
The 65th Annual Meeting of the American Society of Hematology (ASH) will be held in San Diego, USA, from December 9 to 12, 2023. Professor Jiang Qian’s team summarizes the 2023 ASH Continuing Education on Chronic Myeloid Leukemia (CML) to share with everyone.
Today, we present the article: Accelerated Phase of Chronic Myeloid Leukemia (CML) at Diagnosis and Transformation.
Although most CML patients have shown significant improvement in prognosis after treatment with Tyrosine Kinase Inhibitors (TKI), some patients are still diagnosed with accelerated or blast phase during initial diagnosis or treatment. Exploring the pathogenesis, differentiation, and new treatment strategies for blast phase (CML-BP) is crucial for managing patients in blast phase, precision treatment, and prognosis. This article focuses on the revision of CML staging definitions, CML lymphoid blast phase (CML-LBP) and Ph+ positive acute lymphoblastic leukemia (Ph+ ALL), the impact of next-generation sequencing (NGS) on CML-BP, and new treatment strategies.
1Revision of CML Staging Definitions
1. There are certain differences in the CML staging standards across different guidelines, as shown in Table 1. The latest WHO guidelines in 2022 removed the definition of accelerated phase (AP) and did not include cytogenetic characteristics, a revision that has sparked considerable controversy:
-
Most newly diagnosed AP patients have a fairly good treatment response and outcome compared to chronic phase (CP) patients, and the incidence of progression to AP after TKI treatment has significantly decreased. Based on this, WHO 2022 removed the definition of AP.
-
Although WHO 2022 did not consider cytogenetic characteristics, the presence of Additional Chromosomal Abnormalities (ACAs) has been confirmed to be associated with higher disease progression, shorter progression-free survival (PFS), and shorter overall survival (OS), especially high-risk ACAs.
-
The authors believe it is wiser for WHO to cautiously redefine the diagnostic criteria for AP rather than abolishing it completely. For instance, the simplification of AP definition in the ICC 2022 update only considers three variables: blast cells, basophil count, and ACAs.
-
Regardless of the definition used, close monitoring of AP patients’ responses is essential, as single-agent TKI treatment may not be sufficient for some patients. For example, patients with 3q26.2 rearrangements should consider allogeneic stem cell transplantation or participation in clinical trials targeting EVI1.
2. The definition of BP has also been revised in ICC 2022 and WHO 2022:
-
When there is an increase in peripheral blood/bone marrow blast cells, CML-LBP should be suspected. ICC 2022 sets the threshold for blast cells at >5%. However, the evidence supporting this revision is currently limited.
-
