Background
Common treatment methods for hematologic malignancies, immunodeficiencies, hemoglobinopathies, and metabolic disorders include allogeneic hematopoietic stem cell transplantation (allo-HSCT). However, there are many restrictions on the clinical extraction of spinal cord from juvenile donors, leading to suboptimal extraction results. Peripheral blood stem cell collection (PBSC) is a mature technique used to collect progenitor cells, which involves the use of recombinant human granulocyte colony-stimulating factor (rhG-CSF) to enhance the yield of granulocytes collected, mobilizing hematopoietic stem cells (HSC) from the bone marrow into the peripheral blood, and then obtaining HSC through extracorporeal continuous-flow leukopheresis.
1 Study Subjects
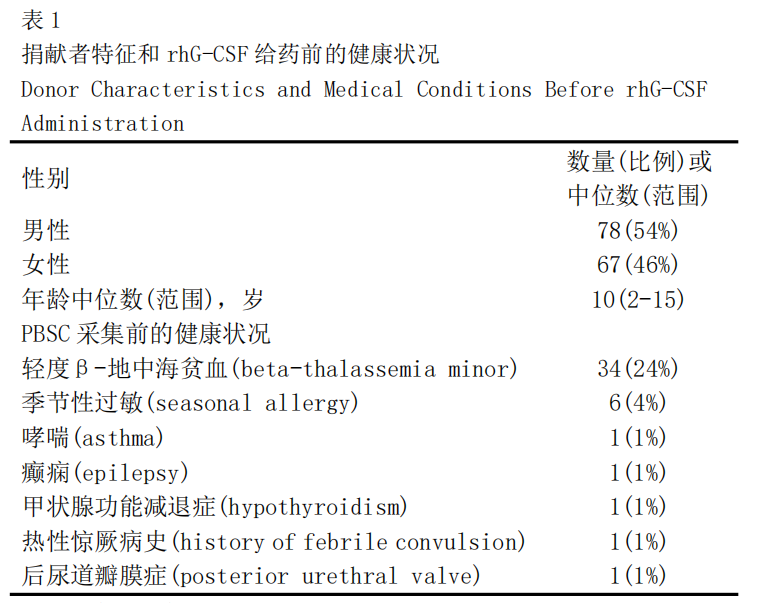
A total of 179 donors who consented to participate in a prospective study from September 1998 to February 2014 were selected (all recipients were relatives, and their parents had undergone PBSC collection). The experimental and transplantation procedures were approved by the Hematology-Oncology Research Center and the Stem Cell Transplantation Ethics Review Board. All donors underwent comprehensive physical and blood examinations prior to donation. Specific results are shown in Table 1.
2 Treatment Process and Results
2.1 Short-Term Side Effects
Fatigue (n=7, 5%) and headache (n=5, 3%) were the most common side effects reported by donors after the administration of rhG-CSF. Other side effects and data are shown in Table 2. All adverse reaction symptoms were mild to moderate and resolved within one week after discontinuation of rhG-CSF, with no donors terminating or reducing the rhG-CSF dosage due to side effects. The incidence of side effects was higher in female donors (22%) compared to male donors (12%), however, this association did not reach significance (P=0.08). The incidence of side effects did not show a significant correlation with donor age (P=0.52).
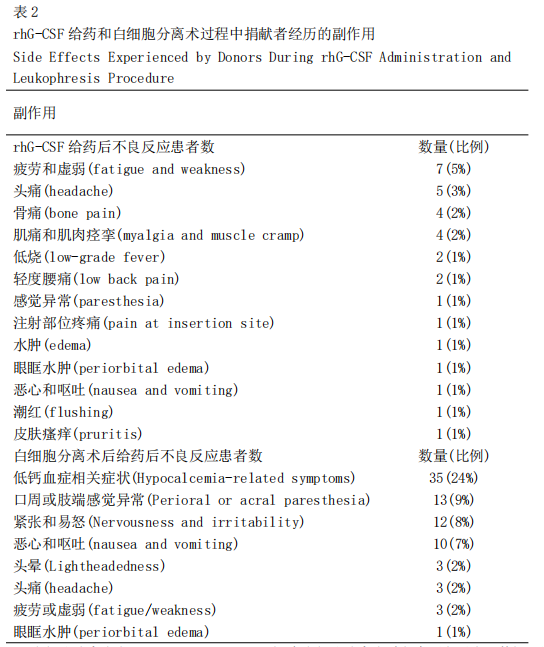
2.2 Leukopheresis Procedure
Adverse reactions and data during the leukopheresis procedure are documented in Table 2. For patients exhibiting symptoms of hypocalcemia (i.e., nausea and vomiting, perioral and peripheral paresthesia, headache, and agitation), intravenous injection of 5-10 mL of 10% calcium gluconate solution (administered over 10-15 minutes, repeated every 4-6 hours based on serum calcium levels and symptoms) was provided. After examination and clearance, eligible donors received subcutaneous injections of rhG-CSF at 5μg/kg for three consecutive days, with two injections on the fourth day. PBSC was collected on the fifth day using standard leukopheresis through a continuous-flow blood cell separator.
