*For reference by medical professionals only
ADC drugs reshape the stratified treatment strategy for HR+ advanced breast cancer
In recent years, the rapid development of antibody-drug conjugates (ADC) has brought groundbreaking progress to the treatment of advanced breast cancer.Trastuzumab deruxtecan (T-DXd) and datopotamab deruxtecan (Dato-DXd) are representative drugs that are profoundly changing the treatment landscape for HR+ advanced breast cancer. The DESTINY-Breast06 (DB06) study explored the benefits of T-DXd in earlier lines of treatment for HR+/HER2 low-expressing and HER2 ultra-low-expressing populations, providing new treatment options for those who have previously received ≥1 line of endocrine therapy (ET) in the HR+/HER2 low-expressing and HER2 ultra-low-expressing populations, leading to unprecedented survival improvements for those who could not continue endocrine treatment after CDK4/6 inhibitor therapy ± targeted therapy (ET±TT). Meanwhile, Dato-DXd, based on the TROPION-Breast01 (TB01) study, has demonstrated exceptional therapeutic potential in patients with treated HR+/HER2- advanced breast cancer, becoming an important representative of TROP 2-targeted ADC drugs.
On August 12, 2025, the official ESMO journal, Annals of Oncology, published an online update of the “ESMO Guidelines for Systemic Treatment Recommendations for Advanced Breast Cancer”[1]. This guideline update actively responds to the aforementioned advancements: for the first time, HER2 ultra-low expression has been included in precision stratification recommendations, further improving the stratified treatment model for breast cancer, and recommending T-DXd for the treatment of HER2 ultra-low expressing population; at the same time, for the first time, Dato-DXd has been included in the treatment pathway for HR+ populations, further enriching the subsequent medication options for HR+/HER2- metastatic breast cancer (MBC) patients. On this occasion, the oncology channel of the medical community specially invited Professor Yang Qingmo from the First Affiliated Hospital of Xiamen University, to deeply interpret the research data and clinical status of T-DXd and Dato-DXd in conjunction with the latest recommendations from the ESMO guidelines.
T-DXd is recommended as the preferred option for MBC patients who are not suitable for ET± TT and have not received chemotherapy HR+/HER2 low-expressing or ultra-low-expressing MBC. The new ESMO guidelines use “sensitivity to endocrine therapy” as an important stratification basis, reconstructing the treatment pathway for HR+/HER2- MBC, clearly stating: for patients with disease progression who are not suitable for ET±TT, if they have not previously received chemotherapy, it is recommended that HER2 low-expressing or ultra-low-expressing patients use T-DXd for treatment[I, A; MCBS 3].
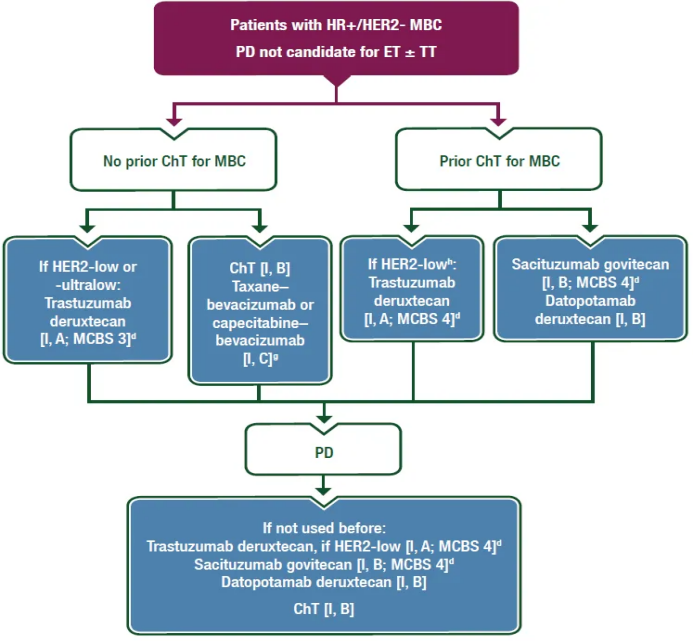
Figure 1. Management plan for HR+/HER2- MBC patients after disease progression who are not suitable for ET±TT
