1
Introduction
c-MET [also known as MET tyrosine protein kinase or hepatocyte growth factor receptor (HGFR)] is a protein encoded by the MET gene. c-MET is crucial for embryonic development, organ growth, and wound healing. Hepatocyte growth factor (HGF) is the ligand for the c-MET receptor.
MET is typically expressed by epithelial-derived cells, but can also be found in endothelial cells, neurons, hepatocytes, hematopoietic cells, melanocytes, and neonatal cardiomyocytes; while HGF is derived solely from mesenchymal cells.
When HGF binds to c-MET, it induces dimerization, leading to activation. When these signals are abnormally activated, they initiate and sustain tumor transformation, promoting tumor cell proliferation and survival, as well as tumor invasion and angiogenesis. Abnormal activation of c-MET in tumors is associated with poor prognosis in various cancers.
In fact, abnormal expression of MET has been found in various malignancies, including renal cancer, liver cancer, gastric cancer, breast cancer, and brain cancer. Normally, only stem cells and progenitor cells can express MET, allowing these cells to undergo invasive growth to generate new tissues in embryos or regenerate damaged tissues in adults.
However, tumor stem cells can possess the abnormal ability to express MET, which should only be expressed by normal stem cells, thereby promoting tumor growth and metastasis. Overexpression of c-MET and the co-expression of its HGF ligand, leading to “autocrine” activation, are closely related to tumor formation.
2
MET Signaling Pathway and Signal Transduction
Based on the structure of HGF/c-MET, HGF can bind to c-MET, inducing c-MET homodimerization and autophosphorylation, which then activates GAB1, GRB2, SHC, and STAT3. Overall, c-MET can participate in activating several major signaling pathways:
1. RAS Pathway — This pathway mediates tumor scattering and proliferation signals induced by HGF, leading to the branching morphogenesis of tumors. HGF can induce sustained activation of RAS, thereby prolonging MAPK activity.
2. PI3K Pathway — Can be activated directly through RAS downstream or directly activated through multifunctional docking sites. Activation of the PI3K pathway can increase the activity of tumor cells by remodeling the adhesion of the extracellular matrix or recruiting sensing molecules of cytoskeleton reorganization (such as RAC1 and PAK). Activated PI3K can also enhance tumor survival through the AKT pathway.
3. STAT Pathway — Sustained activation of STAT and MAPK is essential for tumor branching morphogenesis, and MET can also directly activate the STAT3 transcription factor via the SH2 domain.
Overall, the role of MET in cancer development is primarily achieved through the following three mechanisms:
1) Activation of key oncogenic pathways (RAS, PI3K, STAT3, β-catenin, etc.);
2) Promotion of new blood vessel generation and growth within tumors to support their rampant growth;
3) Promotion of external invasion and metastasis of cancer cells; cancer cells dissociate due to the production of MMP proteases, leading to distant spread of cancer to other body parts, such as bones, liver, lungs, brain, etc.
At the same time, MET has other activation pathways. For example, DCP can induce cell proliferation through the MET-JAK1-STAT3 signaling pathway by binding to MET’s Y1234/1235, leading to autophosphorylation of c-MET in cancer cells. Additionally, c-MET can also be activated through phosphorylation of Y1234/1235, inducing cancer cells to develop resistance to chemotherapy drugs.
Moreover, paracrine HGF/c-MET can also promote glycolytic metabolism through the YAP/HIF-1α pathway. Finally, the activity of MET can also be monitored through cross-talk between c-MET and different cell membrane receptors (such as CD44, integrin α6β4, clusterin, FAS, IGF-IR, EGFR, etc.).
