
Source: “Chinese Journal of Osteoporosis and Bone Mineral Disorders”, Volume 17, Issue 5, September 2024
Corresponding Author: Ding YueOsteoporosis (OP) is a common systemic bone disease with a high prevalence among the elderly population. As the global population ages, the impact of OP and the fragility fractures it causes is becoming increasingly severe for individuals and society. However, effective early screening methods are still lacking. Bone turnover markers (BTMs) are a series of metabolic products generated during the bone remodeling process, which have high sensitivity and can reflect changes in bone tissue, making them useful for assisting in OP screening. However, there are many types of BTMs, with various sources, and there is currently no unified detection standard. In recent years, with advancements in detection technology and deeper research, scholars have reported some new markers with promising application prospects. This article provides a review of the research progress of BTMs in the early screening of OP.
Osteoporosis is characterized by a decrease in bone mass and destruction of bone microstructure, leading to increased bone fragility and a higher likelihood of fractures. OP has become one of the common chronic diseases that severely threaten the health of the elderly population. Epidemiological surveys in China show that the prevalence of OP among people over 50 and 65 years old is 19.2% and 32.0%, respectively, with a total affected population of approximately 90 million[1]. Osteoporotic fractures (OF) are one of the most serious complications of OP, often affecting the hip and spine. Data indicates that the short-term mortality rate after hip fractures reaches 17% to 28%[2].
Most OP patients do not exhibit obvious clinical symptoms in the early stages of the disease and are diagnosed only when the disease has progressed to a later stage. Therefore, early screening and diagnosis of OP are extremely important. Currently, the recommended screening methods for OP in China primarily include the International Osteoporosis Foundation (IOF) one-minute osteoporosis risk test, the Osteoporosis Self-Assessment Tool for Asians (OSTA), and quantitative ultrasound (QUS) for measuring bone density. However, the one-minute osteoporosis risk test is easily influenced by individual subjective judgment, OSTA is only applicable to postmenopausal women, and QUS cannot meet screening requirements due to its poor diagnostic efficacy. Therefore, there is an urgent need to develop more universal, convenient, and efficient early screening methods for OP to improve the feasibility and accuracy of screening.
Since the 1980s, alkaline phosphatase (ALP) has been proposed as an indicator reflecting the degree of bone loss in postmenopausal women[3]. As research deepened, more bone turnover markers (BTMs) such as osteocalcin (OC) and pyridinoline (PYR) began to be used to assess the risk of OP in postmenopausal women by the late 1990s. Entering the 21st century, the IOF and the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) began to promote the standardization and unification of BTMs. China also updated the “Guidelines for the Application of Bone Turnover Markers” in 2021[4], further standardizing the clinical application of traditional BTMs.
In recent years, with advancements in detection technology and deeper research, scholars have reported some new markers with good application prospects. Currently, BTMs have become one of the auxiliary detection indicators in clinical practice, capable of sensitively reflecting changes in bone mass and predicting fracture risk independently of bone density. However, a unified standard has not yet been established. Therefore, this article aims to review the application progress of BTMs in OP screening to provide assistance for future clinical practice and research directions.

Bone Remodeling and OP
Bone remodeling refers to the process of replacing old bone with new bone through bone resorption and bone formation, maintaining the integrity and stability of the skeleton to meet functional needs. In the bone resorption phase, osteoclasts degrade the collagen and inorganic salts in the bone matrix by secreting acids and various enzymes, releasing minerals such as calcium. Subsequently, in the bone formation phase, mesenchymal stem cells differentiate into osteoblasts, secrete osteoid, and promote its mineralization, ultimately resulting in new bone formation. BTMs are metabolic products produced during this process[5], which can be classified into bone formation markers and bone resorption markers. They can sensitively reflect the metabolic state of bone tissue and can be repeatedly measured. In normal physiological conditions in adults, bone resorption and bone formation are coupled, maintaining bone mass stability through dynamic balance.
In the occurrence of OP, an imbalance in bone remodeling is a key feature. This imbalance is primarily manifested as a negative balance between bone formation and bone resorption, where bone resorption exceeds bone formation, leading to a gradual decrease in bone mass. In addition, the mineralization process of the bone matrix is also impaired, further weakening the strength of the skeleton, making it more fragile and prone to fractures. Therefore, monitoring BTMs to assess the state of bone remodeling is crucial for the early screening of OP.
