The Journal of Neurosurgery was published online on February 4, 2022, by 15 experts from the USA, Turkey, Egypt, Czech Republic, India, Dominican Republic, Canada, and others, including Stylianos Pikis, Georgios Mantziaris, Selcuk Peker, titled “Stereotactic radiosurgery for intracranial chordomas: an international multiinstitutional study” (doi: 10.3171/2021.12.JNS212416).
Objective:
The aim of this study is to evaluate the safety, effectiveness, and long-term outcomes of stereotactic radiosurgery (SRS) for the treatment of intracranial chordomas.
Chordomas are rare bone tumors of the axial skeleton, believed to arise from malignant transformation of residual notochord. They occur at a rate of 1 in 100,000 and account for 5% of all bone cancers. They are located in the skull base, spine, and sacrum with approximately equal frequency. Chordomas most commonly occur in adults around age 50, with less than 5% occurring in children. When they do occur, they show a male predominance. Skull base chordomas affect 1 in 1 million per year, accounting for 0.15% of all intracranial tumors. As locally invasive tumors, they are often located at the clivus. Intracranial chordomas present with visual disturbances, headaches, cranial nerve palsies, and rarely with endocrine disorders. In most patients, the safest initial treatment strategy involves high-dose adjuvant radiation following tumor resection. Currently, for small-volume residual or recurrent chordomas where adjuvant resection is not feasible, SRS is recommended. Despite a multicenter SRS outcome report published by the North American Gamma Knife Consortium (NAGKC) in 2011, further data on the long-term outcomes of SRS for chordomas is still needed. This study serves as an update to the NAGKC study published in 2011, aiming to include more patients with longer follow-up times to evaluate the optimal timing, safety, effectiveness, and long-term patient prognosis of SRS for intracranial chordomas.
Methods:
This retrospective multicenter study involved consecutive patients from 10 participating centers who received single-session SRS treatment for intracranial chordomas.
During treatment, each participating center utilized the Gamma Knife to deliver single-session SRS treatment. After installing the Leksell stereotactic head frame (Elekta Instruments AB), high-resolution thin-slice (1mm) T1 and T2-weighted MRI scans were obtained and used for stereotactic planning. A multidisciplinary treatment team at each participating center developed a dose plan to deliver an effective radiation dose to the target tumor.
SRS treatment outcomes were evaluated through radiological and neurological assessments, and statistical methods were used to evaluate predictive factors.
Results:
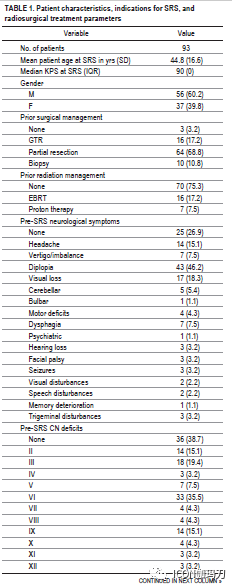
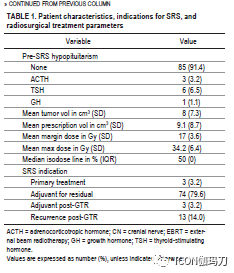
A total of 93 patients (56 male [60.2%], mean age 44.8 years [SD 16.6]) underwent single-session SRS for intracranial chordomas. 77 patients (82.8%) received SRS as adjuvant therapy, 13 patients (14.0%) underwent SRS for recurrent disease, and 3 patients (3.2%) received SRS as initial primary treatment.
The mean tumor volume was 8 cm3 (SD 7.3), and the mean prescribed volume was 9.1 cm3 (SD 8.7). The average marginal and maximal radiation doses delivered were 17 Gy (SD 3.6) and 34.2 Gy (SD 6.4), respectively.