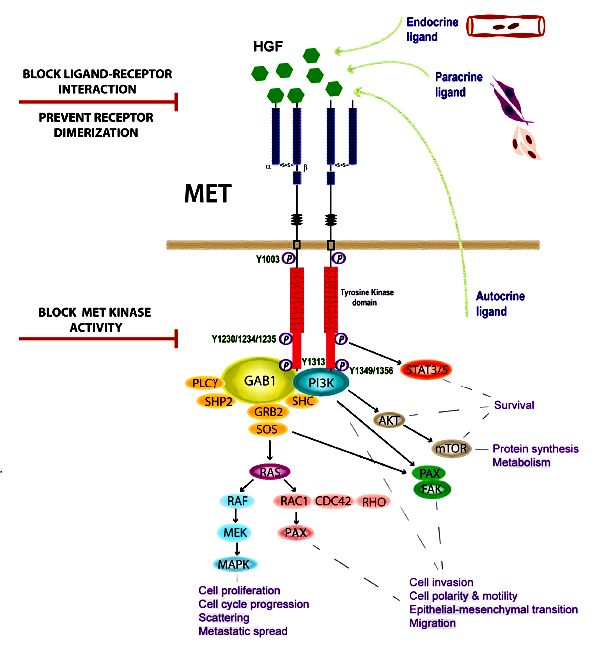
Illustration of MET signaling pathway and signal transduction (Source: Feng Y, et al, 2012)
3
Dysregulation of c-MET
Dysregulation of c-MET in cancer includes point mutations, amplifications, fusions, and overexpression of c-MET protein, all of which are associated with poor prognosis in various cancers. Previous studies have shown that MET activation is both a major oncogenic driver mutation and a driving factor for acquired resistance to targeted drugs. Overall, various types of MET dysregulation can impact the onset and worsening of cancer, as detailed below:
1.METex14 alterations (point mutations, deletions, insertions, and complex mutations) can lead to reduced degradation of the MET receptor. This results in activation of MET signaling and tumor formation.
2.MET fusion genes consist of METs lacking the adjacent regulatory sequences and different N-terminal partners. Many genes have been found to fuse with MET, such as TPR, TRIM4, ZKSCAN1, PPFIB1, LRRFIP1, EPS15, DCTN1, PTPRZ1, NTRK1, CLIP2, TFG, and HLA-DRB1, etc.
3.MET amplification is a major oncogenic factor. During the amplification of MET, the copy number of the MET gene increases, and the MET/CEP7 ratio also increases.
4.Degradation of defective MET receptors can also be one mechanism of abnormal MET signaling caused by ligands.
5.Overexpressed MET/HGF can induce tumor cell transformation by upregulating secretion signals. Although overexpression of MET protein is associated with poor prognosis in many cancers, unfortunately, using it as an indicator for the efficacy of anti-cancer drugs is not reliable. Some researchers even believe that several c-MET inhibitors that failed in phase 3 clinical trials (such as Onartuzumab, Tivantinib, and Cabozantinib) did so because they could not correctly select suitable patients.
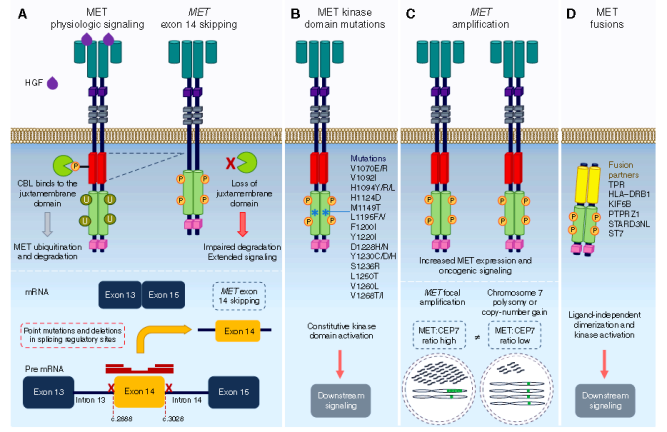
Illustration of various causes of c-MET dysregulation in cancer (Source: Recondo G, et al, 2020)
4
Mechanisms of MET in TKI Resistance
Resistance mechanisms may result from the selective pressure of cancer cells after prolonged drug exposure. In the case of c-MET, resistance can develop over time due to the presence of MET amplification subclonal populations and stimulation by paracrine and autocrine HGF. This, in turn, leads to an increase in resistant tumor subclones to c-MET therapeutic agents.
For example, in many cancers, especially non-small cell lung cancer, resistance to EGFR-TKIs is often observed due to MET amplification. The resistance rates to first and second generation EGFR TKIs are as high as 50-60%, while the resistance rates to third generation EGFR TKIs are also 15-20%. Two major published studies can help everyone understand the mechanisms of resistance to the third-generation EGFR-TKI Osimertinib.