Traditional BTMs
Bone Resorption Markers
Traditional bone resorption markers mainly include C-terminal telopeptide of type I collagen (CTX), N-terminal telopeptide of type I collagen (NTX), PYR, deoxypyridinoline (DPD), and tartrate-resistant acid phosphatase 5b (TRACP 5b). CTX, NTX, PYR, and DPD are components of collagen and are released into the bloodstream under the action of various enzymes secreted by osteoclasts, while TRACP 5b is an enzyme secreted by osteoclasts that assists in the degradation of bone matrix.
These markers are recommended in Chinese guidelines as representative markers reflecting the bone resorption process[4], with CTX being the most commonly used. Recent studies indicate that serum β-CTX levels are positively correlated with the incidence of OP among the elderly population in China[6]. PYR and DPD mainly exist in bone tissue, so their measurement has high specificity and is less influenced by other tissues, but their determination requires the collection of 24-hour urine samples and correction with urine creatinine, which places high demands on patient compliance.
Bone Formation Markers
Traditional bone formation markers mainly include procollagen type I N-peptide (P1NP), procollagen type I C-peptide (P1CP), ALP, bone alkaline phosphatase (b-ALP), and OC. Among them, P1NP and P1CP are products generated from the hydrolysis of procollagen type I during the bone formation process. ALP is widely distributed in various tissues, including bone tissue, while b-ALP is primarily secreted by osteoblasts. OC, as the most abundant non-collagen protein in bone, is mainly secreted by osteoblasts.
These markers are recommended in Chinese guidelines as representative markers reflecting the bone formation process[4], with P1NP being the most commonly used. Since P1NP is less affected by food intake and circadian rhythms[7], its measurement is not time-restricted, making it convenient for outpatient testing. Compared to ALP, b-ALP can more accurately reflect the bone formation process, but its measurement accuracy is still influenced by other isoenzymes. Although OC is considered by some researchers to be the most sensitive indicator of bone formation status[8], its short half-life and easily degradable carboxyl-terminal fragments may limit its widespread clinical application[9].
Potential BTMs
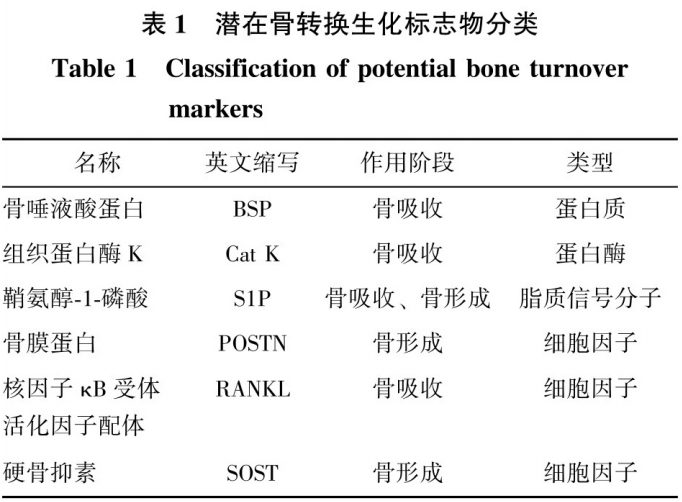
In recent years, some emerging biomarkers have shown promise as potential BTMs. These potential BTMs include bone sialoprotein (BSP), cathepsin K (Cat K), sphingosine-1-phosphate (S1P), receptor activator of NF-κB ligand (RANKL), periostin (POSTN), and sclerostin (SOST). Based on their molecular biological functions, these markers can be categorized into different classes such as proteins, proteases, cytokines, and lipid signaling molecules (Table 1).
 Protein Class
Protein Class
BSP is a highly glycosylated and phosphorylated non-collagen protein, primarily secreted by osteoblasts and osteoclasts. BSP promotes the adhesion of peripheral osteoclasts to the bone surface[10], facilitating bone resorption. Clinically, serum BSP levels are quantitatively analyzed using ELISA to assess osteoclast activity and the degree of bone resorption. Fassbender et al.[11] pointed out that in female populations, serum BSP expression levels are negatively correlated with the bone density of the lumbar spine and femoral neck. Hasan et al.[12] found that in postmenopausal women, serum BSP levels in OP patients were significantly higher than in healthy women and positively correlated with various BTMs levels. These studies suggest that BSP has the potential to become one of the indicators for OP screening. However, more clinical data is needed to confirm its validity as a screening indicator.
