
Secretory otitis media (SOM) refers to the accumulation of fluid in the middle ear without acute inflammatory manifestations, also known as non-suppurative otitis media, exudative otitis media, catarrhal otitis media, serous otitis media, mucous serous otitis media, middle ear effusion, and glue ear. It is more common in winter and spring, and is classified as acute or chronic based on whether the duration exceeds 3 months. If the onset time can be clearly identified, the duration begins from the onset; if the onset time cannot be clearly identified, the duration begins from the date of diagnosis.


The incidence of SOM in children varies across different age groups and regions, with detection rates ranging from 1.16% to 30.7%. It is most prevalent in preschool children, and conditions such as Down syndrome, cleft palate, and autism are high-risk factors for SOM in children.
01Etiology and Pathology
1. Eustachian Tube Dysfunction
(1) Anatomical Factors: The Eustachian tube in children is short, flat, wide, and straight, measuring 15 to 20 mm in length, and matures around the age of 7, with an angle to the horizontal plane of ≤10-20°. Therefore, nasal (pharyngeal) inflammation can easily enter the tympanic cavity through the Eustachian tube, leading to SOM.
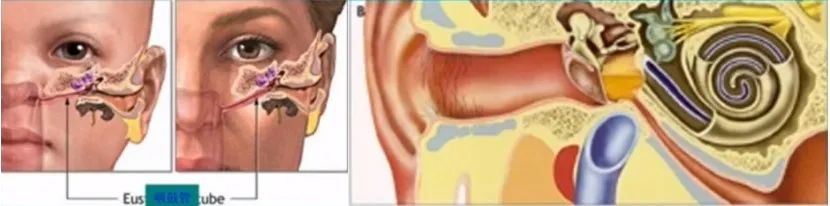
Anatomical diagram of the Eustachian tube
(2) Eustachian Tube Obstruction: Hypertrophy of adenoids or nasal masses can compress the Eustachian tube orifice, affecting middle ear drainage and gas exchange, leading to negative pressure in the tympanic cavity and fluid accumulation.
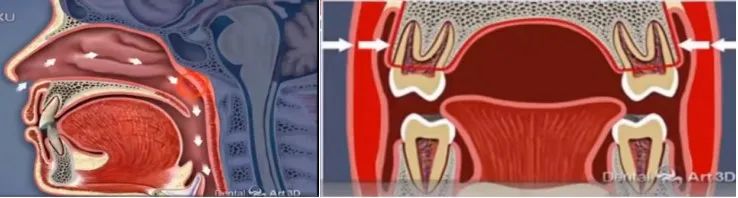
Obstructive diseases such as adenoid hypertrophy lead to mouth breathing
(3) Mucosal Changes in the Eustachian Tube: The “mucociliary transport system” of the Eustachian tube continuously expels pathogens and secretions into the nasopharynx. Congenital ciliary dyskinesia, bacterial exotoxins, inflammatory secretions in the middle ear and Eustachian tube, as well as acute and chronic sinusitis or bronchitis (pneumonia), can cause abnormal mucus secretion and ciliary motility disorders, leading to blockage of the Eustachian tube.
(4) Local Developmental Abnormalities: Children with cleft palates have abnormal development of the levator veli palatini muscle and cannot effectively contract, or the fibers of the tensor veli palatini muscle are underdeveloped, reducing the drainage and pressure-regulating function of the Eustachian tube, resulting in prolonged negative pressure in the middle ear and fluid accumulation.
2. Infectious Factors
SOM was once considered a sterile inflammation of the middle ear, but recent findings have linked SOM to infections, with the most common bacteria being Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis, as well as viruses such as respiratory syncytial virus, adenovirus, rhinovirus, and coronavirus. The presence of varying degrees of bacterial biofilms on the mucosal surfaces of the nasopharynx and middle ear can lead to recurrent SOM and chronic suppurative otitis media.
3. Immune Factors
(1) Allergic Reactions: The proteins and enzymes in the fluid accumulated in the tympanic cavity are secretions rather than exudates and may belong to immune complex (III) diseases; the incidence of SOM is higher in patients with allergic rhinitis, as nasal inflammation can lead to edema of the mucosa at the Eustachian tube orifice, or it may be a rapid allergic (I) reaction or a T-cell mediated delayed allergic (IV) reaction.