The update of the ESMO guidelines regarding T-DXd is mainly based on the groundbreaking results of the DB06 study[2]. In terms of the characteristics of the enrolled population, the DB06 study included patients who progressed within 6 months of first-line CDK4/6 inhibitor + ET, or relapsed within 24 months of starting adjuvant ET, or had received ≥2 lines of ET treatment, and had not previously received chemotherapy for advanced disease. Among them, over 89% of patients received CDK4/6 inhibitor + ET treatment during the metastatic disease stage. Compared to the DB04 study (patients who received 1-2 lines of chemotherapy for advanced disease), the DB06 study enrolled patients who were more frontline; and also included HER2 low-expressing and HER2 ultra-low-expressing patients, covering a broader population. The latest results published in the New England Journal of Medicine (NEJM) show that compared to chemotherapy, T-DXd significantly improved the median progression-free survival (mPFS) of HER2 low-expressing populations (13.2 months vs 8.1 months; HR=0.62; P<0.001). In the HER2 ultra-low-expressing population, T-DXd also showed PFS improvement compared to chemotherapy (13.2 months vs 8.3 months; HR=0.78), with a nearly consistent trend of benefit between the two groups. Furthermore, an interaction test was conducted at the suggestion of the NEJM review committee, showing no significant interaction between the treatment benefits of T-DXd and different populations. This further indicates that both HER2 ultra-low-expressing and HER2 low-expressing populations can benefit from T-DXd treatment.
In addition, exploratory biomarker analysis data from the DB06 study presented at this year’s American Society of Clinical Oncology (ASCO) annual meeting (abstract number: 1013) indicate that regardless of the presence of key gene mutations such as PI3K/AKT pathway, ESR1, or BRCA1/2, T-DXd shows a consistent trend of benefit compared to chemotherapy across the total population, suggesting that T-DXd has the potential to overcome common resistance mechanisms and provide effective treatment options for the genomic heterogeneity of HR+/HER2 low-expressing and ultra-low-expressing patients.
Overall, the results of the DB06 study profoundly impact international clinical practice—the ESMO guidelines have been updated to clearly recommend T-DXd as the preferred treatment option for HR+/HER2 low-expressing or ultra-low-expressing MBC patients who are not suitable for ET±TT and have not received chemotherapy.
In the future clinical practice for HR+ MBC, it may be possible to apply T-DXd to eligible patients without waiting for genetic testing results, thus bringing greater survival improvements. On January 27, 2025, T-DXd was approved by the U.S. Food and Drug Administration (FDA) for the treatment of unresectable, HR+/HER2 low-expressing or ultra-low-expressing breast cancer patients, becoming the first ADC drug approved for the treatment of HER2 ultra-low expression. This marks another expansion of T-DXd’s boundaries in anti-HER2 treatment, extending its benefit population from HER2 low-expressing to HER2 ultra-low-expressing. Furthermore, T-DXd has been included in the national medical insurance catalog in China, greatly improving drug accessibility and reducing the economic burden on patients, allowing more patients to benefit from this efficient and precise treatment plan.
Dato-DXd is recommended as the preferred option for MBC patients who are not suitable for ET±targeted therapy and have received chemotherapy
In addition, the guidelines recommend that for MBC patients with disease progression who are not suitable for ET±TT, if they have previously received chemotherapy, it is recommended to use Dato-DXd [I, B] . This is the first time that the ESMO guidelines have included Dato-DXd in treatment recommendations, highlighting its important position in the treatment of HR+/HER2- MBC.
