Recently, many friends have reported that they often do not receive our articles?The reason is that the public account has pushed updates.You need to give us a little “like”, set the testing starry sky as “starred”, hurry up and move your little fingers!Progress a little every day!
Source: Laboratory Medicine Network
Author: Liver Disease Research Center, Luohu People’s Hospital, Shenzhen, Xu Kecheng
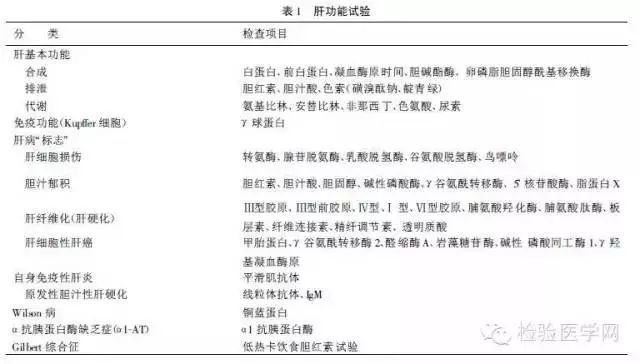
The liver has the functions of synthesis, excretion, and metabolic transformation. The narrow definition of liver function tests refers to tests that reflect the basic functions of the liver mentioned above, while the broad definition of liver function tests also includes tests for liver pathological states or liver disease “markers” (see Table 1). Therefore, the correct term should be liver tests.
One tests reflecting liver synthetic function
1. Serum albumin: The liver is the only site for albumin synthesis. When liver function is impaired, serum albumin levels decrease. In patients with liver cirrhosis without ascites, serum albumin levels reflect prognosis. In cases of cirrhosis where the proportion of albumin in total protein is <45%, the 3-year survival rate is half that of those with a proportion >45%. If albumin rises after treatment, it suggests that the patient’s recent prognosis is good; if it cannot rise, or further declines below 20g/L, the prognosis is poor. When evaluating the clinical significance of serum albumin, the following facts need to be considered.
Albumin has a half-life of up to 21 days in the body, and the decrease in albumin after liver damage often does not show until a week after the illness. In cases of acute severe hepatitis where death occurs rapidly, serum albumin often does not show a decrease. Therefore, serum albumin is not a good indicator of acute liver disease.
The decrease in serum albumin levels may be due to:
① Expansion of the extravascular pool. The adult body has a total exchangeable albumin of 500g, of which 40% is distributed in the vascular system and 60% in various organs, tissues, and interstitial fluid (the extravascular pool). If the patient has ascites or edema, albumin from the vascular system enters the extravascular pool, which can lead to a decrease in serum levels.
② Insufficient supply of amino acids (especially tryptophan) required for albumin synthesis, which can occur due to insufficient intake or digestive absorption disorders.
③ Excessive protein breakdown. Normal individuals break down about 11g of albumin daily; during infections, fever, or cancer, albumin breakdown increases.
④ Abnormal loss through unusual pathways. Normal individuals lose about 1g of albumin from the intestinal mucosa daily. In protein-losing enteropathy, losses increase. In conjunction with kidney disease, albumin can be lost through the kidneys.
In liver disease, the decrease in serum albumin may also be due to abnormalities in the regulation of albumin synthesis. In fact, in liver cirrhosis, the synthesis rate of albumin by liver cells may not necessarily decrease; it may even increase. It is currently believed that the synthesis of albumin by liver cells is influenced by osmotic pressure, which is primarily determined by globulin. Patients with liver cirrhosis often have elevated globulin levels, which can inhibit albumin synthesis by increasing osmotic pressure.
2. Prealbumin: Like albumin, prealbumin is also synthesized by the liver. However, because its half-life is only 1.9 days, its serum levels decrease early in liver disease and show changes more clearly. As the condition improves, prealbumin quickly returns to normal. However, in patients with severe hepatitis, it often remains low. For the course of acute hepatitis, prealbumin is indeed a valuable indicator. However, in nephrotic syndrome, serum prealbumin not only does not decrease but may even increase slightly, for reasons that are unclear.
3. Prothrombin time (PT): The liver synthesizes six coagulation factors: I (fibrinogen), II (prothrombin), IV, V, VI, and VII. When they are deficient individually or in combination, PT is prolonged, making PT a useful indicator for studying liver synthetic function. In acute hepatocellular disease, prolonged PT suggests a high likelihood of fulminant liver failure. In alcoholic liver disease, 60% of deaths have PT prolonged by more than 4 seconds, while only 10% of survivors have PT prolonged to this level. In chronic liver disease, prolonged PT also indicates poor long-term prognosis. In cases of cirrhosis and portal hypertension, PT can be used to predict the risk of intra-abdominal shunt surgery.
However, prolonged PT is not unique to liver disease; it can also be seen in congenital coagulation factor deficiencies, consumptive coagulopathy, vitamin K deficiency, and after the use of anticoagulant drugs (such as coumarin). Prolonged PT may also be due to:
(1) The liver’s inability to effectively clear activated coagulation factors and coagulation inhibitors from plasma;
(2) Impaired function of the liver to synthesize plasminogen;
(3) Primary fibrinolysis;
(4) Accompanied by disseminated intravascular coagulation.