(2) Immunoglobulin Deficiency: Secretory antibodies IgA produced by the upper respiratory mucosa can prevent pathogen adhesion and clear resident flora in the nasopharynx. The immature immune system in children and the deficiency of secretory IgA may lead to a higher incidence and recurrence of SOM.
4. Other Factors: Passive smoking, obesity, endocrine diseases, improper breastfeeding positions, excessive use of pacifiers, and gastroesophageal reflux in infants can trigger SOM.
02Clinical Symptoms
1. Hearing Abnormalities:
(1) Some children may complain of hearing loss, most often manifesting asignoring calls, lack of concentration in class which is noticed by parents or teachers; they may also experience abnormal sounds in the ear, enhanced self-hearing, and (or) changes in hearing with body position;
(2) It may also occur that one ear is affected while the other is normal, which maygo unnoticed for a long time and is only discovered during a comprehensive examination by a doctor for nasal issues;
(3) Infants may show delayed responses to speech and environmental sounds,and prolonged hearing loss can lead tospeech development disorders in preschool children.
2. Ear Fullness: Children may feel a sensation of fullness or blockage in the ear, which can be temporarily relieved by repeatedly pressing on the ear.
3. Ear Pain: This is often transient and mild, which adds to the subtlety of SOM.
4. Tinnitus: This is often low-pitched and intermittent, such as “popping” sounds, “buzzing” sounds, and water-like sounds; sounds may occur during head movements or yawning.
5. Dizziness and unsteadiness: A few children may experience vestibular symptoms and balance abnormalities.
03Examinations and Signs1. Otoscopic Examination and Tympanic Membrane Appearance(1) Acute Phase: The tympanic membrane is congested and retracted (the light reflex is dispersed or absent, the handle of the malleus is displaced upward and backward, and the short process of the malleus is bulging), and it may even show retraction pockets in the anterior-superior quadrant or exhibit the contour of the malleus.

Congestion and light reflex changes in the tympanic membrane during the acute phase of SOM
(2) Fluid and Bubble Signs: The tympanic membrane appears dark or amber, with enhanced reflection, and may show air-fluid levels or bubble formation; when there is a significant amount of fluid, the tympanic membrane may bulge.
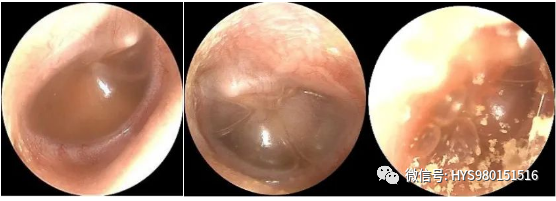
Fluid accumulation and bubble signs in the tympanic membrane
(3) Pneumatic Otoscopy: Dynamic changes in the tympanic membrane can be observed.
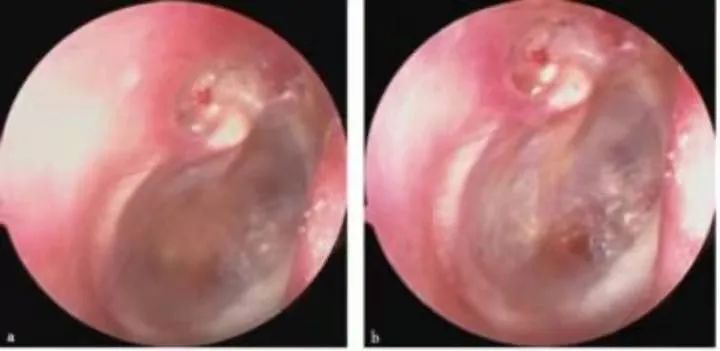
(4) Chronic Phase: The tympanic membrane appears milky white or gray-blue, and when there is prolonged negative pressure in the tympanic cavity or accompanying adhesions, retraction of the tympanic membrane may be observed, even leading to adhesion with the tympanic annulus.