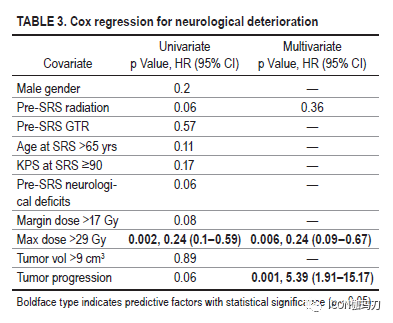
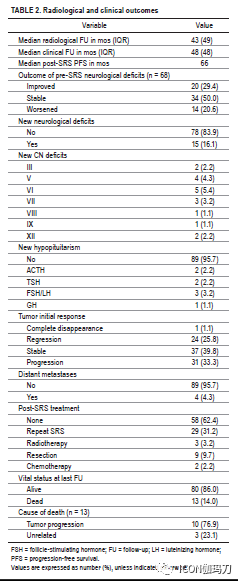
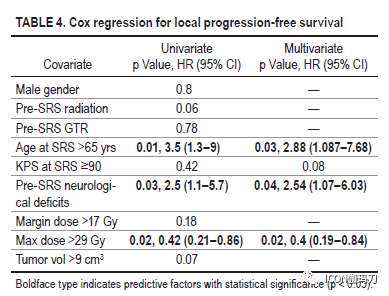
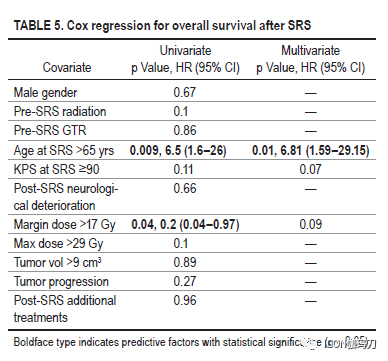
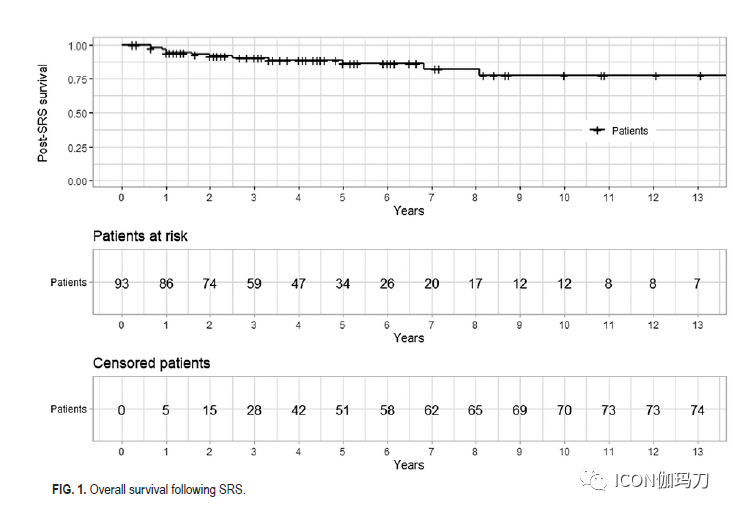
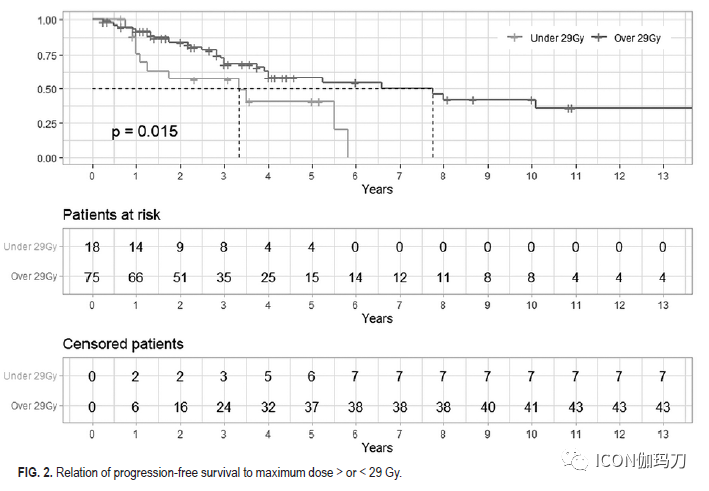
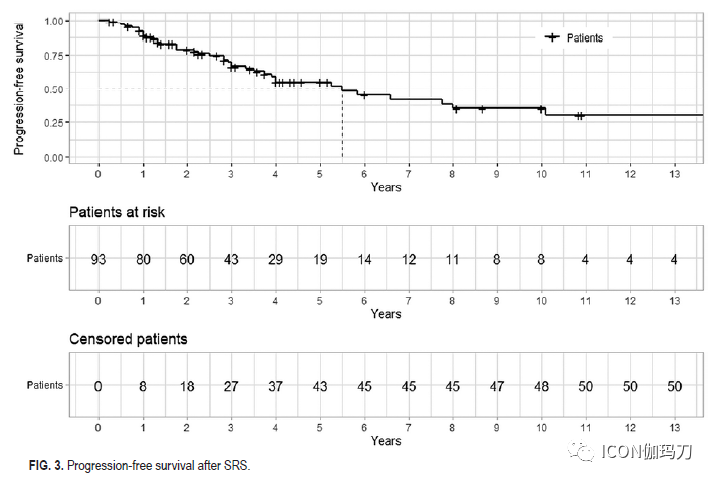
In multivariate analysis, treatment failure due to tumor progression (p = 0.001) was associated with an increased risk of neurological deterioration following SRS treatment, while a maximal dose > 29 Gy (p = 0.006) was associated with a reduced risk. A maximal dose > 29 Gy was also associated with improved local tumor control (p = 0.02), whereas pre-existing neurological deficits (p = 0.04) and age > 65 years in SRS patients (p = 0.03) were associated with poorer local tumor control. The 5-year and 10-year progression-free survival rates were 54.7% and 34.7%, respectively. Patient age > 65 years at SRS treatment (p = 0.01) was associated with decreased overall survival. The 5-year and 10-year overall survival rates were 83% and 70%, respectively.
Discussion:
In this multicenter study, 93 patients underwent SRS treatment across 10 participating centers. We evaluated the safety and efficacy of SRS treatment for skull base chordomas within a multidisciplinary treatment framework. During a median clinical follow-up of 48 months (IQR 48) following SRS, 15 patients (16.1%) experienced new neurological deficits, and 4 patients (4.3%) developed new pituitary axis deficiencies. Tumor progression (p = 0.001) was associated with an increased risk of neurological deterioration following SRS treatment, while a maximal dose > 29 Gy was associated with reduced risk (p = 0.006). Pre-existing neurological deficits (p = 0.04) and age > 65 years (p = 0.03) were associated with an increased risk of tumor progression. During a median radiological follow-up of 43 months (IQR 49) after SRS, 33% of chordomas progressed, 40% remained stable, and 27% shrank. A maximal dose > 29 Gy was associated with improved tumor control (p = 0.02). The 5-year and 10-year