4. Lecithin-cholesterol acyltransferase (LCAT): This enzyme is synthesized and secreted by the liver. When liver cells are damaged, LCAT synthesis decreases, and the degree of decrease in serum LCAT parallels the severity of liver damage. Like albumin and ChE, LCAT can reflect liver reserve function but is more sensitive than them.
Two tests reflecting liver excretory function
1. Bilirubin metabolism test: The liver has the functions of uptake, conjugation, and excretion of bilirubin. If any one or several of these functions are impaired, jaundice can occur. Checking bilirubin metabolism is of great significance for judging liver function and differentiating jaundice.
The main value of measuring total serum bilirubin lies in discovering hidden jaundice. The daily production of bilirubin is less than 50mg, but a normal liver can process up to 150mg of bilirubin daily. Due to the liver’s large reserve capacity for processing bilirubin, total serum bilirubin is not a sensitive indicator of liver function. Although bilirubin concentration is significantly elevated in liver disease, reflecting more severe liver damage, this is not always the case. For example, in fulminant hepatitis, serum bilirubin may only be mildly to moderately elevated; in cholestatic hepatitis, although liver cells are relatively lightly affected, serum bilirubin can be significantly elevated.
Measuring serum direct bilirubin may help in the early diagnosis of certain liver and biliary diseases. In cases of viral hepatitis before jaundice or non-jaundiced hepatitis, compensated cirrhosis, or partial biliary obstruction, about 30%-50% of cases show elevated serum direct bilirubin, while total bilirubin remains within normal limits. In some cases, even after total bilirubin returns to normal, direct bilirubin may still be elevated; the main clinical use of measuring direct bilirubin is to diagnose hyperbilirubinemia with high unconjugated bilirubin, where total bilirubin is elevated, while direct bilirubin is normal.
Urinary bilirubin and urobilinogen measurement have certain value for the early diagnosis and differential diagnosis of jaundice, and the methods are simple and can yield immediate results, so they should still be classified as routine tests.
2. Bile acid metabolism test: Bile acids are the main organic anions excreted by the early liver. In liver disease, serum bile acids and bilirubin can be compared to serum creatinine and urea nitrogen in kidney disease. Since the metabolism of bile acids, like creatinine, is mainly controlled by the organ responsible for their excretion, the liver, it can more specifically reflect the liver’s excretory function. Therefore, theoretically, measuring serum bile acids can be more sensitive than bilirubin in reflecting liver function abnormalities.
From current data, measuring serum bile acids is a moderately sensitive and specific test for liver disease. This test is mainly used for:
① Differentiating liver and biliary diseases from congenital or hemolytic jaundice, where the latter tests are normal;
② Monitoring the course of liver disease and assessing treatment efficacy;
③ Confirming the hepatic origin of certain enzyme tests (transaminases, alkaline phosphatase) that are abnormal;
④ Some believe that measuring the bile acid/deoxycholic acid ratio helps differentiate hepatocellular obstructive jaundice.
3. Pigment excretion test: The liver can excrete certain exogenous pigments such as sulforhodamine sodium (BSP), whose transport mechanism differs from that of endogenous organic anions (such as bile acids). Therefore, measuring the liver’s transport of pigments can reflect liver function from another aspect.
Measuring the BSP retention rate is one of the most sensitive screening tests for liver disease, with a higher positive rate than most other liver function tests. For example, if the BSP retention rate is <5%, it cannot be liver cirrhosis; if >14%, the liver cannot be normal. However, since BSP can occasionally cause allergic reactions and even be fatal, it is no longer used as a routine test except for the diagnosis of Dubin-Johnson syndrome (where the BSP retention rate shows a biphasic change).
ICG is rapidly excreted by the liver, disappears quickly from the blood, and has minimal reflux from the liver, with few side effects. It has replaced BSP and become the most valuable and practical pigment for screening liver disease and detecting liver damage. Clinically, the 15-minute blood retention rate of ICG is often measured. It is generally believed that the clinical significance of the ICG test is basically the same as that of the BSP test. Some believe that in diagnosing non-jaundiced hepatitis, or monitoring outcomes, and diagnosing occult or inactive liver cirrhosis, the ICG test is more sensitive than the BSP test. In Dubin-Johnson syndrome, there is no phenomenon of ICG retention rate rising.
Three tests reflecting liver metabolic function
Inject substances that can be selectively metabolized by the liver (drugs); measuring the metabolic rate of these substances in the body can reflect the number of functional liver cells or the liver’s metabolic capacity. The ideal drug should meet the following conditions:
① Non-toxic, mainly cleared by the liver.
② Can be intravenously injected or rapidly absorbed after oral administration.
③ The measurement of these drugs or their metabolites in plasma, urine, or breath should be simple, feasible, and reproducible.