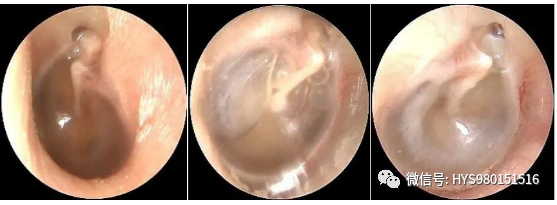
Chronic phase of SOM: amber fluid in the tympanic cavity; retraction of the tympanic membrane, prominence of the short process of the malleus, and formation of retraction pockets in the upper tympanic cavity.2. Behavioral AudiometryChoose based on the child’s age; infants aged 7 months to 2.5 years can use visual reinforcement audiometry, children aged 2.5 to 5 years can use play audiometry, and children over 5 years can undergo pure-tone audiometry, with the average air conduction threshold at frequencies of 500, 1000, 2000, and 4000 Hz used to assess the degree of hearing loss.Hearing loss exceeding 50 dB HL is rarely caused solely by SOM and is usually associated with other middle or inner ear lesions.
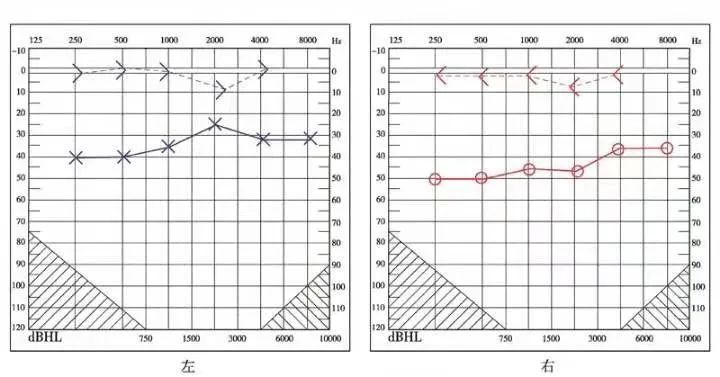
Pure-tone audiometry threshold values for SOM3. Acoustic Impedance Testing: Tympanometry using a 226 Hz probe tone is recommended for children over 6 months of age, primarily classified into types A, B, C, and D. Type B indicates fluid in the tympanic cavity or significant middle ear adhesion, which is a typical manifestation of SOM, with a positive predictive value of 86% to 96%; Type C indicates negative pressure in the middle ear or Eustachian tube dysfunction, which is an excessive type between the normal and fluid-filled ears. Using a 1000 Hz probe tone is more sensitive for detecting SOM in infants under 6 months of age, and tympanograms can be classified as unimodal, bimodal, flat, and uncertain, with unimodal and bimodal types serving as the standard for normal acoustic impedance, while SOM presents as lacking a positive peak.
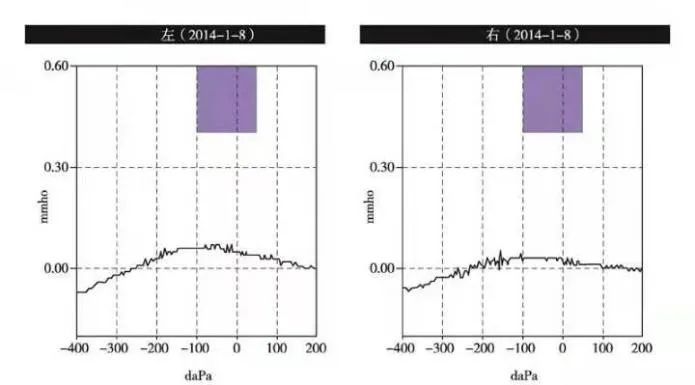
Typical “B” type tympanogram for SOM
Wideband acoustic impedance (WBA) can monitor whether the middle ear fluid is completely removed during tympanostomy, evaluate the efficacy of the procedure, check whether the tube is patent, and whether there is residual fluid in the middle ear.
WBA images indicating middle ear effusion and negative pressure
4. Objective Audiometry
(1) Auditory Brainstem Response (ABR) Testing: For children who cannot cooperate with subjective hearing threshold tests, ABR testing can be performed under sedation, with SOM presenting as elevated ABR thresholds, prolonged I-V wave latencies, and a bone conduction threshold difference of >10 dB.