progression-free survival rates were 54.7% and 34.7%, respectively. Among the 13 patients who died during the follow-up, 10 patients (77.0%) had tumor progression as a primary or contributing cause of death. The 5-year and 10-year overall survival rates were 83% and 70%, respectively. Age > 65 years at SRS treatment was associated with an increased risk of mortality (p = 0.01).
Microsurgical resection (R0) and/or therapeutic radiation are currently recommended treatment methods for the diagnosis and recurrence of intracranial chordomas, aiming to preserve or restore neurological function and maintain quality of life. Despite this initial treatment approach, the 5-year and 10-year recurrence-free survival rates and local control rates for chordomas are reported to be 47%-76% and 42%-71%, respectively. Furthermore, due to radiation damage to adjacent brainstem, temporal lobe, or cranial nerves, traditional fractionated radiotherapy may not achieve the high doses of re-irradiation required to control chordomas. Proton therapy has been reported to better control local tumors compared to conventional radiotherapy. A systematic review of 11 studies, including 511 patients receiving adjuvant proton beam therapy, reported a recurrence rate of 26.8% with a mean follow-up of 45 months. In the current multimodal management study, 33.3% of patients experienced tumor progression at a median follow-up of 43 months (IQR 49). Therefore, according to published studies, the outcomes of single-session SRS and proton beam therapy for clival chordomas are comparable. This study and previously published studies suggest that highly conformal single-session SRS is an important additional option for chordomas, particularly in patients with small-volume tumors adjacent to critical brain and cranial nerve structures. The precise targeting and steep dose gradients provided by SRS allow for the delivery of radiation doses to the tumor while preserving the adjacent neurovascular structures, brain, brainstem, and cranial nerve structures.