④ The liver’s excretion of the drug mainly depends on the number of functional liver cells (metabolic capacity) rather than on liver blood flow. Drug metabolism is mainly completed by the microsomal enzyme system.
⑤ Does not bind to plasma proteins, and its metabolism is not affected by plasma protein levels.
Currently, tests used to reflect metabolic function mainly include measuring the plasma clearance rate of antipyrine, the 14C-aminopyrine breath test, the galactose clearance rate, and the maximum synthesis rate of urea. However, these tests are not sensitive screening tests for liver disease. The current trend is to use them as non-invasive indicators for estimating the prognosis of severe liver disease. With the development of liver transplantation, systematically testing these tests may be beneficial for determining the optimal timing for liver transplantation. Currently, these tests have not been widely applied, partly because they do not provide more information than conventional liver function tests, and also due to individual differences in results from single-drug tests or different drug tests, making result interpretation difficult.
Four tests reflecting liver immune function
The liver contains abundant Kupffer cells, which act as the second line of defense for the digestive tract, phagocytizing large molecules from the portal vein and systemic circulation, such as microorganisms, endotoxins, foreign antigens, and immune complexes, eliminating the immunogenicity of antigens, thus preventing harmful substances from entering the body from the intestine while also reducing the body’s response to foreign antigens, preventing hypersensitivity reactions and tissue damage.
The serum globulin level reflects the liver’s above functions to some extent. When liver damage occurs, Kupffer cell dysfunction occurs, and measuring serum globulin or various immunoglobulins can serve as a marker for monitoring the integrity of liver immune function.
Five markers reflecting liver cell damage
1. Transaminases: Serum transaminases mainly include alanine transaminase (ALT) and aspartate transaminase (AST). The liver is rich in these two enzymes; as long as 1% of liver cells are damaged, the released transaminases are sufficient to raise serum transaminase levels by 1 fold; within the liver, transaminases are mainly contained within liver cells, with an intracellular/extracellular enzyme activity ratio of 5000/1. When liver cells undergo degeneration and necrosis, the enzymes within the liver are released into the blood, causing an increase in serum transaminase activity.
So far, measuring serum transaminases is still considered the standard test for reflecting liver cell damage. However, when judging results, attention should be paid to the following:
① Various liver diseases can cause elevated serum transaminases, but levels exceeding 10 times normal are mainly seen in acute viral or drug-induced hepatitis, ischemia leading to liver hypoxia, and acute right heart failure causing liver congestion.
② In acute liver disease, the level of serum transaminases does not proportionally reflect the degree of liver damage. It is now believed that the elevation of transaminases in liver disease is due not only to enzyme release from necrotic liver cells but also due to excessive production of transaminases by surviving liver cells. In typical hepatitis, liver damage is mainly characterized by liver cell degeneration, and a large number of non-necrotic liver cells excessively produce transaminases, leading to significantly elevated serum enzyme levels; in severe hepatitis, liver cells are mostly necrotic, with no ability to produce transaminases, resulting in no significant increase in serum enzyme levels.
③ In chronic liver disease, transaminase levels reflect disease activity. If transaminases are more than 10 times normal and accompanied by a 1-fold elevation in globulin, and persist for more than 8 weeks, it is almost certain to be chronic active liver disease.
④ In biliary diseases, transaminases also increase, generally not exceeding 8 times normal. In a few cases of common bile duct stones, transaminases can be as high as 10 times normal, but they decrease significantly or return to normal within 24-48 hours.
⑤ In alcoholic liver disease, transaminases are mildly elevated, which may be related to the exhaustion of pyridoxal, a coenzyme for ALT.
To improve the diagnostic and differential diagnostic value of serum transaminase measurements, further measurements can be made:
① AST/ALT ratio. Within liver cells, ALT is mainly distributed in the cytoplasmic aqueous phase, while AST is mainly distributed in mitochondria, with a small amount in the aqueous phase. When liver cells degenerate and the cell membrane permeability increases, the main enzyme escaping from the cells is ALT, while when liver cells are severely damaged and necrotic, AST in the mitochondria is released into the blood. In mild hepatitis, the AST/ALT ratio decreases, while in severe hepatitis, the ratio increases; therefore, measuring this ratio can serve as an indicator of the severity of liver damage. However, this value also increases in cirrhosis and liver cancer for unknown reasons.
② Measurement of AST isoenzymes. Mitochondrial AST (ASTm) significantly elevated reflects severe liver damage.
2. Adenosine deaminase (ADA): The activity of this enzyme increases in the liver and is similar to transaminases in reflecting acute liver damage.
However, serum ADA measurements have advantages that transaminases do not possess:
① Clinically, it has been found that during the recovery phase of acute hepatitis, the positive rate of ADA elevation is higher than that of transaminases, suggesting that it reflects residual lesions of hepatitis better than the latter. This may be because ADA molecules are smaller than transaminases, making it easier to enter the blood through the tissue-blood barrier when liver cell lesions are mild;
② In chronic liver disease, especially cirrhosis, the positive rate of ADA is higher than that of transaminases.
③ In obstructive jaundice, ADA remains normal, thus helping to differentiate jaundice.