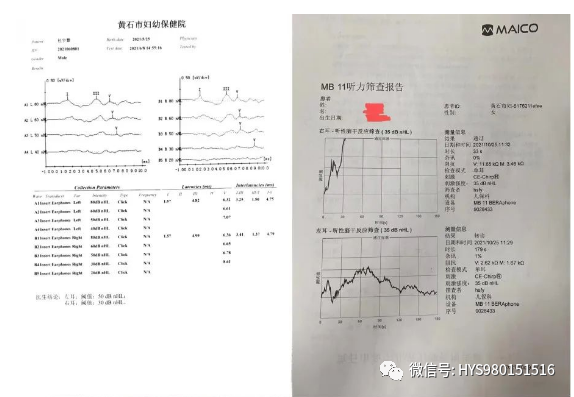
ABR and AABR test result reports
(2) Otoacoustic Emissions (OAE): OAE is not a specific indicator for diagnosing SOM but is directly affected by the functions of the outer and middle ear, thus can assist in diagnosing SOM and assessing its condition and efficacy.
5. Nasopharyngeal Examination: The ear, nose, and throat cavities are interconnected, and inflammation can affect one another. Clinically, it is often necessary to examine the nasal and pharyngeal areas and simultaneously treat related diseases.

SOM associated with adenoid hypertrophy, acute sinusitis, allergic rhinitis, and acute tonsillitis
6. Imaging Examination: Not routinely recommended; CT scans of the temporal bone may be performed if necessary.
04Diagnosis and Differential Diagnosis
Based on the medical history and clinical manifestations, combined with otoscopy and audiometric examinations, diagnosing SOM is not difficult. Clinically, it is often necessary to differentiate it from acute suppurative otitis media, nasopharyngeal masses, cholesterol granulomas, cerebrospinal fluid otorrhea, acute middle ear barotrauma, and jugular bulb tumors.
05Treatment1. Medical Observation
SOM is a self-limiting disease with a high spontaneous resolution rate; children with a history of less than 3 months and no high-risk factors should avoid unnecessary medical interventions and have regular follow-ups.
2. Pharmacological Treatment(1) Corticosteroids: Given the adverse effects of oral steroids, nasal spray formulations are generally recommended.(2) Antibiotics: Antibiotics have adverse effects, resistance, and SOM is self-limiting; their routine use is not recommended in the absence of clear co-infections such as acute sinusitis or upper respiratory infections.(3) Antihistamines: These can inhibit the release of inflammatory mediators, reducing edema and secretion in the tympanic and Eustachian tube mucosa; they are not routinely recommended in the absence of significant allergic conditions such as allergic rhinitis.(4) Mucolytics: These can promote the synthesis and secretion of surfactant-like substances in the Eustachian tube, regulate the ratio of the mucosal surface’s gel and sol layers, and facilitate mucociliary transport and drainage of middle ear fluid.
(5) Decongestants: These can relieve nasal mucosal swelling but have no definitive effect on improving SOM symptoms and may have adverse effects; their use is not recommended.
3. Surgical Treatment(1) Tympanostomy
-
Indications: Unilateral or bilateral SOM lasting more than 3 months, with tympanometric findings showing type B or C, meeting one of the following conditions: ① Hearing loss ≥25 dB HL in the affected ear, with air-bone gap, or affecting speech communication and learning; ② Significant retraction, adhesion, and (or) fluid in the tympanic membrane; ③ Three or more episodes within 6 months, or four or more episodes within a year.
-
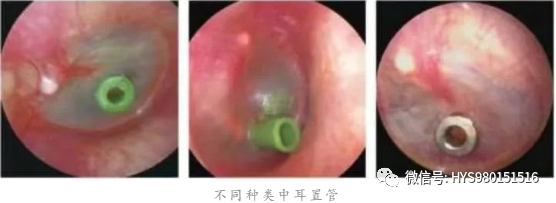
Ventilation tubes: The possibility of SOM recurrence and the patient’s compliance with follow-up must be considered when choosing; they are usually placed in the anterior or posterior inferior quadrant of the tympanic membrane and should not be close to the annulus. Recommendations: ① For children ≤6 years, T-tubes are preferred; for >6 years, button tubes can be selected; ② For those unable to attend follow-ups, button tubes are recommended; ③ In cases of allergic rhinitis, T-tubes may be used during the first placement; ④ Button tubes are preferred for retracted tympanic membranes; ⑤ T-tubes may be selected for completely retracted tympanic membranes and narrow tympanic cavities.