The two studies, named FLAURA and AURA2, provided patients with first-line and second-line treatment with Osimertinib. Plasma samples from patients were subjected to next-generation genomic sequencing at disease progression or discontinuation. The results indicated that MET amplification is the most common acquired resistance mechanism; 15% of patients in the first-line treatment group had MET amplification, while 19% of patients in the second-line treatment group had MET amplification. Additionally, increased levels of HGF in tumors and stromal cells can also lead to dysregulation of the MET pathway, resulting in resistance to EGFR-TKIs.
Fortunately, several preclinical studies have shown that anti-c-MET drugs can reverse resistance to EGFR-TKI and restore sensitivity. In fact, the synergistic effect of EGF and HGF on cell proliferation has also been confirmed in other preclinical studies. This provides a basis for combination targeted drug therapy or using bispecific antibodies to treat patients (especially those resistant to EGFR-TKIs).
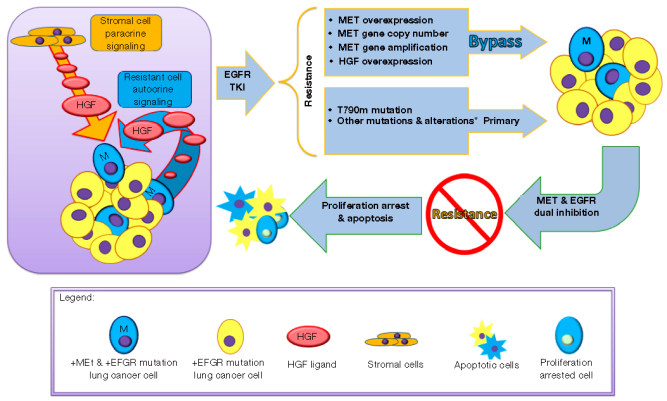 Possible mechanisms of MET in EGFR-TKI resistance (Source: Ko B, et al, 2017)
Possible mechanisms of MET in EGFR-TKI resistance (Source: Ko B, et al, 2017)
5
Development of Antibody Drugs Targeting the HGF/c-MET Axis
Generally, only patients with MET gene alterations will have objective responses after receiving anti-c-MET drugs; while for patients with wild-type MET, targeting the HGF/MET signaling pathway usually has little impact on cancer cell growth.
Recent reports indicate that anti-c-MET drugs are quite effective for patients with high levels of MET amplification or METex14 skipping mutations. Currently, several anti-c-MET drugs are under development, and this article will mainly focus on antibodies and biological agents.
a. Onartuzumab (Roche/Genentech)Onartuzumab is an interesting fully humanized monovalent/single-chain c-MET monoclonal antibody. It can block the binding of the HGF-α chain to the c-MET ligand. Onartuzumab uses knobs-into-holes technology to preferentially assemble the heavy chain and Fc chain. This special design was developed because scientists at Genentech were concerned that drugs structured as bivalent antibodies might mimic the dimerization induced by HGF. This not only fails to inhibit MET activity but may also activate the MET pathway. To address this issue, they developed a special monovalent/single-chain c-MET monoclonal antibody to ensure that the drug binds to the receptor in a one-to-one manner, thereby blocking MET pathway activity.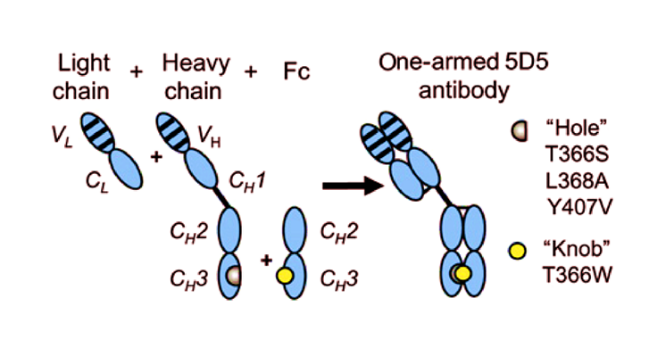 Design illustration of Onartuzumab monovalent/single-chain c-MET monoclonal antibody (Source: Merchant, et al, 2013)
Design illustration of Onartuzumab monovalent/single-chain c-MET monoclonal antibody (Source: Merchant, et al, 2013)
Genentech has conducted a total of 18 clinical trials for Onartuzumab, including phase II trials for breast cancer, colorectal cancer, and glioblastoma, as well as phase III trials for non-small cell lung cancer and gastric cancer. However, the results of most clinical trials have been disappointing. After 2015, the company has not initiated new clinical programs, and the development of Onartuzumab has stalled.