The update of the ESMO guidelines regarding Dato-DXd is mainly based on the groundbreaking results of the TB01 study. This study included 732 HR+/HER2- advanced breast cancer patients who had received 1-2 lines of chemotherapy (of which over 80% were treated with CDK4/6i), randomly receiving Dato-DXd or investigator’s choice of chemotherapy (ICC). The results have been disclosed multiple times at international oncology conferences and published in full in the Journal of Clinical Oncology (JCO).[4,5] The primary study endpoint showed that compared to the ICC group, the Dato-DXd group had a significant improvement in PFS (6.9 vs 4.9 months; HR=0.63); at a median follow-up of 22.8 months, the overall survival (OS) between the two groups did not reach statistical significance (HR=1.01; 95% CI 0.83–1.22). This may be due to the approval of multiple new ADC drugs during the trial, with some subjects receiving these drug treatments after disease progression or treatment discontinuation, thus interfering with the OS results. Specifically, the treatment rates of subsequent ADC drugs in the Dato-DXd group and ICC group were 12% and 24%, respectively; this crossover treatment situation, especially the higher proportion of ADC drug use in the ICC group, may have weakened the OS difference. Therefore, the researchers conducted an OS sensitivity analysis, and after correction, the OS for the Dato-DXd group and ICC group were 19.1 months and 17.5 months (HR=0.86; 95% CI 0.70‒1.06). In terms of safety, the incidence of grade ≥3 treatment-related adverse events (TRAEs) in the Dato-DXd group was 21%, less than half of that in the ICC group (45%); among them, the incidence of grade ≥3 neutropenia was only 1%, reduced by about 30 times compared to the ICC group (31%), further confirming the efficacy and safety advantages of Dato-DXd.
Not only that, at the 2024 ESMO Asia conference, data from the TB01 study’s Chinese cohort were presented (abstract number: 38MO), which included 83 Chinese patients.[6] Among them, the Dato-DXd group had 44 cases, and the ICC group had 39 cases. The results showed that the mPFS of the Dato-DXd group reached 8.1 months, nearly twice that of the ICC group (8.1 vs 4.2 months; HR=0.54). In terms of objective response rate (ORR), the Dato-DXd group improved by 20.7% compared to the ICC group (38.6% vs 17.9%). Safety data were consistent with global patients, with the incidence of grade ≥3 TRAEs being 27.3%, far lower than that of the ICC group (27.3% vs 55.6%), and no Chinese patients discontinued treatment due to Dato-DXd, providing important data support for the application of Dato-DXd in chemotherapy-treated HR+/HER2- breast cancer patients in China.
Based on the TB01 study, Dato-DXd has been successively approved in Japan, the United States, and the European Union in December 2024, January 2025, and April 2025 for the treatment of unresectable or metastatic HR+/HER2- (IHC 0, IHC 1+, or IHC 2+/ISH-) breast cancer adult patients who have previously received endocrine therapy and at least one line of chemotherapy in the advanced disease stage, and was approved by the National Medical Products Administration (NMPA) in China on August 22, 2025.[7-10] In summary, Dato-DXd provides a new treatment option superior to traditional chemotherapy for HR+/HER2- MBC patients who have been treated with chemotherapy but are not suitable for continuing ET±TT, and it is expected that Dato-DXd will bring more treatment benefits to breast cancer patients in China in the future.
In conclusion, the update of the 2025 ESMO online guidelines for metastatic breast cancer promotes a transformation in the treatment model for HR+/HER2- MBC, further clarifying the core position of ADC drugs in the treatment pathway. The new guidelines emphasize that for patients who are no longer suitable for ET±TT, new ADC drugs can be used as standard subsequent treatment options, and the treatment pathway is clearer: for HR+ MBC patients who have not received chemotherapy and have HER2 low-expressing or ultra-low-expressing, T-DXd can be prioritized; while for HR+/HER2- MBC patients who have previously received chemotherapy, Dato-DXd is recommended. This stratification strategy not only reflects the shift from traditional chemotherapy to ADC drug treatment models but also establishes the key position of ADC drugs in endocrine resistance, especially in patients treated with CDK4/6 inhibitors, providing a solid foundation for achieving more individualized and precise clinical practice.
HER2 ultra-low expression status detection is first included in routine clinical practice recommendations
Another important breakthrough in the update of the ESMO guidelines is the classification of HER2 expression levels into HER2 positive, HER2 low-expressing, HER2 ultra-low-expressing, and HER2 0, and for the first time, HER2 ultra-low expression has been included as a treatment-related biomarker that needs to be routinely measured in clinical practice, indicating that for HR+/HER2-MBC: HER2 ultra-low level status should be detected through IHC [II, A]. This update aligns with cutting-edge academic trends and is more in line with current clinical practice.