3. Lactate dehydrogenase (LDH): In liver disease, serum LDH is elevated, but its sensitivity is far inferior to that of transaminases, and it also rises in many extrahepatic diseases such as myocardial infarction, pulmonary embolism, and hemolysis, thus lacking specificity for liver disease. In terms of liver disease, the main value of LDH measurements lies in its isoenzymes. There are five isoenzymes of LDH: LDH1-5, with LDH1 mainly present in the myocardium and LDH5 mainly found in striated muscle and the liver. In normal individuals, serum LDH2 > LDH1 > LDH3 > LDH4 > LDH5; in myocardial lesions, LDH increases with LDH1 > LDH2, while in liver disease, LDH5 increases with LDH5 > LDH4.
4. Glutamate dehydrogenase (GDH): This enzyme is mainly present in the liver and is only found in mitochondria. Therefore, theoretically, measuring serum GDH is more sensitive and specific than transaminases. However, GDH elevation is transient, and the degree of elevation is smaller than that of transaminases. GDH activity in the central acinus of the liver is 1.7 times higher than that in the peripheral acinus. In alcoholic liver disease, liver damage mainly occurs in the central acinus, so serum GDH activity can serve as a good indicator of alcoholic liver disease.
Six
markers reflecting cholestasis
In addition to serum bilirubin and bile acids being significantly elevated during cholestasis, there are also:
1. Serum cholesterol: Whether intrahepatic or extrahepatic cholestasis, serum cholesterol often exceeds 7.8mmol/L, especially in chronic cases, it can rise to over 26mmol/L; in cases of biliary obstruction caused by cancer, cholesterol levels are often higher than in cases of common bile duct stones. The elevated cholesterol in serum during cholestasis is mainly free cholesterol; the absolute content of cholesterol is generally normal, but the proportion of total cholesterol decreases. If liver cell damage occurs, the absolute content of cholesterol esters also decreases.
2. Alkaline phosphatase (ALP): ALP is mainly distributed in the liver, bone, intestine, and placenta. The serum ALP mainly comes from the liver and bone, with some coming from the intestine in O and B blood types. Serum ALP is elevated to more than 2.5 times normal. If transaminases do not exceed 8 times normal, 90% of the cases are due to cholestasis; conversely, 90% are due to viral hepatitis. In cholestasis, serum ALP elevation often parallels bilirubin levels; in intrahepatic occupying lesions, especially liver cancer, ALP may often be elevated even without jaundice. A disadvantage of ALP testing is that it also increases in bone disease.
Using polyacrylamide gel electrophoresis, ALP can be divided into seven isoenzymes, namely ALP I-VII, among which ALP VII is high molecular weight ALP, mainly seen in extrahepatic cholestasis.
3. Gamma-glutamyl transferase (GGT): Similar to ALP, serum GGT elevation is mainly seen in cholestasis and intrahepatic occupying lesions; its advantage is that it does not elevate in bone disease. However, GGT is widely distributed in the body and can easily be induced by drugs (such as phenobarbital, phenytoin, sedatives, alcohol), so its specificity for liver disease is not as high as that of ALP. Some believe that GGT can serve as a sensitive screening test for liver disease; if serum GGT is normal, liver disease can almost be ruled out.
4. 5′-nucleotidase (5′-NT): The clinical significance of measuring this enzyme is similar to that of ALP, but its specificity is higher than that of ALP. Although 5′-NT is distributed in multiple organs, its increased activity in serum is only seen in liver disease patients.
5. Lipoprotein X (LPX): This is a special lipoprotein that is absolutely absent in normal serum. It is occasionally seen in rare cases of intrahepatic cholestasis. In terms of diagnosing and excluding cholestasis, the sensitivity and specificity of LPX surpass all known biochemical tests. However, LPX testing alone cannot differentiate between intrahepatic and extrahepatic cholestasis.
Seven markers reflecting liver fibrosis (cirrhosis)
So far, routine liver function tests cannot diagnose liver fibrosis or early cirrhosis. The presence of a β-γ bridge on protein electrophoresis is specific for cirrhosis, but only occurs in the late stages of cirrhosis and is mainly seen in alcoholic cirrhosis. The essence of liver fibrosis is the proliferation of connective tissue in the extracellular matrix, mainly composed of collagen, as well as various glycoproteins and proteoglycans. Measuring these components and their degradation products in serum, as well as enzymes involved in their metabolism, can assist in diagnosing liver fibrosis.
1. Collagen and its metabolites: There are various types of collagen, and types I, III, IV, V, and VI are present in the liver, with types I and III being the most common. Currently, measuring serum type III procollagen amino-terminal peptide (PⅢP) is more frequently used to diagnose liver fibrosis. In the early or compensated stages of cirrhosis, the liver mainly synthesizes and deposits procollagen, and serum (PⅢP) can remain >100ng/mL. However, recent studies have found that serum PⅢP can also significantly increase during liver inflammation and necrosis, possibly due to increased degradation of pre-existing collagen, leading some to believe that serum PⅢP is only related to liver inflammation, necrosis, and fibrosis. However, most scholars believe that serum PⅢP is related to liver inflammation, necrosis, and fibrosis, with a primary correlation to liver fibrosis.