For example, in a randomized study treating patients with non-small cell lung cancer (GO27820), when comparing the efficacy of Onartuzumab combined with first-line platinum-based chemotherapy versus chemotherapy alone, the median PFS in the primary endpoint was the same in both groups, at only 4.9 months. For patients with high MET expression, the median PFS in the Onartuzumab group was 5.0 months, while the control group was 5.2 months, showing no difference.
In another phase II trial for non-small cell lung cancer patients (GO27281), Onartuzumab combined with platinum/pemetrexed/bevacizumab treatment again did not meet its primary endpoint, with a median PFS of 5.0 months for the combination group, compared to 6.8 months for the control group. In patients with high MET expression, the median PFS for Onartuzumab was 4.8 months, while the control group was 6.9 months.
Clinical data of Onartuzumab combined with EGFR-TKI were also disappointing. In a phase II clinical trial, 120 previously treated non-small cell lung cancer patients were randomly divided into two groups, one receiving Onartuzumab combined with Erlotinib, and the other receiving Erlotinib alone. The results showed that compared to the control group, the Onartuzumab combination group did not improve PFS and OS in the overall population. However, in the MET-positive subgroup, the treatment group did show prolonged PFS and OS.
Therefore, Genentech subsequently conducted a phase III randomized clinical trial involving 499 MET-positive non-small cell lung cancer patients. One group of patients received Onartuzumab combined with Erlotinib, while the other group received Erlotinib alone. The results indicated that patients in the Onartuzumab combination group performed poorly compared to the control group: ORR (8.4% vs 9.6%), PFS (2.7 vs 2.6 months), and OS (6.8 vs 9.1 months) showed no improvement. The development of Onartuzumab faced another setback, and Genentech subsequently abandoned further development.
Of course, many will later offer opinions on why this highly anticipated phase III clinical trial failed. The comprehensive viewpoints are as follows:
First, there is the issue of how to define patients as MET-positive or negative using biomarkers. Unfortunately, the IHC assay antibody used in this study to define MET negative/positive had a poor correlation with Onartuzumab; therefore, the selected patients may not have benefited from Onartuzumab treatment.
Second, the determination of MET negative/positive was made based on biopsied tissue at the initial diagnosis, but the patients actually enrolled had already received other first-line or second-line drug treatments. During subsequent treatments, the MET status of patients may have changed.
Finally, the phase II clinical data originally laid out for this phase III trial were not robust. In the Onartuzumab combination group, 20% of patients had EGFR mutations, while only 7% in the Erlotinib monotherapy group. This difference makes it difficult to assess the impact on efficacy. Of course, subsequent clinical data for other c-MET drugs have also not been outstanding, indicating that merely inhibiting the MET pathway alone may not be the most effective treatment strategy.
b. Emibetuzumab (Eli Lilly)
Emibetuzumab is a humanized c-MET IgG4 monoclonal antibody that can block the binding of HGF to c-MET, leading to the internalization and degradation of c-MET and preventing signal transduction. Eli Lilly has conducted several clinical trials for this antibody, most of which are targeting non-small cell lung cancer. Unfortunately, due to a lack of strong efficacy signals, Eli Lilly has not initiated new clinical studies since 2014, and the development of this drug seems to have been abandoned.
For example, in a phase II clinical trial, Eli Lilly attempted to assess the efficacy of Emibetuzumab + Erlotinib compared to Emibetuzumab monotherapy in MET-positive non-small cell lung cancer patients. This trial enrolled a total of 111 patients, with 28 patients receiving Emibetuzumab monotherapy and 83 patients receiving Emibetuzumab combined with Erlotinib.
The results indicated that in patients with MET expression (≥10% cells with IHC≥2+), the ORR for the combination group was 3.0%, while the monotherapy was 4.3%. In patients with high MET expression (≥60% cells with IHC≥2+), the combination group had slightly higher PFS (3.3 months vs 1.6 months) and OS (9.2 months vs 8.2 months), although the ORR (3.8% vs 4.8%) was lower than the monotherapy; of course, this slight difference is also difficult to achieve statistical significance.
Additionally, in a reverse-designed phase II clinical trial, Eli Lilly assessed the efficacy of Emibetuzumab + Erlotinib compared to Erlotinib in treating advanced non-small cell lung cancer patients with EGFR mutations. This clinical trial enrolled 141 patients, half of whom received the combination treatment, while the other half received Erlotinib monotherapy.