The update of the ESMO guidelines regarding HER2 expression status detection is mainly based on the results of the DB06 study. The advent of trastuzumab established the treatment pattern of breast cancer as “HER2 dichotomy.” However, traditional anti-HER2 treatments have limited efficacy for breast cancer patients with low HER2 expression. The phase III DB04 study evaluated the efficacy and safety of T-DXd in HER2 low-expressing breast cancer populations.[11] The results showed that the mPFS of the T-DXd treatment group reached 9.9 months, and the mOS reached 23.4 months, significantly better than the chemotherapy group. This achievement marks the official entry of breast cancer into the “HER2 tri-classification era.” The subsequent DB06 study explored the treatment benefits of T-DXd in HR+ populations at earlier lines and lower HER2 expression levels, further clarifying the status of HER2 ultra-low expression as a subtype of HER2-targeted therapy, broadening the boundaries of anti-HER2 treatment.
Both the DB04 and DB06 studies have made significant breakthroughs in the treatment of HER2-expressing breast cancer while also raising higher requirements for pathological diagnosis. Following the announcement of the DB06 study results, Chinese scholars took the lead in formulating the “Breast Cancer HER2 Testing Guidelines (2024 Edition),” providing important theoretical support for the detection and interpretation of HER2 ultra-low expressing breast cancer.[12] The recommendation in the ESMO guidelines regarding the need to test for HER2 ultra-low expression also aligns with the philosophy of this guideline.
However, in clinical practice, due to the heterogeneity of HER2 expression in breast cancer and the uncertainty of routine pathological testing, inconsistencies in HER2 interpretation results often occur. To avoid patients missing potential treatment opportunities, multiple measures should be adopted to improve the consistency of HER2 interpretation: strictly follow HER2 testing and interpretation standards, strengthen personnel training, improve quality control systems, and actively introduce new technologies such as AI-assisted interpretation. For example, a study on AI-assisted HER2 interpretation presented at this year’s ASCO annual meeting (abstract number: 1014) showed that only the experimental cohort C used AI-assisted interpretation, while groups A and B used manual interpretation. The results showed that the accuracy of group C improved by 7% compared to groups A and B (96.1% vs 89.1%); the consistency of interpretation also significantly improved, with the Fleiss Kappa value increasing from 0.506 to 0.798; in addition, the sensitivity for HER2 0 expression, HER2 ultra-low expression, and HER2 low expression improved by 34.16%, 43.14%, and 11.71%, respectively. This study indicates that AI-assisted interpretation helps improve the accuracy of HER2 detection in breast cancer. Furthermore, it is worth emphasizing that for some HER2 IHC 0 advanced breast cancer patients, through re-reading slides, re-biopsy, and testing, they may be reinterpreted as HER2 low-expressing or ultra-low-expressing, thus obtaining the opportunity for T-DXd treatment, which has also been fully confirmed in the DB06 study.
Summary
New ADC drugs bring tremendous changes to the treatment pattern of HR+ MBC, and future treatments will become more refined and standardized. Based on the DB06 study, the applicable population for T-DXd has been expanded for the first time to HER2 ultra-low expressing (IHC >0 and <1+) populations, providing more patients with the opportunity to delay chemotherapy; while the TB01 study established the standard treatment position of Dato-DXd in chemotherapy and endocrine-treated populations. The 2025 ESMO MBC online guidelines stratify based on “sensitivity to endocrine therapy,” incorporating these two ADC drugs into treatment pathways for different clinical scenarios, providing key subsequent treatment options for patients who fail first-line treatment with CDK4/6 inhibitors. In addition, the transformation of HER2 stratification raises higher requirements for pathological diagnosis, necessitating standardized testing processes to accurately identify HER2 low/ultra-low expressing populations, ensuring that more patients benefit from targeted therapy.