2. Serum type III procollagen (PC3): This is positively correlated with the degree of liver fibrosis and has similar clinical significance to PⅢP, and its influence on serum PC3 during liver inflammation and necrosis is minimal. Therefore, it is believed that serum PC3 measurement may be superior to serum PⅢP in diagnosing liver fibrosis.
3. Type V collagen: This is an important component of the basement membrane. Serum type V collagen increases in patients with chronic active hepatitis and cirrhosis, with cirrhosis being higher than in the chronic liver disease group. Some have measured serum type I collagen (C1) and compared it with PⅢP, finding that serum C1 is more reflective of the degree of liver fibrosis than PⅢP during cirrhosis.
4. Collagen metabolism-related enzymes: Prolyl hydroxylase (PH) is a key enzyme in collagen synthesis, composed of α and β subunits forming a tetramer. In liver biopsy tissues of cirrhosis patients, PH content is significantly elevated. Serum PH detection is more difficult, as less than 10% of active PH tetramers exist, and inhibitors are present in the blood. Using RIA to measure serum immunogenic PH (SIRPH) reveals that its level is correlated with PH activity in liver tissue, but specificity is not high. Some have used PH subunit monoclonal antibodies to measure serum immunogenic PH subunits (SIRPH), believing this may improve specificity.
5. Non-collagen proteins: This includes glycoproteins and proteoglycans. Among the glycoproteins that can be detected in the blood and have clinical significance are laminin, fibronectin, and elastin (UN). These glycoproteins can be elevated in the serum of patients with cirrhosis, with laminin being particularly valuable.
6. Hyaluronic acid (HA): This is a glycosaminoglycan. With the progression of hepatitis, from acute hepatitis to chronic hepatitis to cirrhosis, HA levels increase sequentially, with a critical value for diagnosing cirrhosis proposed at 250μg/L.
Currently, it seems that serum markers for diagnosing liver fibrosis are not perfect. A more acceptable approach is to measure markers with different mechanisms, such as PⅢP primarily reflecting active liver fibrosis, laminin mainly reflecting basement membrane proliferation, and prolyl hydroxylase primarily reflecting collagen degradation. Measuring the aforementioned markers together can increase diagnostic sensitivity and specificity.
Eight markers reflecting liver cancer
The serum markers for hepatocellular carcinoma can be divided into:
① Those with relatively high specificity include alpha-fetoprotein (AFP), gamma-glutamyl transferase isoenzyme II (GGT II), alkaline phosphatase 1 (ALP1), prothrombin, alpha-L-fucosidase, and aldose reductase isoenzyme A;
② Non-specific to liver cancer but valuable for diagnosing gastrointestinal cancers include glutathione-S-transferase, 5′-nucleotidase V, alpha1-antitrypsin, alpha1-antichymotrypsin, ferritin, and acid ferritin.
1. AFP: So far, serum AFP remains the most important marker for hepatocellular carcinoma, with a positive rate of 60-70%. If serum AFP >400μg/L (RIA), sustained for 4 weeks, and transaminases are normal, hepatocellular carcinoma should be highly suspected.
For increases in serum AFP caused by non-cancerous liver diseases, differentiation can be made through AFP variants. The conA-bound AFP increase is mainly seen in hepatocellular carcinoma and cirrhosis, while the conA unbound AFP is more common in embryonic cancer and metastatic liver cancer; the LCA unbound AFP is more common in cirrhosis and chronic hepatitis, while the LCA bound AFP is more common in liver cancer.
2. GGT II: Using polyacrylamide gel gradient electrophoresis, serum GGT can be divided into 11-13 bands, among which band II, i.e., GGT II, has diagnostic value for hepatocellular carcinoma. Our studies have found that GGT II has a sensitivity of 86%-90% for diagnosing liver cancer and a specificity of 97.1%; in patients with AFP <50ng/mL, the positive rate of GGT II also reaches 70.8%, suggesting that combined testing has complementary value; in patients who are GGT II positive without other evidence of liver cancer, follow-up for a year found that 24.2% developed liver cancer; in small liver cancers <5cm in diameter, the positive rate of GGT is as high as 78.6%, indicating that GGT II has early diagnostic significance for liver cancer. It is now believed that GGT II is the best marker for liver cancer besides AFP, but its testing method is relatively complex.
3. ALP1: In agarose electrophoresis, serum ALP can be divided into seven bands, among which ALP1 is specific for liver cancer, but unfortunately, its sensitivity is poor, with a positive rate of only 16%.
4. Alpha-L-fucosidase (AFU): According to reports, a serum AFU ≥10mmol/mL/min is the diagnostic limit, with a sensitivity of 75%, specificity of 90%, and accuracy of 84% for diagnosing liver cancer.
5. Des-γ-carboxylated prothrombin (DCP): About 70% of liver cancer cases have serum DCP levels exceeding 300μg/L, while benign liver diseases do not exceed 40μg/L.