The results showed that in the overall population, the combination group did not show significant differences in the primary endpoint PFS compared to the monotherapy group (9.5 months vs 9.3 months), making the clinical trial a failure. Subsequently, exploratory analysis suggested that in the MET high expression (MET IHC3+) patient subgroup, the combination treatment seemed to extend PFS compared to monotherapy (20.7 vs 5.4 months); however, such post hoc analyses generally have low sample sizes, making it difficult to determine their true significance.
Overall, due to a lack of strong efficacy signals, Eli Lilly chose not to further develop this drug.
c. Rilotumumab (Amgen)
Rilotumumab is a fully humanized IgG2 monomer that can bind to the HGF-β chain, thus inhibiting the binding of HGF to c-MET. Amgen has conducted 17 clinical trials for this drug. Among them, phase II trials were conducted in renal cell carcinoma, malignant glioma, colorectal cancer, mesothelioma, ovarian cancer, and prostate cancer, while phase III trials were conducted in non-small cell lung cancer and gastric cancer.
However, the efficacy data shown is quite mediocre. For example, in a phase I/II clinical trial assessing the efficacy of Rilotumumab combined with Erlotinib in non-small cell lung cancer patients, the ORR among all 45 treated patients was 8.8%, with a median PFS of 2.6 months and a median OS of 6.6 months. Additionally, for the subgroup of 33 wild-type EGFR patients, the median PFS was 2.6 months, and the median OS was 7.0 months, showing no significant differences.
Based on these disappointing results, Amgen has not initiated new clinical studies for this drug since 2014.
d. Ficlatuzumab (Aveo)
Ficlatuzumab is a high-affinity humanized IgG1 monoclonal antibody targeting HGF, inhibiting the HGF/cMET signaling pathway by blocking HGF/cMET binding.
A phase II randomized clinical trial assessed the efficacy of Ficlatuzumab + Gefitinib compared to Gefitinib monotherapy in non-small cell lung cancer patients. Although in the overall population, the combination treatment did not significantly improve ORR (40% vs 38%), PFS (5.6 vs 4.7 months), and OS (24.7 vs 21.8 months) compared to Gefitinib monotherapy; however, in the subgroup of patients with EGFR mutations and low c-MET expression, patients receiving combination treatment showed improved ORR (41% vs 22%) and median PFS (11 months vs 5.5 months), both significantly improved.
Overall, Ficlatuzumab combined with Gefitinib shows promising efficacy in patients with EGFR mutations and low c-MET expression in small cell lung cancer, warranting further exploration.
Aveo has conducted about 10 clinical trials for this drug, including a phase I clinical trial for pancreatic cancer, as well as several phase II clinical trials for non-small cell lung cancer, head and neck cancer, and acute myeloid leukemia (AML). Currently, this antibody is the most actively developed drug among all similar drugs in clinical development.
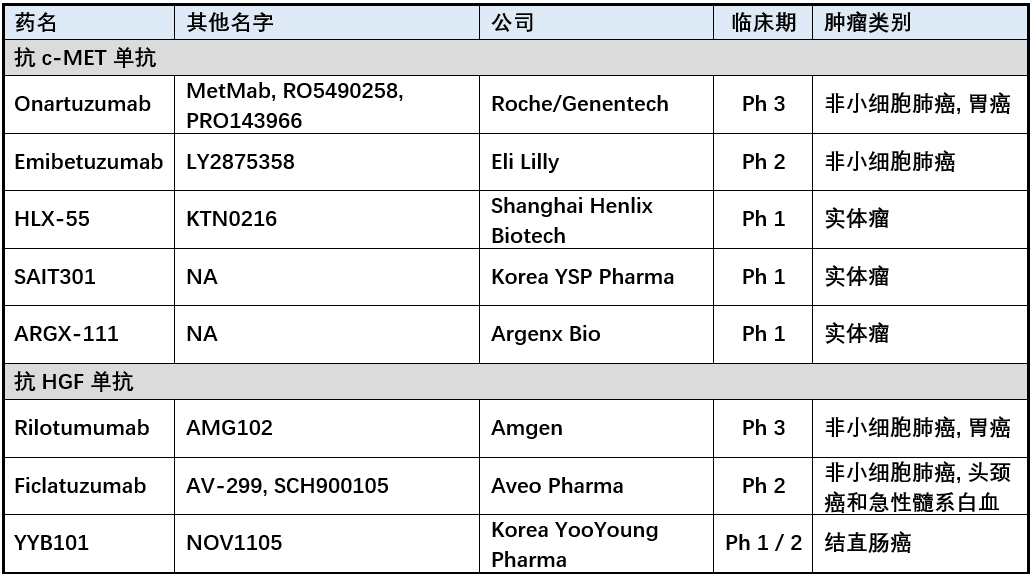
Below is a summary of the main cMET/HGF antibodies under development for readers’ reference. Several phase I new drugs currently have no public data, so they cannot be commented on.