Protease Class
Cat K is a cysteine protease primarily secreted by osteoclasts. Cat K can cooperate with other proteases to degrade type I collagen in the bone matrix[13] and may serve as a potential indicator reflecting the quantity and function of osteoclasts and evaluating the bone resorption process.
Studies have shown that serum Cat K expression levels may help distinguish postmenopausal OP women from healthy women[14-15] and predict the risk of OF. Meanwhile, Munoz-Torres et al.[16] found that serum Cat K expression levels decreased with OP treatment in postmenopausal women. However, Gao et al.[17] analyzed 1752 postmenopausal women in China and reached the opposite conclusion, suggesting that serum Cat K expression levels were unrelated to bone density and did not significantly correlate with other BTMs. This indicates that Cat K may not be suitable for OP screening in the Chinese population. However, Gao et al. did not conduct a statistical comparison of Cat K expression levels between OP patients and healthy women, so the effectiveness of Cat K for OP screening still requires extensive further validation.
Additionally, the low circulation level of Cat K and its potential hydrolysis by other enzymes such as cathepsin S may also limit its reliability in clinical applications. Future research should focus on improving the sensitivity of detection technology to fully utilize Cat K’s potential in OP screening.
Lipid Signaling Molecule Class
S1P is a bioactive lysophospholipid secreted by osteoblasts and osteoclasts, which can influence osteoblast differentiation to promote bone formation and regulate osteoclast generation to promote bone resorption[18]. S1P also acts as a coupling factor between bone formation and resorption, maintaining bone metabolic balance. As osteoclasts mature, the secretion of S1P gradually increases, subsequently binding to sphingosine-1-phosphate receptor-3 (S1PR3) on osteoblasts, promoting their maturation and OC secretion.
After binding to the receptor on the surface of osteoclasts, OC downregulates S1P transport protein synthesis and subsequently inhibits S1P secretion[19], while also binding to sphingosine-1-phosphate receptor-2 (S1PR2) on osteoblasts, promoting the release of osteoprotegerin (OPG), which competitively binds to RANK receptors on osteoclasts, negatively regulating the number of osteoclasts[20]. An imbalance in this coupling process will promote the occurrence of OP; therefore, S1P has the potential to be used as a marker for OP screening.
Lee et al.[21] found that plasma S1P expression levels were negatively correlated with bone density and positively correlated with the expression levels of bone resorption markers. Additionally, multiple studies have indicated that plasma S1P expression levels are positively correlated with the incidence of OF[22-23]. Kim et al.[24] also pointed out that the ratio of S1P levels in plasma to bone marrow can serve as a predictive indicator for OF occurrence. However, Weske et al.[25] found the opposite conclusion, suggesting that S1P expression levels were positively correlated with bone formation markers.
The discrepancies in these different studies may stem from the complex role of S1P in bone metabolism. On one hand, S1P may primarily promote OP and OF development by enhancing bone resorption; on the other hand, when bone density decreases, S1P may act as a protective factor by promoting bone formation more actively to counteract bone loss. Therefore, the role of S1P in bone metabolism may depend on different physiological or pathological conditions, necessitating further research to clarify its specific mechanisms in disease progression. Additionally, the accuracy of S1P measurement is influenced by lipid metabolism and the secretion of S1P from red blood cells and other cells[26]. Consequently, clinical applications should consider whether patients have conditions such as obesity or anemia that may affect S1P expression levels.
Cytokine Class
POSTN:Also known as osteoblast-specific factor-2 (OSF-2), is a bone matrix protein primarily secreted by osteoblasts. In the process of bone metabolism, POSTN promotes bone formation by binding to osteoblast surface integrins αvβ3 and αvβ5, regulating signaling pathways such as Wnt/β-catenin, NF-κB/STAT3, and PI3K/AKT[27], thus its expression level can reflect osteoblast activity and the bone formation process.
In terms of predicting OF, Kim et al.[28] proposed that serum POSTN expression levels could better reflect changes in cortical bone, indicating a higher accuracy for predicting femoral OF occurrence compared to spinal OF. Prospective studies by Rousseau et al.[29] found that total serum POSTN expression levels could serve as an indicator for predicting the risk of OF occurrence, while Bonnet et al.[30] suggested that the expression levels of K-POSTN fragments in serum could more accurately predict OF occurrence.Although the correlation between POSTN and OF occurrence has been confirmed by multiple studies, there is currently no clear data indicating that POSTN can predict the occurrence of OP.Li et al.[31] reported that total serum POSTN expression levels among postmenopausal women in China showed no correlation with bone mass or bone density, nor with the levels of traditional BTMs[30-31].This suggests that POSTN may not be suitable for OP screening in the Chinese population.
