and sputum, symptoms may include nasal congestion, increased nasal secretions, frequent throat clearing, and the sensation of post-nasal drip, with lymphoid follicles visibly proliferating in the posterior pharyngeal wall (cobblestone appearance), and mucus adhering to the posterior pharyngeal wall. For patients with AR, NAR, and CRS, please refer to the corresponding sections for symptoms and signs.
2. Auxiliary Examination:
If CRS is suspected, a CT scan is preferred, and if necessary, nasal endoscopy, allergen immunological tests, etc., may be performed. Seasonal cough suggests an association with pollen allergies, while perennial cough indicates a close relationship with dust mites, fungi, and pet dander; specific allergen testing aids in diagnosis.
3. Diagnosis
Diagnostic criteria: (1) Paroxysmal or persistent cough, primarily during the day and less so at night; (2) Clinical manifestations and history of nasal and/or throat diseases; (3) Auxiliary examinations supporting the diagnosis of nasal and/or throat diseases; (4) Cough relief after treatment targeting the underlying cause.
4. Cough Assessment
It is recommended to conduct a comprehensive assessment of cough using both subjective and objective indicators. Examples include VAS scores, cough symptom scores, cough quality of life assessments (CCIQ, CQLQ, LCQ), cough frequency monitoring, and cough sensitivity testing.
5. Assessing Patient Adherence to Treatment
Due to the difficulty in making a clear diagnosis and insufficient patient understanding of the disease and medication, many UACS patients often undergo various tests repeatedly or use large amounts of antibacterial and cough medications long-term with little effect, severely undermining their confidence in treatment and reducing adherence. Clinicians should strengthen patient education and management to enhance adherence.
6. Treatment
Treatment can be divided into etiological treatment and symptomatic treatment. For common colds, first-generation antihistamines are preferred, as most patients will respond within days to 2 weeks after initial treatment. For causes such as AR, NAR, CRS, etc., treatment methods can refer to the first part of this consensus.
The diagnosis and management process for UACS/PNDS is shown in Figure 3.
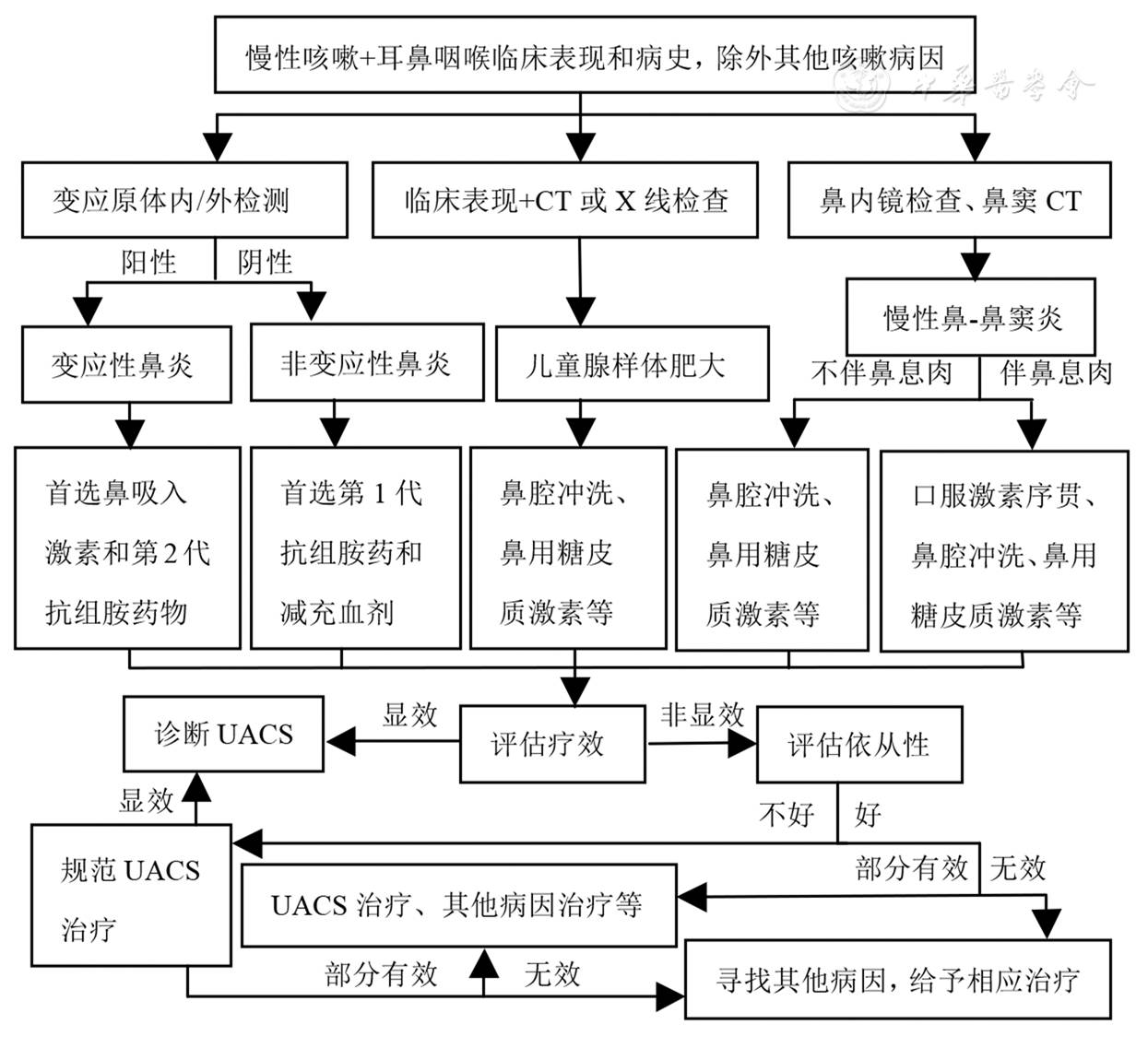
Figure 3: Diagnosis and Management Process for UACS
This article is sourced from the Chinese Medical Journal, 2017, 97(26): 2001-2022.
Click to view recent hot articles
Application of Flow Cytometry in the Diagnosis of Non-Hodgkin Lymphoma: Expert Consensus
Clinical Significance Interpretation of Infection-Related Biomarkers: Expert Consensus
Early Endovascular Intervention Procedures and Guidelines for Acute Ischemic Stroke: Expert Consensus
A Doctor’s Insightful Article on Medical Treatment: Lifelong Benefits
A Dummy Placed in Front of a Baby: Her Actions Shocked the World!