6
Development of Small Molecule c-MET Inhibitors
Currently, several small molecule c-MET inhibitors have been marketed or are under development. However, Tivantinib and Cabozantinib have both recorded failures in phase III clinical trials. These drugs seem to be most successful in the subgroup of non-small cell lung cancer patients with METex14 mutations, such as the recent FDA approval of Tepotinib and Capmatinib is a good example. Due to space limitations, and since this article focuses on antibodies and biological agents, further elaboration on small molecule drugs will not be provided. However, for completeness, below is a summary table of major c-MET small molecule drugs for readers’ reference: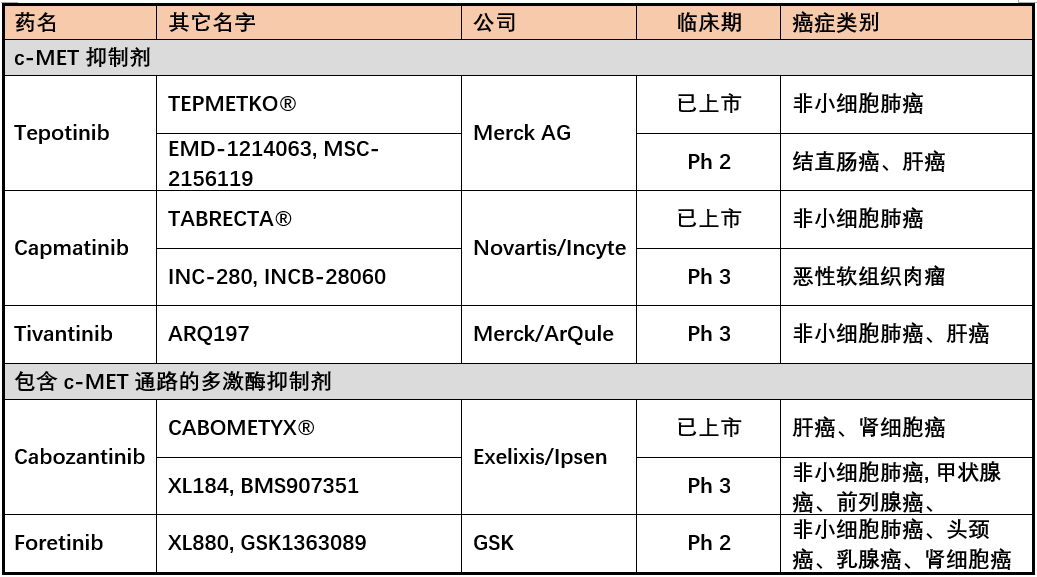
7
Immunotherapy
In today’s era of IO therapy, we certainly cannot overlook the potential role of immunotherapy in patients with MET mutations.
A retrospective study analyzed the efficacy of immunotherapy on different oncogenic driver patients among non-small cell lung cancer patients; including 36 patients with MET alterations (13 patients with MET amplification, 23 patients with METex14 skipping mutations), all of whom received anti-PD1 or PDL1 antibody drugs at different stages of treatment. In these subgroup analyses, the ORR was 16%, with a median PFS of 3.4 months and OS of 18.4 months. The efficacy seems average, but the OS data is still decent.
Another retrospective study covered 147 patients to assess PD-L1 expression, tumor mutational burden (TMB), and clinical activity of immunotherapy in METex14 lung cancer patients. Among them, the incidence of PD-L1 positivity (PD-L1≥ 1%) was 63%, while the TMB levels in patients with METex14 mutations were relatively low. Among 24 patients who received anti-PD1/PDL1 treatment, the ORR was 17%, with a mean OS of 18.2 months. However, the median PFS among 21 evaluable patients was only 1.9 months. Similar to the previous retrospective analysis, the PFS was relatively poor, but the OS was still acceptable.