2.3 Long-Term Side Effects
All patients in this study survived. Two pregnancies occurred after the administration of rhG-CSF, both resulting in the normal delivery of healthy infants. During a median follow-up time of 4.8 years (1.2-14.2 years), no reports of any tumor-related diseases were made. One 5-year-old donor was found to have dyslexia and received educational therapy and support. A donor with a history of epilepsy remains controlled and has not experienced any seizures since the age of 4 (10 years prior to PBSC collection). One donor was diagnosed with epilepsy three years after PBSC donation and is currently receiving treatment with sodium valproate.
3 Discussion
This retrospective study aimed to assess the short-term and long-term risks associated with the use of rhG-CSF and leukopheresis in healthy pediatric donors. This investigation is one of the largest single-center series examining the long-term effects of PBSC collection in healthy pediatric donors. G-CSF is a cytokine that promotes the proliferation, survival, and differentiation of neutrophil-granulocyte lineage cells and mobilizes bone marrow progenitor cells into peripheral blood. rhG-CSF is used to treat congenital and chemotherapy-related neutropenia, as well as to mobilize circulating HSC in peripheral blood. The use of rhG-CSF for PBSC mobilization and separation is a widely practiced method for HSCT purposes. In 2013, mobilized PBSC accounted for approximately 20% and 85% of the sources of grafts for pediatric and adult HSCT, respectively.
In this study, rhG-CSF was well tolerated with no significant toxicity. During a median follow-up of 3.9 years, no serious adverse reactions attributable to rhG-CSF were observed. The most common short-term clinical symptoms after rhG-CSF were fatigue (5%) and headache (3%), which are significantly lower than the data reported in adult cohorts, where the most common symptoms in adult donors were bone pain. Kawano et al. compared PBSC collection in pediatric and adult donors and reported that younger children (<10 years) did not experience any side effects after rhG-CSF administration. They also noted that older children most commonly experienced headache and fatigue, which is consistent with our findings. They found that G-CSF levels in children were lower than in adult donors and suggested that the lower incidence of rhG-CSF-related symptoms could be partially explained by this finding.
PBSC collection may be beneficial for both HSCT donors and recipients compared to bone marrow collection. Pediatric bone marrow HSCT collection must be performed in an operating room under general anesthesia with sterile techniques, involving repeated large-bore needle insertions into the iliac crest to extract bone marrow. Despite the risks associated with anesthesia (such as cardiac arrest, brain injury, and death), suboptimal cell collection is not unexpected, especially when there is a significant weight difference between the recipient and the related donor. There is evidence that using PBSC as a source of graft can achieve faster neutrophil and platelet engraftment and reach higher numbers of CD34+ cells while avoiding anesthesia, transfusions, and bone marrow collection procedures.
To our knowledge, this study is one of the largest single-center cohort studies with long-term follow-up of normal pediatric donors; however, there are some limitations. Although there were no occurrences of cancer, severe long-term complications, or deaths in our population, the small sample size, loss to follow-up of some donors (18%), and the limited number of children followed for over 10 years restrict our ability to detect rare events (such as malignancies) and determine the long-term risks of PBSC donation in normal children.
Conclusions and Recommendations
In conclusion, our results indicate that short-term exposure to rhG-CSF for PBSC donation is safe and effective for healthy children. We did not encounter any occurrences of adverse hematologic diseases or deaths. Although there were no occurrences of leukemia or severe adverse events in our population, and reports indicate no association between rhG-CSF administration and the occurrence of hematologic diseases, more definitive data from multiple centers with long-term follow-up of pediatric donors are needed to fully assess the impact of short-term exposure to rhG-CSF on the development of acute leukemia in healthy pediatric PBSC donors. In this way, we will be able to determine the optimal lower age limit for unrelated donor stem cell sourcing and the selection of pediatric donors.
References: omitted
Source: Long-Term Safety of Short-Term Administration of Filgrastim (rhG-CSF) and Leukopheresis Procedure in Healthy Children: Application of Peripheral Blood Stem Cell Collection in Pediatric Donors. Biol Blood Marrow Transplant, vol. 24, 2018, pp. 866-870.