Expert Profile
Professor Yang Qingmo
-
PhD, Chief Physician, Associate Professor, Master’s Supervisor
-
Deputy Director of the Breast Surgery Department, First Affiliated Hospital of Xiamen University
-
Young Scholar of the Breast Oncology Group of the Chinese Society of Clinical Oncology
-
Member of the Breast Cancer Committee of the Fujian Anti-Cancer Association
-
Deputy Chairman of the Youth Committee of the Breast Cancer Prevention and Treatment Branch of the Fujian Strait Anti-Cancer Science and Technology Exchange Association
-
Chairman of the Breast Cancer Committee of the Xiamen Anti-Cancer Association
-
Secretary-General of the Breast Disease Branch of the Xiamen Medical Association
-
Deputy Director of the Youth Committee of the Xiamen Municipal Committee of the Democratic National Construction Association
References:
[1]Trapani D, et al. Updated treatment recommendations for systemic treatment: from the ESMO Metastatic Breast Cancer Living Guideline. Ann Oncol. 2025 Aug 12.
[2]Bardia A, et al. Trastuzumab Deruxtecan after Endocrine Therapy in Metastatic Breast Cancer. N Engl J Med. 2024;391(22):2110-2122.
[3]Giuseppe Curigliano, et al. Exploratory biomarker analysis of trastuzumab deruxtecan (T-DXd)vs physician’s choice of chemotherapy (TPC) in HER2-lowultralow, hormone receptor-positive (HR+) metastaticbreast cancer (mBC)in DESTINY-Breast06(DB-06). 2025 ASCO. Abstract 1013.
[4]Bardia A, et al. Datopotamab Deruxtecan Versus Chemotherapy in Previously Treated Inoperable/Metastatic Hormone Receptor-Positive Human Epidermal Growth Factor Receptor 2-Negative Breast Cancer: Primary Results From TROPION-Breast01. J Clin Oncol. 2025 Jan 20;43(3):285-296.
[5]Pistilli, B. et al. VP1-2025:Datopotamab deruxtecan (Dato-DXd) vs chemotherapy (CT) in previously-treated inoperable or metastatic hormone receptor-positive, HER2-negative (HR+/HER2–) breast cancer (BC): Final overall survival (OS) from the phase III TROPION-Breast01 trial. Annals of Oncology, Volume 36, Issue 3, 348-350.
[6]Shusen Wang, et al. Datopotamab deruxtecan (Dato-DXd) vs chemotherapy (CT) in patients (pts) with pre-treated inoperable/metastatic hormone receptor-positive, HER2-negative (HR+/HER2–) breast cancer (BC): Results from TROPION-Breast01 China cohort. ESMO Asia 2024; Abstract 38MO.
[7]DATROWAY® Approved in Japan as the First TROP-2 Directed Therapy for Patients with Previously Treated Unresectable or Recurrent HR Positive, HER2 Negative Breast Cancer. 第一三共官网新闻.
[8]DATROWAY® Approved in the U.S. for Patients with Previously Treated Metastatic HR Positive, HER2 Negative Breast Cancer. 第一三共官网新闻.
[9]DATROWAY® Approved in the EU for Patients with Previously Treated Metastatic HR Positive, HER2 Negative Breast Cancer. 第一三共官网新闻.
[10]国家药品监督管理局官网.国家药监局批准注射用德达博妥单抗上市.https://www.nmpa.gov.cn/zhuanti/cxylqx/cxypxx/20250822150653144.html.
[11]Modi S, Jacot W, Yamashita T, et al. DESTINY-Breast04 Trial Investigators. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022 Jul 7;387(1):9-20.
[12]《乳腺癌HER2检测指南(2024版)》编写组,等.乳腺癌HER2检测指南(2024版)[J].中华病理学杂志,2024,53(12):1192-1202.
[13]David Mulder, et al. Use of artificial intelligence–assistance software for HER2-low and HER2-ultralow IHC interpretation training to improve diagnostic accuracy of pathologists and expand patients’ eligibility for HER2-targeted treatment. 2025 ASCO, 1014.* This article is for scientific information to medical professionals only and does not represent the views of this platform.