Overall, these two retrospective studies indicate that IO monotherapy does not show particularly outstanding clinical performance in treating non-small cell lung cancer patients with MET alterations. Therefore, IO combined with other drugs may yield better results than using anti-PD1/PDL1 treatment alone. We look forward to more clinical studies providing data for reference in the future.
8
Future Development Directions
Although many anti-c-MET drugs have failed in phase III clinical trials in recent years, cancer patient subgroups with MET gene alterations, especially MET amplification or METex14 skipping mutations, seem to respond well to MET inhibitors. Additionally, finding suitable biomarkers for better patient selection, or using combination therapies or bispecific antibodies, are feasible directions for future development. A good example of the latter is Johnson & Johnson’s Amivantamab, a bispecific antibody targeting EGFR x cMET. (Editor’s Note: The author of this article, Dr. Mark Chiu, led the development of Amivantamab)
Amivantamab bispecific antibody can block ligand binding by combining EGFR and MET, promoting receptor degradation, and triggering ADCC in non-small cell lung cancer patients with EGFR mutations (EGFRm). A phase I clinical trial assessed the efficacy of Amivantamab in treating advanced non-small cell lung cancer patients with EGFR mutations, with interim data presented at the ASCO conference in 2019.
The trial enrolled 116 patients, of whom 97% carried EGFR mutations. Among 88 evaluable patients, 28% achieved PR. Furthermore, among 47 patients resistant to third-generation EGFR-TKI, 21% also achieved PR (4 of whom had C797S mutations, 1 had MET amplification, and 5 had no identifiable EGFR/MET gene alterations). In 20 patients with EGFR 20ins, 30% also achieved PR.
The most impressive data was that this drug had clinical efficacy in patients resistant to third-generation EGFR-TKIs (including C797S, MET amplification, and exon 20ins). Overall, Amivantamab shows promising efficacy in non-small cell lung cancer patients with EGFR mutations or resistance to third-generation EGFR-TKIs. Due to the positive data, the FDA approved this drug for marketing in May 2021 based solely on this phase I clinical data.
With the success of Amivantamab, other EGFR x cMET bispecific antibodies are also being developed. These include: LY3164530 (Eli Lilly), MCLA-129 (Merus), CKD-702 (Korean CKD Pharmaceutical), and EMB01 (Chimera Bio), all currently in phase I or phase I/II clinical development.
In China, besides Chimera Bio, Betta Pharmaceuticals has also acquired the development and sales rights of MCLA-129 from Merus and recently initiated domestic phase I/II clinical trials.
As for preclinical drugs, Merck in Germany and Samsung in Korea also have similar preclinical pipelines. Samsung even possesses a tri-specific antibody targeting EGFR x cMET x HER3. We look forward to seeing whether these drugs can yield results comparable to or even better than Amivantamab in the future.
Additionally, AbbVie also has a c-MET ADC drug Telisotuzumab Vedotin (ABBV-399) currently in clinical stages. In a phase I clinical trial, 16 MET-positive non-small cell lung cancer patients were treated with this ADC drug. The results showed an ORR of 18.8%, with a median PFS of 5.7 months and a median duration of response of 4.8 months. The safety profile is also quite good. AbbVie has conducted 6 clinical trials for this drug, most of which are for non-small cell lung cancer. In December 2021, AbbVie plans to conduct a head-to-head phase III clinical trial with this ADC drug in 600 non-small cell lung cancer patients.
We hope that more c-MET-based ADC drugs will enter clinical trials in the future to benefit patients.
9
Direction of TAVOTEK in c-MET Biologics Development
With more drugs targeting the c-MET/HGF pathway being launched, TAVOTEK currently has multiple development plans. The company aims at various development directions for c-MET-driven tumors. Since blocking c-MET through ligands is not particularly effective, it is deemed necessary to have additional pathway mechanisms as supportive treatment strategies. One direction is to target c-MET-driven tumors associated with related family receptors. In this direction, targeting these tumor tissues will require identifying different expression levels of c-MET and other receptors in the tumor microenvironment.