-
Complications includeear discharge, tympanic membrane perforation, retraction, and cholesteatoma formation, and the management principles are: ① Keep the ear canal clean and dry postoperatively; ② For ear discharge, local antibiotic or steroid + antibiotic ear drops are recommended, systemic antibiotics are not routinely recommended, and tube removal is not advised in the presence of ear discharge; ③ Persistent tympanic membrane perforation may require elective tympanoplasty; ④ Retraction pockets and cholesteatoma formation should be addressed electively; ⑤ Tympanosclerosis is generally not treated.
-
Postoperative matters: Follow-up every 3 months after tube placement to check for tube patency, displacement, or dislodgement. The duration of tube placement is typically 12-18 months; for younger children or those with repeated recurrences, the duration should be extended as appropriate; some tubes may naturally fall out, and those that do not need to be removed after the due date. Recurrence of SOM, tube blockage, or early dislodgement with unresolved SOM requires re-tubing.
(2) Adenoidectomy
Indications:
For children ≥4 years who meet one of the following conditions, adenoidectomy is recommended to be performed concurrently with tympanostomy or tube placement:
① Accompanying recurrent sinusitis or nasopharyngitis;
② Recurrent SOM;
③ Repeated tympanostomy;
④ Other indications for adenoidectomy.
For children <4 years, the clinical benefits of adenoidectomy are poor unless there are indications for adenoid surgery (such as adenoid hypertrophy, obstructive sleep apnea, or sinusitis); surgery is generally not recommended.
(3) Tympanic Membrane Puncture and Incision
Tympanic membrane puncture can quickly drain fluid from the tympanic cavity, but it is difficult to perform painlessly, and the puncture site has a short retention time, so it is not recommended. Simple tympanic membrane incision generally heals within 7-10 days and is not routinely recommended for pediatric SOM; laser tympanic membrane perforation can coagulate the edges of the perforation, making it difficult to heal in the short term and may be used selectively.
(4) Eustachian Tube Inflation
Should be avoided in conjunction with acute upper respiratory infections, chronic sinusitis, and acute otitis media. Children over 2 years can be assisted by parents in using a balloon or automatic Eustachian tube inflation device, with follow-up after 2-4 weeks of treatment.
(5) Hearing Aids
For children with other related diseases who cannot improve hearing despite standard treatment and have potential risks affecting speech development, hearing aids may be considered; they are not recommended for children with simple SOM.
4. Follow-Up and Assessment
High-risk children with SOM should be followed up every 1-2 months, while non-high-risk children should be assessed every 3 months.
06Impact and Harm1. MiddleEar Structure and FunctionThe negative pressure and fluid in the tympanic cavity caused by SOM can lead tohearing loss, initially characterized by low-frequency hearing loss due to negative pressure, gradually developing into both low and high-frequency hearing loss due to fluid accumulation. Long-term SOM can lead toadhesive otitis media, persistent negative pressure in the tympanic cavity can formretraction pockets in the tympanic membrane, which may ultimately result incholesteatoma of the middle ear.
SOM with retraction pockets in the upper tympanic cavity
2. Auditory and Speech Development
SOM primarily causes conductive hearing loss, but sensorineural hearing loss may also occur,with an average hearing threshold of about 28 dB HL, leading to children exhibiting unclear speech or age-inappropriate speech errors; good family care can mitigate this impact.
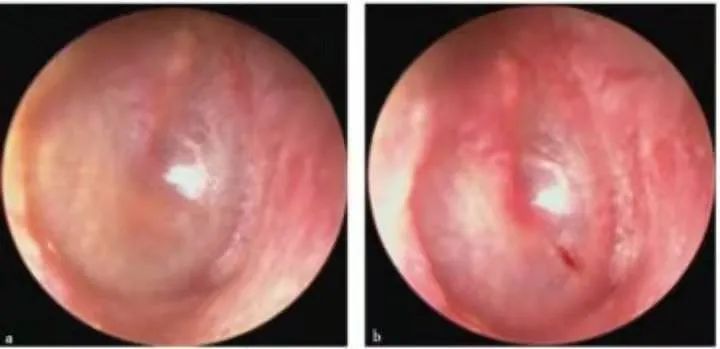
Recurrent SOM after tympanic membrane puncture, with healed puncture sites, and fluid still present in the tympanic cavity; the tympanic membrane is thin, retracted, and shows signs of calcification.