Given the limited sample size of current studies, future research needs to expand the sample size and conduct prospective studies to further explore the utility of POSTN in OP screening, including assessing the correlation between changes in POSTN expression levels over time and bone density. Furthermore, research should investigate whether the combined use of POSTN and BTMs can predict the occurrence of OP.
Currently, the measurement of POSTN expression levels is relatively simple and can be detected using kits, making it convenient for community medical applications and aiding in early OP screening. However, since POSTN is expressed in multiple tissues, the accuracy of its measurement is affected, leading to deviations in the results. Therefore, future research needs to carefully consider how to accurately interpret changes in POSTN levels and explore possible strategies to distinguish variations in POSTN levels caused by skeletal and non-skeletal factors.
SOST:A glycoprotein secreted by mature osteocytes, which can bind to low-density lipoprotein receptor-related protein 4 (LRP4) and 5/6, thereby inhibiting the Wnt/β-catenin signaling pathway[32], subsequently inhibiting bone formation and stimulating bone resorption. Currently, there is some controversy regarding the relationship between SOST and bone density. Some studies have found that serum SOST levels in postmenopausal women are positively correlated with bone density[33-34], while others have indicated a negative correlation[35]. A prospective study found that although SOST is positively correlated with bone density, high serum SOST expression levels are also associated with a high risk of OF[36].
The differences in the above studies may partially explain that higher bone density means a larger number of bone cells, leading to more SOST secretion[35]. Additionally, bone loss in postmenopausal women may primarily be due to local mechanical stress stimulating osteocytes to secrete SOST, while an imbalance in feedback regulation of SOST levels will lead to OP and OF occurrence[36]. Therefore, SOST, as a potential BTM, has significant research prospects in the field of OP screening, and future studies need to further explore the role of SOST in bone metabolism in OP patients and assess its application potential in OP screening.
Currently, SOST measurement primarily uses ELISA and electrochemiluminescence methods. Studies have shown that although these two methods exhibit high correlation, significant differences in measurement results may occur due to structural similarities between SOST fragments and other protein fragments[37]. Therefore, in clinical applications, it is essential to consider the differences in results that may arise from different detection methods. Research indicates that SOST expression levels are not affected by blood collection time[38] and remain stable during the menstrual cycle[39], providing convenience for early OP screening.
RANKL:A member of the tumor necrosis factor superfamily, exists in two forms: membrane-bound (mRANKL) and soluble (sRANKL), primarily expressed by osteocytes and osteoblasts. RANKL promotes the activation of osteoclasts by binding to the RANK receptor on their surface, making it an important indicator reflecting the bone resorption process. Although clinical trials have proven that monoclonal antibodies against RANKL, such as denosumab, have good efficacy in treating OP[40], the exact correlation between RANKL and OP remains a controversial topic.
Some studies have indicated that RANKL expression levels are not significantly correlated with bone density in postmenopausal women[41-42]. However, research by Stern et al.[43] showed that while serum RANKL levels are not related to bone density in postmenopausal women, they have a statistically significant correlation with bone density in elderly men. This finding suggests that RANKL may be more suitable as a biomarker for OP screening in men. Furthermore, the ratio of RANKL to OPG is believed to more comprehensively reflect changes in bone metabolism than RANKL alone. Many studies have demonstrated that the RANKL/OPG ratio can reflect changes in bone density[44-45]. The discrepancies in the above studies may be influenced by factors such as different sample preservation conditions and detection methods.
Thus, the gender-specific effects of RANKL and the effectiveness of the RANKL/OPG ratio in OP screening still require more basic and clinical research for further validation. Although RANKL measurement is not affected by circadian rhythms[46], its expression levels in circulation are low, and the lack of highly sensitive detection technology limits the accurate measurement of RANKL. Future research should focus on developing more sensitive detection methods to provide stronger evidence for the application of RANKL in OP screening.
Limitations of BTMs in OP Screening
BTMs have high sensitivity in monitoring bone metabolic status and are mainly used for determining OP bone turnover types and evaluating anti-osteoporosis drug treatment. However, clinical validation is still needed for screening or diagnosis. Although they show potential for early screening of OP, factors such as a lack of clinical data, significant individual differences, and difficulties in standardization limit the application of BTMs as OP screening indicators in clinical practice.