Moreover, these new drug molecules can also utilize immune cell activation and proliferation to target and kill tumor tissues. TAVOTEK is also very keen on developing other delivery modes, such as using ADC, ITC, or even mRNA payloads to more specifically deliver drugs to the tumor microenvironment to enhance efficacy. Finally, using c-MET as a tumor-specific marker, linking tumor tissue localization with other tumor antigens, is expected to bring more effective new drug molecules in the future with this innovative concept.
10
Conclusion
There is currently strong evidence that the HGF/c-MET pathway plays an important role in the development of various tumors. The genomic features of the HGF/c-MET pathway in cancer occurrence have also been fully demonstrated. In recent years, several anti-HGF/c-MET drugs have been launched or are in clinical trials.
However, despite the very positive preclinical data for HGF/c-MET targeted therapy in various cancers, numerous disappointing phase III clinical trials have lowered the expectations of the medical community for targeting the c-MET pathway.
Various mechanisms of c-MET activation in different cancers, including HGF/c-MET overexpression, MET gene alterations (such as mutations, amplifications, translocations, or transcriptional disruptions), and impaired MET degradation, can provide a series of good potential biomarkers in the future to better select patient subgroups.
Additionally, exploring combination therapies, including IO or other associated pathway drugs, is a feasible approach. Finally, multi-target bispecific or multispecific antibodies, or even ADCs or other effective payloads, may open a new avenue for treating c-MET-related tumors in the future. We will wait and see, with anticipation for the future.
References:
Bylicki O, Paleiron N, Assié JB, Chouaïd C. Targeting the MET-Signaling Pathway in Non-Small-Cell Lung Cancer: Evidence to Date. Onco Targets Ther. 2020; 13:5691-5706. (doi: 10.2147/OTT.S219959)
Feng Y, Thiagarajan PS, Ma PC. MET signaling: novel targeted inhibition and its clinical development in lung cancer. J Thorac Oncol. 2012; 7(2):459-67. (doi: 10.1097/JTO.0b013e3182417e44)
Ko B, He T, Gadgeel S, Halmos B. MET/HGF pathway activation as a paradigm of resistance to targeted therapies. Ann Transl Med. 2017; 5(1):4. (doi: 10.21037/atm.2016.12.09)
Mazieres J, Drilon A, Lusque A, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019; 30:1321–1328. (doi:10.1093/annonc/mdz167)
Merchant M, Ma X, Maun HR, et al. Monovalent antibody design and mechanism of action of onartuzumab, a MET antagonist with anti-tumor activity as a therapeutic agent. Proc Natl Acad Sci U S A. 2013; 110(32):E2987-96. (doi: 10.1073/pnas.1302725110).
Moosavi F, Giovannetti E, Peters GJ, Firuzi O. Combination of HGF/MET-targeting agents and other therapeutic strategies in cancer. Crit Rev Oncol Hematol. 2021; 160:103234. (doi: 10.1016/j.critrevonc.2021.103234)
Neijssen J, Cardoso RMF, Chevalier KM, Wiegman L, Valerius T, Anderson GM, Moores SL, Schuurman J, Parren PWHI, Strohl WR, Chiu ML. Discovery of amivantamab (JNJ-61186372), a bispecific antibody targeting EGFR and MET. J Biol Chem. 2021; 296:100641. (doi: 10.1016/j.jbc.2021.100641)
Park KC, Richardson DR. The c-MET oncoprotein: Function, mechanisms of degradation and its targeting by novel anti-cancer agents. Biochim Biophys Acta Gen Subj. 2020; 1864(10):129650. (doi: 10.1016/j.bbagen.2020.129650)
Recondo G, Che J, Jänne PA, Awad MM. Targeting MET Dysregulation in Cancer. Cancer Discov. 2020; 10(7):922-934. (doi: 10.1158/2159-8290.CD-19-1446)
Sabari JK, Leonardi GC, Shu CA, et al. PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers. Ann Oncol. 2018; 29:2085–2091. (doi:10.1093/annonc/mdy334)
Syed YY. Amivantamab: First Approval. Drugs. 2021; 81(11):1349-1353. (doi: 10.1007/s40265-021-01561-7)
Zambelli A, Biamonti G, Amato A. HGF/c-MET Signalling in the Tumor Microenvironment. Adv Exp Med Biol. 2021; 1270:31-44. (doi:10.1007/978-3-030-47189-7_2)