3. Vestibular Function
Long-term SOM may lead to decreased balance abilities in children, but balance and motor skills can generally return to normal after the middle ear fluid resolves.
4. Behavioral and Learning Abilities
Persistent SOM can cause children to be slow to respond, have difficulty concentrating, and experience declines in reading and communication abilities, even being unable to complete tasks and homework independently.
5. Quality of Life
Hearing loss, ear discharge post-tubing, sleep disturbances, behavioral issues, and balance disorders can affect children’s health-related quality of life (HRQL), with the degree of impact related to the severity and frequency of SOM.
07Prevention and Management
The incidence of SOM in children is high, with diverse causes, insidious onset, prolonged course, and significant harm. Active diagnosis and treatment are necessary, as well as knowledge dissemination to ensure early detection, diagnosis, and rehabilitation.
1. Control Causes
Inform parents that the occurrence of SOM is related to various factors including allergic rhinitis, adenoid hypertrophy, upper respiratory infections, air pollution, passive smoking, and pharyngeal reflux, and actively treat primary diseases to reduce recurrence.
2. Cooperate with Follow-Ups
Most children can self-resolve or recover after 3 months of observation, while some require follow-up. Those who have undergone tympanostomy should be informed to avoid water entering the ear and to have regular check-ups.
3. Provide Consultation
Inform parents that children may experience speech development delays, learning and communication difficulties, and behavioral abnormalities due to hearing loss. During follow-ups, inquire about the treatment process and any changes in hearing, speech, and quality of life, and provide appropriate consultations.

“Share if Useful”
Source | Good Doctor [ID: haoyishi520]Copyright belongs to the original author. If there are any violations or infringements, please contact us.
Everyone is watching
Hypotension
Uveitis
Hypomagnesemia
Hypophosphatemia
Fetal cardiac ultrasound
Undifferentiated connective tissue disease
Neuroscience popularization of concussion
Pathological sinus node syndrome
Acute mesenteric vascular embolism
Understand cardiogenic shock in one article
Detailed explanation of Sjögren’s syndrome
China’s 1120 myocardial infarction rescue day
Have you seen Bowen’s?
What are warts? (Common warts)
Discuss Takotsubo syndrome briefly
The past and present of HELLP syndrome
What is POEMS syndrome?
What is Alport syndrome?
I am a nurse, how long will you love me?
Coronary heart disease, this article is enough!
In one minute, learn what cataracts are
COVID-19 prevention and control plan (eighth edition) PPT
Chinese video on simple compression cardiopulmonary resuscitation
Animation and nursing guide on the occurrence and treatment of cerebral aneurysms
Learn this technique, it can save lives at critical moments
5.17 World Hypertension Day | Healthy blood pressure, healthy life
If it weren’t for mammary hyperplasia, maybe we would have…
[420 Gout Day] This article explains gout thoroughly!
What is respiratory syncytial virus? Have you heard of it?
Stop urging nucleic acid reports, this article will make you understand!
What is vocal cord leukoplakia? Which populations are prone to it?
World Prematurity Day: Breastfeeding empowers early babies with love and ability
Valentine’s Day “Death” Guide, cases that make doctors afraid of sex!
World Tuberculosis Day | End tuberculosis epidemic, breathe freely and healthily
What is Asperger’s syndrome?
“World AIDS Day” – “Join hands to prevent and control AIDS, share health responsibility”
My senior son insists on studying medicine, and the doctor father wrote this informed consent overnight
Attention! New anti-corruption regulations: Doctors are not allowed in entertainment venues, and offices are not allowed to have unopened alcohol and tobacco
“Spring has arrived, but I can’t smell the flowers” – Sexual immaturity with anosmia in Kallmann syndrome
After hours of rescue, the life of a 23-year-old young man could not be saved! You must learn some first aid knowledge, it can save lives at critical moments!
★★★★★
Remember to share after reading
