Click the “blue words” above to follow us!
Some patients with progressive supranuclear palsy (PSP) complain that their eyes “cannot be opened.” This phenomenon is often caused by blepharospasm and apraxia of eyelid opening. Today, we will share the clinical features, pathogenesis, and treatment methods of these two symptoms.
01
Clinical Features
Blepharospasm (BSP) and apraxia of eyelid opening (AEO) are common ocular symptoms in PSP patients.
Blepharospasm is a focal dystonia characterized by involuntary sustained contractions of the orbicularis oculi muscle, leading to spasmodic closure of the eyelids. When the patient tries to close their eyes tightly and then reopen them, one can observe the lowering of the eyebrows during closure and the sustained contraction of the orbicularis oculi during reopening.
Apraxia of eyelid opening, also translated as apraxia of eyelid opening, eyelid opening apraxia, is characterized by weakness in opening the eyelids; if the patient wants to open their eyes, they must assist with vigorous contraction of the frontalis muscle. PSP patients with apraxia of eyelid opening may tighten their frontalis muscle and try to pull up the upper eyelid margin to open their eyes, which often results in noticeable deep wrinkles on their forehead and raised eyebrows—this is a manifestation of their struggle to open their eyes.
Blepharospasm and apraxia of eyelid opening can occur simultaneously, and are more likely to co-occur in the late stages of PSP. They are believed to be related. Apraxia of eyelid opening can lead to ptosis; mild ptosis has little effect on vision, but severe ptosis can obstruct the pupil, affect vision, and even pose a risk of amblyopia.
 02
02
Pathogenesis
The specific pathogenesis of PSP is still unknown. The general pathological manifestation of PSP is atrophy of the cerebral hemispheres and brainstem, with the atrophy of the dorsal midbrain being the most pronounced, involving the atrophy of multiple neural nuclei in the midbrain brainstem. It is generally believed that the associated symptoms are caused by the orbicularis oculi muscle, which is innervated by the facial nerve; apraxia of eyelid opening is caused by disinhibition of the levator palpebrae superioris and orbicularis oculi at the nuclear level.
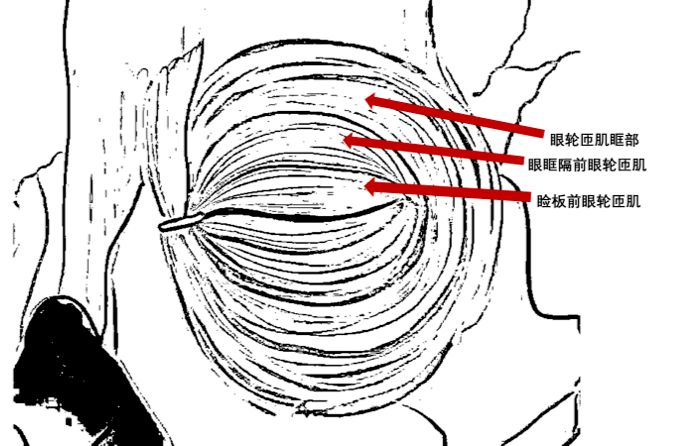
Some early clinical studies based on electromyography suggest that both blepharospasm and apraxia of eyelid opening are caused by spasms of the orbicularis oculi muscle, and different clinical symptoms result from tension disorders of different components of the orbicularis oculi muscle. Involvement of the orbital part of the orbicularis oculi can produce typical blepharospasm; isolated spasms of the pre-tarsal orbicularis oculi can lead to apraxia of eyelid opening. Patients with both blepharospasm and apraxia of eyelid opening may be affected by spasms in multiple regions of the orbicularis oculi.
Some scholars argue that apraxia of eyelid opening should be termed “focal eyelid dystonia” because “apraxia of eyelid opening” is essentially not an “apraxia”; its underlying cause is a dystonia. Compared to patients without parkinsonian symptoms who only have isolated eyelid muscle dystonia, PSP patients exhibit more pronounced symptoms of apraxia of eyelid opening, possibly because the orbital part of the orbicularis oculi in PSP patients cannot sustain contraction—thus making spasms more likely to occur.
Some case reports mention that during treatment of PSP patients, an increase in the dose of levodopa led to a worsening of apraxia of eyelid opening symptoms, which disappeared after discontinuation of the drug; a certain dose of apomorphine also caused the emergence of apraxia of eyelid opening symptoms. Some studies have also mentioned the occurrence of apraxia of eyelid opening in PSP patients receiving levodopa treatment. This reminds us that such symptoms can be caused by the disease itself or may result from the use of dopaminergic drugs.
03
Treatment Methods
The treatment of PSP still focuses on symptomatic targeted therapy, and the treatment for blepharospasm and apraxia of eyelid opening is no exception.