Lack of Clinical Data
1. The limitations of research populations lead to a concentration of studies on BTMs in specific groups, such as postmenopausal women or patients with certain diseases, while related research on healthy middle-aged women, premenopausal women, and men is relatively lacking, limiting the application value of BTMs in broader populations.
2. Most studies are single cross-sectional studies, lacking prospective studies that can assess the long-term stability and predictive value of BTMs.
3. Insufficient research on the sensitivity and accuracy of BTMs in OP screening limits the understanding of their clinical utility.
4. Most studies have insufficient sample sizes, affecting the generalizability and reliability of the results.
Therefore, future research needs to adopt multi-center, large-scale sample designs to provide richer data, which is crucial for establishing unified reference intervals and detection methods for BTMs. These efforts will help comprehensively assess the practical application potential of BTMs in OP screening and promote their widespread application in clinical settings.
Significant Individual Differences
The individual variability of BTMs is influenced by various controllable and uncontrollable factors. Controllable factors include circadian rhythms, dietary habits, menstrual cycles, seasonal changes, etc. Uncontrollable factors involve individual age, sex, pregnancy status, immobilization, and related diseases affecting BTM expression levels. Specific content can be summarized in Table 2.
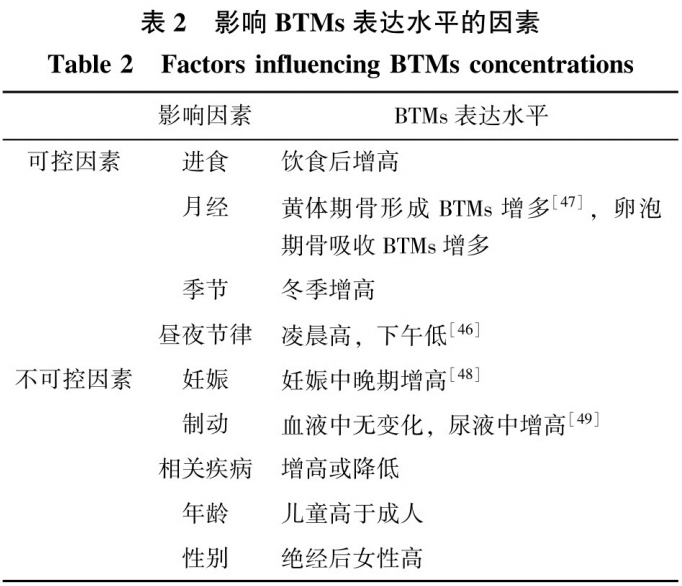
The individual variability of BTMs is also affected by other factors such as ethnicity and medication use. Therefore, when establishing reference intervals for BTMs and using them for screening or efficacy assessment in clinical practice, individual assessments of patients should be conducted.
Difficulties in Standardization
Although some immunoassay methods for BTMs have been automated, significant differences still exist in accuracy and standardization between different testing institutions and methods. A study in Europe tested serum and urine BTM samples from 73 laboratories, revealing that even when using the same testing method, most BTM measurement results showed significant discrepancies[50]. Additionally, some BTMs, such as TRACP 5b and OC, due to their structural instability, have strict requirements for sample preservation and transportation conditions, and improper sample handling can further affect the accuracy of detection. Therefore, achieving calibration of reference values and standardization among laboratories remains a problem to be solved.
Future Research Directions
Bone Density Combined with BTMs
Bone density, as the “gold standard” for OP diagnosis, can directly reflect skeletal strength; BTMs can provide information about the dynamics of bone metabolism. Therefore, combined detection of both is expected to more comprehensively assess bone status, thereby improving the accuracy of OP screening. The OFELY study, through prospective observation of 671 postmenopausal women, revealed that women with both low bone density and high BTM levels had a higher risk of OF within 10 years[51]. This finding is supported by a retrospective study by Qu et al.[52], which indicated that older women with high serum β-CTX levels and low bone density were more likely to experience OF.
In addition, Chinese guidelines also indicate that the combined detection of bone density and BTMs can improve the predictive efficacy for fragility fractures[4]. By combining these two measurement methods, more precise screening scales and judgment standards can be developed, which may achieve early screening for OP. However, the current bone density detection equipment is large and expensive, making it unsuitable for OP screening. There is still a need to develop more portable and highly accurate bone density detection devices. The screening methods combining bone density and BTMs still require more prospective clinical studies to validate their reliability and practical application effectiveness.