6. Aldose reductase isoenzyme A (ALD-A): There are three isoenzymes of ALD: A, B, and C, originating from muscle, liver, and brain, respectively. In normal individuals, serum ALD is primarily of type B. In liver cancer, type A increases, while type B decreases or even disappears. ALD-A has a sensitivity of approximately 80% for liver cancer diagnosis.
7. Alpha1-antitrypsin (α1AT) and alpha1-antichymotrypsin (α1AC): Our findings show that in the liver cancer group, serum α1AT and α1AC elevations were found in 74.5% and 68%, respectively, with their average serum concentrations significantly higher than those in the normal group and various benign liver disease groups. In the liver cancer group, simultaneous elevation of both markers occurred in 60%; if either one or both are elevated, the total positive rate for liver cancer reaches 80%. α1AT and α1AC have complementary value with AFP; if all three are tested simultaneously, 96% of liver cancer cases can be diagnosed.
Selection and Application of Tests
The principles and clinical significance of various tests have been introduced above. In clinical practice, how to select these tests and combine them is a practical issue faced by clinicians. From the perspective of clinical application, liver function tests are mainly used to detect liver damage, differentiate jaundice, assess prognosis, and diagnose specific liver diseases.
1. Detecting liver damage
Various enzyme tests reflecting liver and biliary damage are mainly selected, among which transaminases (ALT, AST), alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT) are the most commonly used. When interpreting results, attention should be paid to the following issues:
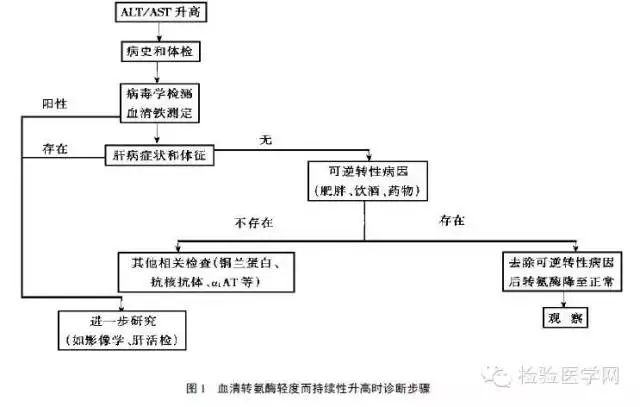
1. Asymptomatic elevation of transaminases: In routine health check-ups or when conducting routine liver function tests due to other diseases, about 5-10% of patients show elevated serum transaminases without liver disease symptoms. For those with mild elevations, short-term re-examination can be done to rule out testing errors; if transaminases are elevated in two consecutive tests, or if moderate elevations are present, the cause should be investigated. The reasons for elevated transaminases can vary by region and ethnicity. In Asia, including China, Africa, etc., viral hepatitis, especially hepatitis B and C, malaria, and schistosomiasis are often the main causes. In some Western countries, hepatitis C and autoimmune liver diseases are among the main causes. In overweight individuals and drinkers, fatty liver or alcohol-related liver disease should be considered. A report indicated that 5% of cases of elevated transaminases were due to drug-induced hepatitis. Additionally, some rare diseases should also be noted; one report indicated that 7% of asymptomatic transaminase elevations were due to hemochromatosis and α1-antitrypsin deficiency. For patients with mildly persistently elevated serum transaminases, careful inquiry of medical history and physical examination should be performed, and viral immunological tests conducted; if necessary, imaging and liver histological studies should be done (see Figure 1).
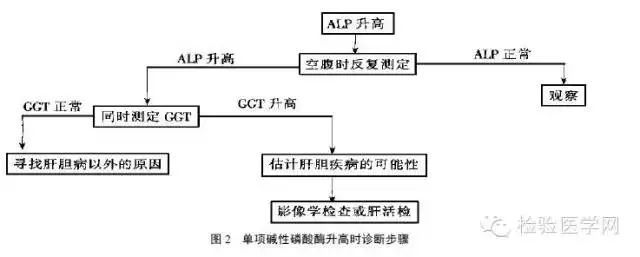
2. Isolated elevation of alkaline phosphatase (ALP) while gamma-glutamyl transferase (GGT) is normal: Whenever serum ALP is elevated, GGT should also be measured (see Figure 2). If GGT is also elevated, it indicates that the lesion is in the liver and biliary system; if GGT is normal, the cause should generally be sought outside the liver and biliary system. Rapid bone growth (such as in children), bone diseases (such as Paget’s disease), or pregnancy can often lead to these changes. Some rare liver diseases can also present similar abnormalities, such as Byler’s disease, BRIC, and congenital bile acid synthesis defects. Byler’s disease is a fatal autosomal recessive hereditary cholestasis with an unclear pathogenesis, and orthotopic liver transplantation is the only treatment. BRIC is a familial idiopathic syndrome characterized by recurrent, self-limiting intrahepatic cholestasis, which can last for several months, accompanied by cold-like symptoms and abdominal pain, with elevated serum ALP and bilirubin, while transaminases and GGT remain basically normal. The genes for Byler’s disease and BRIC are located on the long arm of chromosome 18.