SRS has been used as part of multimodal treatment for selected adult and pediatric intracranial chordomas. In 2011, Kano et al. reported 71 patients with skull base chordomas who underwent Gamma Knife radiosurgery. Following SRS treatment, the median follow-up was 5 years (range 0.6 – 14 years), with 23 patients dying from tumor progression. The 5-year actuarial overall survival and tumor control rates were 80% and 66%, respectively. In multivariate analysis, younger age, no prior history of radiotherapy, and no or single cranial nerve involvement were associated with longer survival after SRS treatment, while younger age and higher marginal doses were associated with improved local tumor control. The authors concluded that SRS is best suited for medium-sized chordomas and is part of a multimodal treatment strategy that includes resection when feasible. Hasegawa et al. evaluated 37 patients with skull base tumors who underwent SRS, of which 30 underwent biopsy (n = 27) or radiological diagnosis of chordoma (n = 3), with a mean tumor volume of 20 cm3, and mean marginal dose of 14 Gy. The 5-year and 10-year actuarial overall survival rates were 80% and 53%, and the 5-year and 10-year actuarial local tumor control rates were 76% and 67%, respectively. Tumor volumes < 20 cm3 were associated with improved local tumor control. One patient experienced facial numbness following SRS. The authors suggested that SRS adjuvant therapy is a reasonable treatment choice for patients with residual tumors < 20 cm3. A marginal dose of ≧ 15 Gy should be used to achieve local tumor control. Krishnan et al. reported 29 patients with skull base tumors who underwent SRS, of which 25 were chordomas. During an average clinical and imaging follow-up of 4.8 and 4.5 years, 28% (7/25) of chordoma patients experienced tumor progression, with 3 dying due to tumor progression. The 5-year actuarial chordoma control rate was 32%, and the 5-year actuarial progression-free survival rate was 67%. 10 patients (34%) experienced radiation-related complications, including 6 (21%) cranial nerve deficits, 5 (17%) brain necrosis, and 3 (10%) pituitary function deficits. No radiation-related complications were observed in patients who exclusively received SRS treatment.
The current study represents the largest series of patients utilizing SRS as part of a multimodal treatment strategy for residual or recurrent intracranial chordomas. Younger age and larger radiation doses > 29 Gy were associated with better tumor control and improved patient outcomes prior to the onset of neurological deficits. Our data supports the concept that early SRS treatment following incomplete resection may further improve prognosis.
Conclusion:
SRS appears to be a safe and relatively effective adjuvant treatment option for intracranial chordomas, with the best outcomes achieved in younger patients without significant neurological deficits. Further well-designed studies are needed to determine the optimal timing for SRS treatment in the multidisciplinary management of intracranial chordomas.
The treatment of skull base chordomas is challenging and requires a multidisciplinary approach. In our study, patients who received SRS treatment as part of their management had a 10-year progression-free survival rate and overall survival rate of 34.7% and 70%, respectively. Age > 65 years was associated with a high risk of tumor progression and decreased overall survival rates. A maximal radiosurgical dose > 29 Gy was associated with improved chordoma control and reduced risk of neurological deterioration. Additionally, pre-existing neurological deficits and tumor progression following SRS were associated with local SRS failure and neurological deterioration following SRS treatment. These factors suggest that early SRS treatment may have potential benefits for patients with previously incompletely resected chordomas. Further well-designed studies are needed to determine the role of SRS in the treatment of intracranial chordomas.