AI-Assisted Screening
The rapid development of artificial intelligence (AI), especially in the field of machine learning, has significantly enhanced the ability to extract meaningful information from complex BTM datasets. Advanced algorithms in AI can identify and analyze patterns and associations within large BTM datasets, simplifying the complexity of the data and improving the depth and accuracy of comprehensive analyses of OP biomarkers.
Zhang et al.[53] analyzed data from 9053 postmenopausal OP patients using support vector machines (SVM) and found that a single BTM could not determine whether an individual had OP, but as the number of BTMs in the model increased, the accuracy of OP determination improved. When six types of BTMs were used together, this judgment method achieved a kappa coefficient of 0.9876 compared to DXA diagnostic methods. Wang et al.[54] similarly used SVM to construct a learning model to determine OP in type 2 diabetes patients, achieving an accuracy rate of 88% by combining gender, age, body mass index, P1NP, and OC. Wang et al.[55] used a random forest model to select BTMs for determining whether postmenopausal women had OP, while also constructing a model with high accuracy for OP determination by combining BTMs with biochemical metabolites, achieving an area under the ROC curve of 0.828.
Although AI shows great potential in BTM data analysis, there are some limitations in current research and applications.
1. AI models rely on large amounts of high-quality data for training, but currently available data is limited[53-54] and may have selection bias, affecting the generalizability and clinical applicability of the models.
2. The performance of biomarkers may vary across different populations, and current AI models have not adequately considered the influence of factors such as ethnicity, region, and genetics.
3. Although studies have shown that AI models have high accuracy, their application in actual clinical settings remains limited, partly due to high hardware and software requirements and the need for AI technology professionals.
Future research directions should focus on addressing these limitations to improve the accuracy and efficiency of screening. Fully utilizing AI’s capabilities in BTM data analysis through its powerful data integration and feature extraction capabilities is expected to enhance screening efficiency.
Innovations in Detection Methods
Test Strips:Test strip technology is rapidly developing in the application of BTMs detection. Lee et al.[56] utilized lateral flow immunochromatography to develop test strips for detecting urine NTX and serum CTX, with measurement results highly correlated with the “gold standard” ELISA. However, the low concentration of BTMs in test samples requires further research on the correlation of measurement results with ELISA for high concentration samples. Chen et al.[57] designed a test strip to measure P1NP using gold nanoparticles, which showed good correlation with the Roche method and had a detectable minimum concentration of 10 ng/mL, expanding the detection range and providing new possibilities for low concentration BTM detection.
BTM detection test strips stand out due to their rapid and easy operation. These strips can provide immediate qualitative or semi-quantitative results, which can be transformed into quantitative data through advanced software technology, greatly facilitating statistical analysis and clinical decision-making. However, the accuracy of test strip measurements may be affected by environmental factors such as temperature and humidity, necessitating consideration of these factors in design and usage. There is a need to develop test strips capable of detecting more types of BTMs, combined with advanced nanotechnology to improve the sensitivity and specificity of the strips, and to encourage close collaboration between research institutions and industry to promote the research and marketization of convenient and practical BTM measurement test strips.
Chips:Chip technology provides an efficient alternative for BTM detection. Static protein chips and microfluidic chips allow for simultaneous detection of multiple BTMs, significantly improving detection efficiency. Claudon et al.[58] simultaneously detected CTX, P1NP, and OC in serum, with measurement results highly correlated with ELISA. Future exploration of the minimum detection concentrations for each BTM and the development of kits to enhance BTM detection efficiency is warranted. Protein microfluidic chip technology manipulates fluids at the micron scale on chips to detect protein content, offering high efficiency and sensitivity, which has great potential in BTM detection. Research by Carmona et al.[59] successfully measured the binding coefficient of OC with microchannel surfaces modified on chips, highlighting the application potential of microfluidic chips in BTM detection. Although this research demonstrates a new method for enhancing OC detection sensitivity, this technology has not yet been applied in actual OC content measurement.
Microfluidic chips possess advantages such as automation, low sample reagent requirements, and high detection efficiency, but their high production costs and the need for optimization in result integration and analysis limit their widespread clinical adoption. Future efforts should focus on reducing the manufacturing costs of chips, enhancing the detection capabilities for multiple target BTMs, and integrating AI technology to improve data processing intelligence, promoting the popularization of microfluidic chip detection technology and making it an efficient and accurate tool for OP screening.