3. Isolated elevation of serum GGT: In patients with elevated GGT and normal ALP, careful investigation of medication and alcohol history should be conducted, as most anticonvulsants, warfarin, and alcohol can cause GGT elevation. If there is such a medical history, re-examination should be performed after stopping the medication or abstaining from alcohol.
4. Analyzing the degree of elevation, duration, and relationships with other indicators of serum transaminases can help significantly in the differential diagnosis of liver disease. Significantly elevated transaminase levels are almost only seen in acute damage. Ischemic hepatitis or “shock liver” is a consequence of acute liver circulatory failure, often seen in acute and chronic heart failure, myocardial infarction, arrhythmia, sepsis, extensive burns, severe trauma, or heat stroke, and low blood pressure may not necessarily be present. Characteristic changes include a sudden rise in transaminases (up to dozens of times normal), lasting about a week before returning to normal ranges, followed by a mild temporary rise in serum bilirubin and alkaline phosphatase. LDH is often significantly elevated. Prothrombin time is rarely prolonged by more than 3 seconds. Although transaminases are significantly elevated, ischemic hepatitis is usually subclinical. In toxic hepatitis, transaminase elevation is often also transient, while in drug-induced liver injury, enzyme elevation generally lasts longer than in ischemic hepatitis. In acute viral hepatitis, regardless of type, transaminases are significantly elevated, lasting about a month, unlike in ischemic/toxic liver damage. Serum LDH is often only mildly elevated in acute viral hepatitis. In severe cases, PT is often significantly prolonged.
2. Differentiating jaundice
Generally, jaundice can be differentiated based on serum bilirubin, bile acids, transaminases, alkaline phosphatase, gamma-glutamyl transferase, and other tests. In practical application, the following procedures can be followed:
1. Confirming the presence of jaundice: Yellowing of the skin and mucous membranes may be due to jaundice or pigmentation or drug staining, such as excessive intake of carotenoids (carrots, citrus, papaya, pumpkin, etc.) or large doses of amitriptyline can cause skin and mucous membrane yellowing, clinically referred to as pseudo-jaundice. Measuring serum bilirubin can help differentiate this, as serum bilirubin remains normal in pseudo-jaundice.
2. Clarifying which type of hyperbilirubinemia is present, i.e., whether it is unconjugated hyperbilirubinemia or conjugated hyperbilirubinemia, can be achieved by measuring serum direct bilirubin. In unconjugated hyperbilirubinemia, total serum bilirubin is elevated (generally not exceeding 85μmol/L), with direct bilirubin accounting for less than 25% of total bilirubin, while in conjugated hyperbilirubinemia, direct bilirubin accounts for more than 40%.
3. Urinary bilirubin and urobilinogen can also be measured; in conjugated hyperbilirubinemia, urinary bilirubin is positive with decreased urobilinogen (obstructive jaundice) or increased urobilinogen (hepatocellular jaundice); in unconjugated hyperbilirubinemia, urinary bilirubin is negative while urobilinogen is increased.
4. If it is unconjugated hyperbilirubinemia, the underlying cause should be clarified; in suspected hemolytic jaundice, peripheral blood cells, reticulocytes, bone marrow smears, and relevant immunological indicators can be tested; if there is no evidence of hemolysis, Gilbert’s disease should be considered, and a low-dose phenobarbital test can be performed to confirm the diagnosis.
5. If it is conjugated hyperbilirubinemia, it should be differentiated whether it is hepatocellular jaundice or obstructive cholestasis; in conjugated jaundice, serum direct bilirubin often exceeds 60% of total bilirubin, while in hepatocellular jaundice, it exceeds 40%, but in practice, there is significant overlap between the two types, which does not help differentiate them. Simultaneously measuring serum transaminases, ALP, and GGT has diagnostic significance. If transaminases are more than 10 times normal while ALP is less than 2.5 times normal, it leans towards hepatocellular jaundice; conversely, it leans towards obstructive jaundice. Serum bile acids and cholesterol are significantly elevated in obstructive jaundice; LPX is positive in obstructive jaundice and negative in hepatocellular jaundice.
6. If it is hepatocellular jaundice, the cause should be clarified; various liver diseases, including all types of viral hepatitis and markers for hepatocellular carcinoma, can be tested.
7. If it is obstructive jaundice, it should be clarified whether it is intrahepatic cholestasis or extrahepatic biliary obstruction. Currently, there is no biochemical test that can effectively differentiate between the two types of obstructive jaundice. The ratio of alcohol dehydrogenase isoenzyme Am/Et activity measurement has certain value and can serve as a reference. The development of imaging examinations has made it easy to differentiate between intrahepatic and extrahepatic cholestasis, so biochemical tests are no longer of major importance.