Our recommendation is to perform flow cytometry analysis at diagnosis to ensure the identification of patients with increased blast cells, allowing timely initiation of appropriate treatment.
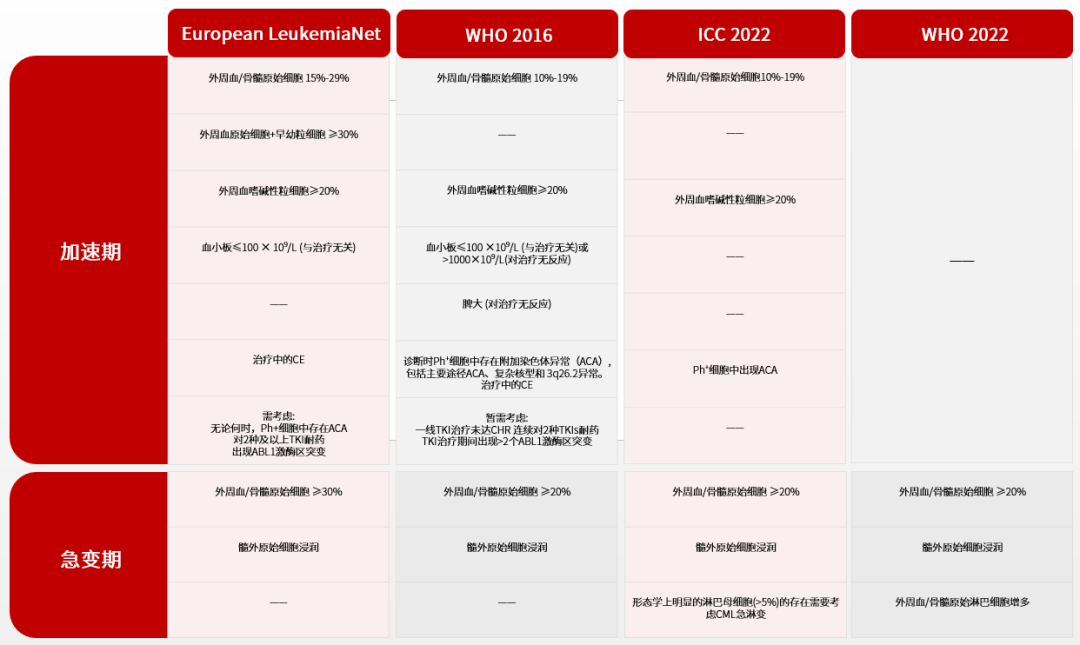
▲ Definitions of CML Accelerated Phase and Blast Phase (Table 1)
2CML-LBP and Ph+ ALL
1. Comprehensive flow cytometry analysis is needed at initial diagnosis
At initial diagnosis of CML, comprehensive flow cytometry testing can accurately count the proportion of blast cells and identify abnormal cell phenotypes. When patients exhibit an abnormal lymphoid phenotype, the risk of progressing to blast phase significantly increases, necessitating more frequent monitoring, including repeated bone marrow biopsies and actively seeking hematopoietic stem cell transplant donors (Table 2). Moreover, when patients continue to exhibit an abnormal lymphoid phenotype, they should be managed according to CML-LBP.
2. When an abnormal lymphoid phenotype appears, prevention of central nervous system leukemia (CNSL) is crucial
When patients exhibit an abnormal lymphoid phenotype, it is essential to emphasize the prevention of CNSL. Chemotherapy regimens should include high-dose cytarabine or methotrexate that can penetrate the blood-brain barrier, and comprehensive cerebrospinal fluid and imaging examinations as well as regular intrathecal chemotherapy should be performed. When CNSL is diagnosed, in addition to intrathecal administration, it is recommended to choose dasatinib or ponatinib, which can penetrate the blood-brain barrier.
3. Should allogeneic hematopoietic stem cell transplantation be preceded by myeloablation or reduced-intensity conditioning for patients in blast phase?
Both myeloablative and reduced-intensity conditioning have their advantages; although both regimens yield comparable overall survival, the latter is associated with a higher relapse rate. Therefore, myeloablative conditioning is recommended. However, in actual clinical practice, due to factors such as age and comorbidities, more patients opt for reduced-intensity conditioning.
4. Differentiating CML-LBP from Ph+ ALL
When immunoglobulin/T-cell receptor (Ig/TCR) gene rearrangements are consistent with BCR::ABL transcript levels, it is more indicative of Ph+ ALL; otherwise, it is CML-LBP.
3The Role of NGS in CML-BP
NGS testing has improved the detection rate of BCR::ABL1 kinase domain mutations from 50% to 80%. The disease progression of CML is closely related to cytogenetic abnormalities, BCR::ABL1 kinase domain mutations, and mutations of other cancer-related genes such as RUNX1, IKZF1, and ASXL1 (Figure 1). Compared to patients who achieve optimal efficacy, most patients progressing during TKI treatment exhibit molecular genetic abnormalities. Therefore, it is recommended that CML patients undergo NGS testing at initial diagnosis to identify high-risk populations.