Biological Sensors:Biological sensors are detection tools that convert the concentration of biological substances into electrical signals, offering non-invasive, highly specific, and repeatable measurements. Optical and electrochemical biological sensors are particularly prominent in BTM detection. Chinnappan et al.[60] developed an optical biosensor using graphene oxide, successfully detecting serum OC concentrations with a low detection limit. The electrochemical biosensor designed by Yun et al.[61] demonstrated a wide dynamic range and low detection limit for CTX using electrochemical impedance spectroscopy (EIS) technology. Similarly, the electrochemical biosensor based on nanopore arrays designed by Lee et al.[62] exhibited high sensitivity in detecting ALP, also based on EIS principles. Besides the widely used optical and electrochemical biosensors, Liu et al.[63] designed a photothermal biosensor that quantitatively and qualitatively detects ALP through temperature changes, offering portability and sensitivity, providing a new avenue for rapid BTM detection.
Although biological sensors provide advantages of high sensitivity and wide detection ranges in biomarker detection, they still face some challenges. Electrochemical biosensors may suffer from insufficient interference resistance, while the signal transmission efficiency of optical biosensors is affected by environmental temperature and humidity. Currently, most biological sensor designs are limited to detecting a single BTM, restricting their application scope in OP screening. With continuous advancements in nanotechnology, the application of nanomaterials in biological sensors to enhance their performance will become an important development direction in the future, such as Chang et al.[64], who have utilized gold nanoparticles to modify electrochemical sensor electrodes to improve the minimum detection concentration of OC. Additionally, new biological sensors capable of simultaneously detecting multiple BTMs are urgently needed for design and application.
Test strips, chips, and biological sensors have shown great application prospects in basic research and have the potential to improve the accuracy of OP screening. However, these technologies are still in their initial stages of development and face challenges such as high costs, technical demands, and difficulties in application promotion. The advancement of technology requires the impetus of clinical pain points and needs, but it must also consider cost, benefits, and the translation of research results. Developing low-cost, portable, and highly accurate devices to move from the “laboratory” to the “shelf” is essential for benefiting the general public.
Conclusion
BTMs, as sensitive indicators reflecting the state of bone remodeling, show vast application prospects in OP screening. Traditional BTMs have been used to determine the bone turnover type of OP, but a unified detection standard has not yet been established. New markers including BSP, Cat K, S1P, etc., provide a more comprehensive view of bone metabolism but still require large-scale research to verify their effectiveness and accuracy in OP screening. Future research will focus on improving the precision and convenience of BTM detection and actively addressing the issues in the translation process from research to clinical application, enabling various detection devices to enter clinical practice and achieve the goal of OP screening for the general population.
References


↑Swipe up to read the full article↑
Corresponding Author Profile

Ding Yue
Director of the Department of Orthopedics, Sun Yat-sen Memorial Hospital of Sun Yat-sen University, Doctor of Medicine, Professor, Chief Physician, Doctoral Supervisor, Secretary of the Party Branch of Orthopedic Staff, Director of the Medical Engineering Integration Research Center.
Serving as an executive committee member of the Osteoporosis and Bone Mineral Disorders Branch of the Chinese Medical Association, deputy leader of the Basic Research and Innovation Transformation Professional Group of the Sports Medicine Physician Branch of the Chinese Physician Association, member of the Basic Group of the Orthopedic Physician Branch of the Chinese Physician Association, member of the Basic Group of the Orthopedic Society of the Chinese Medical Association, and the incoming chairman of the Osteoporosis Branch of the Guangdong Medical Association.
Responsible for 7 national natural science foundation projects and over 10 provincial and university research projects, published more than 100 papers in domestic and international professional journals, and has 5 authorized patents. Received the second and third prizes for scientific and technological progress in Guangdong Province, and the second prize for scientific and technological progress in Guangzhou City. Awarded the title of Outstanding Young Medical Talent in Guangdong Province and “March 8 Red Flag Bearer”.
Related Reading
● Ding Yue: Comprehensive Analysis of the Current Status and Response Strategies for Osteoporosis Treatment
Disclaimer: The content and images of this article are provided by the contributing unit for learning and exchange purposes only and do not represent the views of Orthopedic Online.




↓↓↓Click 【Read Original】 for more content