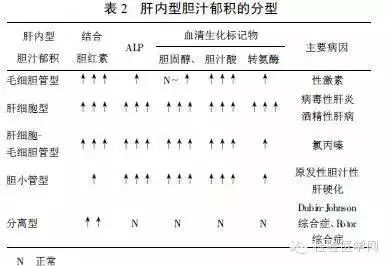
8. If it is intrahepatic cholestasis, the underlying cause should be further clarified; based on changes in serum direct bilirubin, ALP, bile acids, cholesterol, and transaminases, it can be classified into canalicular cholestasis, hepatocellular cholestasis, hepatocellular-canalicular cholestasis, ductal cholestasis, and isolated cholestasis. This classification is of certain significance for identifying the cause and guiding treatment (see Table 2).
3. Assessing prognosis
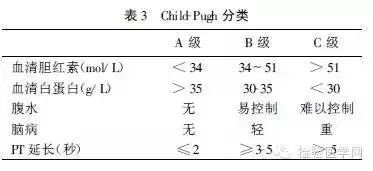
Based on serum albumin, bilirubin, and prothrombin time (PT), the prognosis of liver disease patients can be estimated. In fulminant liver failure, prolonged prothrombin time and progressive elevation of bilirubin are poor prognostic indicators. The Child-Pugh classification based on serum bilirubin, albumin, and prothrombin time accurately reflects the prognosis of chronic liver disease and helps assess the risk of surgery. The Child-Pugh classification was originally used to estimate the prognosis of liver disease patients after portosystemic shunt surgery, and is now also used as an indicator for estimating prognosis after non-portosystemic shunt surgery. In a prospective study, 100 patients with cirrhosis (mostly alcoholic) underwent abdominal surgery, with a mortality rate of 10% in Class A patients, 31% in Class B, and as high as 76% in Class C. The Child-Pugh classification is also correlated with postoperative complications such as renal failure, hepatic encephalopathy, bleeding, infection, refractory ascites, and liver function deterioration. In Class A patients, the surgical risk is only moderately increased, while in Class B, C, or cirrhotic patients, the surgical risk is significantly increased; in these patients, surgery (such as portosystemic shunt surgery) should be avoided as much as possible, delayed, or liver transplantation performed.
If surgery is necessary, adequate preoperative preparation and postoperative care should be done, and avoid using drugs that can cause or exacerbate low blood pressure, kidney toxicity, liver damage, or brain disease (such as sedatives).
For many chronic liver diseases, using general biochemical tests often makes it difficult to correctly predict prognosis. With the development of liver transplantation, accurately estimating the number of functional liver cells and measuring liver reserve capacity is crucial for determining the timing of transplantation surgery. Quantitative liver function tests can assess the liver function status at a specific time for a given patient, such as the 14C-aminopyrine breath test, galactose clearance test, caffeine-MEG-X test, and indocyanine green test; if various tests are combined or performed in series, they are even more valuable. However, these tests are often time-consuming, expensive, and some believe they may not necessarily provide more value than traditional Child-Pugh classification. Therefore, they are currently limited to certain research centers.
4. Diagnosing specific liver diseases
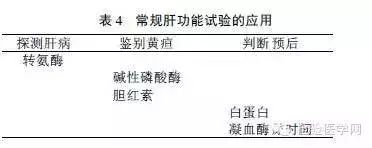
Testing various disease markers is mainly used; for viral hepatitis, corresponding antigens, antibodies, and viral genes can be tested; for hepatocellular carcinoma, serum alpha-fetoprotein can be tested; and for primary biliary cirrhosis, mitochondrial antibodies can be tested (see Table 1). In daily work, it is neither possible nor necessary to test all of these various liver function tests for every patient. To achieve the purposes of detecting liver disease, differentiating jaundice, and assessing prognosis, serum transaminases, alkaline phosphatase, bilirubin, and prothrombin time are generally used as routine tests (see Table 4), which often show relatively characteristic changes in common liver diseases. Based on this, additional tests can be added as clinically needed.
5. Limitations of the tests
Although liver function tests are indispensable in the management of liver disease, they have many limitations, reflected in:
① Sensitivity is not high. In some severe liver diseases such as cirrhosis and hepatocellular carcinoma, test results can be normal;
② Some tests do not necessarily have specificity for liver function abnormalities; for example, decreased serum albumin can also be seen in inflammatory bowel disease, and elevated transaminase activity can also be seen in skeletal muscle and myocardial diseases;
③ Most tests cannot specifically diagnose a particular liver disease; for example, they cannot differentiate between intrahepatic and extrahepatic cholestasis, nor can they differentiate between viral hepatitis and drug-induced hepatitis;
④ No single test can accurately assess all liver functions. The liver has hundreds of biochemical functions, and tests can only reflect limited functions. Some tests, such as transaminases, only reflect liver cell damage and do not help in assessing liver function. Therefore, in clinical practice, different liver function tests should be used in conjunction with clinical test results for comprehensive analysis and judgment.

● The most complete expression pack for the laboratory department, so real!
● Reference values and clinical significance of cerebrospinal fluid tests
● How to handle cold agglutination specimens in blood routine
● What is EDTA-dependent pseudothrombocytopenia?