Botulinum Toxin A Injection Treatment
Since the 1990s, relevant case reports and even small-scale clinical studies have indicated that botulinum toxin A injection treatment has a certain improvement effect on the symptoms of blepharospasm and apraxia of eyelid opening; studies suggest that injecting botulinum toxin A at the junction of the pre-orbital and pre-tarsal parts of the orbicularis oculi can improve the eyelid movement of patients. Compared to other treatment options, botulinum toxin A injection treatment is the method with the most complete clinical evidence for treating blepharospasm and apraxia of eyelid opening symptoms; however, it should be noted that botulinum toxin A injections must be performed by experienced physicians to ensure safety and effectiveness.

Consider Adjustment of Medication Treatment
PSP patients often use dopaminergic drugs to treat parkinsonian symptoms. Although some clinical studies suggest that combining benztropine (Cogentin) with botulinum toxin A injection treatment, or even using benztropine alone, may have therapeutic effects on eyelid dystonia, the current clinical evidence supporting the benefit of using benztropine in PSP patients with eyelid dystonia is not sufficient. Since some studies have found that the use of levodopa and other dopaminergic drugs can lead to the emergence and worsening of apraxia of eyelid opening symptoms, if such symptoms occur during medication, consideration should be given to adjusting the treatment regimen.

Currently, Neurosurgical Treatment is Not Recommended
Early case reports showed that neurosurgical treatment did not benefit PSP, including pallidotomy and deep brain stimulation (DBS) of the subthalamic nucleus or pallidum. Although some studies claim that a PSP-P patient who underwent DBS of the pedunculopontine nucleus gained slight benefits; however, a study involving eight PSP-RS patients who underwent unilateral DBS of the pedunculopontine nucleus found no significant benefits and unacceptable side effects. Therefore, currently, neurosurgical treatments, including DBS, are not recommended for PSP patients.

Eyelid Support Devices
While botulinum toxin A generally has a good therapeutic effect on blepharospasm and apraxia of eyelid opening in PSP patients, some patients may not respond to higher doses of botulinum toxin after an initial good response. A case report indicated that using botulinum toxin in conjunction with eyelid support devices significantly improved the symptoms of apraxia of eyelid opening in a patient experiencing these issues—an eyelid support device is a device installed on glasses to support the eyelids.
References:
Krack P , Marion M H . “Apraxia of lid opening,” a focal eyelid dystonia: clinical study of 32 patients.[J]. movement disorders, 1994, 9(6):610.
Phokaewvarangkul O, Bhidayasiri R, How to spot ocular abnormalities in progressive supranuclear palsy? A practical review.[J] .Transl Neurodeg, 2019, 8: 20
Polo KB, Jabbari B. Botulinum toxin-A improves the rigidity of progressive supranuclear palsy[J]. Ann Neurol. 1994;35(2):237–9
+ + + + + Images and text:Yang MindyReviewed by:Tang YilinImage source:Internet (infringement deleted)
Download
Download method for APP for PSP patients

1. Scan the QR code below to download and install (You can long press the QR code to recognize the QR code in the image for download)
2. Android phones can search for “Pawai” in Tencent App Treasure to download, and Apple phones can search for “Pawai” in App Store to download