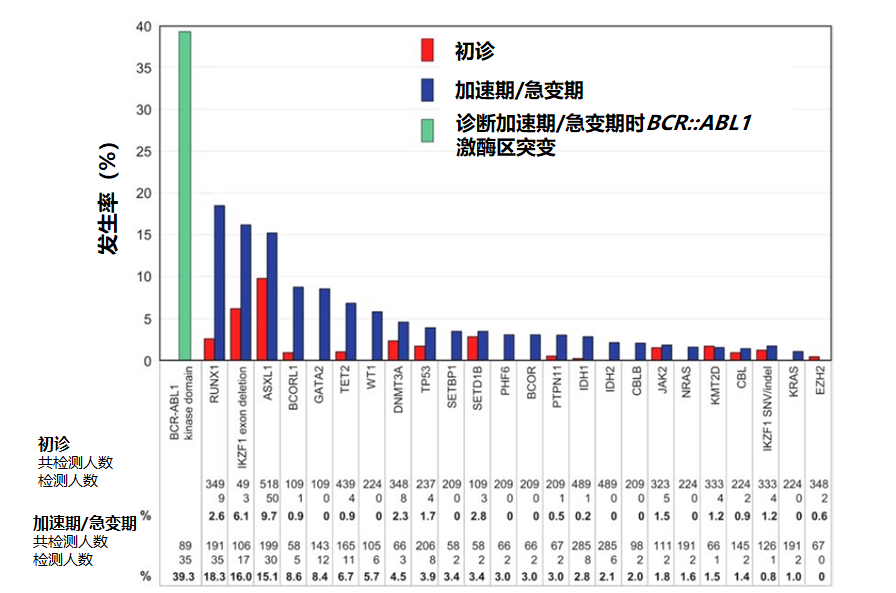
▲ Gene mutation profile at initial diagnosis and during accelerated/blast phase (Figure 1) Source | Accelerated-phase CML: de novo and transformed4New Treatment Strategies
1. The treatment goal for CML-BP is to quickly return to chronic phase for allogeneic hematopoietic stem cell transplantation. Currently, there is no clear consensus on the treatment of CML-BP; a TKI combined with chemotherapy regimen is recommended. The choice of chemotherapy regimen depends on the type of blast phase; acute myeloid transformation requires an acute myeloid leukemia-like chemotherapy regimen, while acute lymphoid transformation requires an acute lymphoblastic leukemia-like chemotherapy regimen. The choice and dosage of TKI are currently unclear, but to achieve better treatment responses and outcomes, it is recommended to select more potent TKIs. The MATCHPOINT study explored ponatinib combined with fludarabine, high-dose cytarabine, granulocyte colony-stimulating factor, and mitoxantrone (FLAG-IDA). Other studies have confirmed that dasatinib combined with decitabine is a safe and effective regimen. Overall, the treatment plan for CML-BP is still in the exploratory stage, requiring more new treatment strategies.
2. Patients with significant pancytopenia should be considered for hematopoietic stem cell transplantation. If transplantation is temporarily not possible, TKI standard doses should be maintained through transfusions and cytokines, and dose reduction or discontinuation is not recommended.
▲ High-risk patients who need to consider finding donors for transplantation (Table 2)END
Compiled by | Bao Mei, Qi Feiyang, Yang Sen
Reviewed by | Jiang Qian
References
Shanmuganathan N, Hughes TP. Accelerated-phase CML: de novo and transformed. Hematology Am Soc Hematol Educ Program. 2023 Dec 8;2023(1):459-468.

Jiang Qian
National Center PI 、Professor
Chief Physician, Doctoral Supervisor
National Clinical Research Center for Hematologic Diseases
Peking University People’s Hospital
Peking University Institute of Hematology

Bao Mei
Advisor: Professor Jiang Qian
National Clinical Research Center for Hematologic Diseases
Peking University People’s Hospital
Peking University Institute of Hematology

Qi Feiyang
Advisor: Professor Jiang Qian
Peking University People’s Hospital
Yang Sen
Advisor: Professor Jiang Qian
National Clinical Research Center for Hematologic Diseases
Peking University People’s Hospital
Peking University Institute of Hematology
The Yimaitong platform is a professional online doctor platform, with the mission of “perceiving the pulse of world medicine and assisting clinical decision-making in China.” The platform offers a series of products including “Clinical Guidelines,” “Medication Reference,” “Medical Literature King,” “Medical Knowledge Source,” “e-Research Pass,” and “e-Pulse Broadcast,” fully meeting the needs of medical practitioners for clinical decision-making, acquiring new knowledge, and enhancing research efficiency.This platform aims to convey more medical information to healthcare professionals. The content published on this platform cannot replace professional medical guidance in any way and should not be considered as medical advice. If such information is used for purposes other than understanding medical information, this platform shall not bear any related responsibilities. The content published by this platform does not represent agreement with its descriptions and viewpoints. If there are copyright issues, please contact us, and we will handle them promptly.