Historically, open ileal ureter replacement (IUR) has been a reconstructive option for patients with long segment ureteral strictures that are not suitable for initial resection and anastomosis.Although IUR has proven to be an effective treatment method, its implementation is technically challenging and requires bowel reconstruction.With advancements in robotic platforms and increased accessibility to alternative tissues, the current paradigm has shifted to support the use of buccal mucosa grafts (BMG) and/or appendiceal grafts in robotic ureteroplasty to address most long segment ureteral strictures.1,2Nevertheless, the most destructive long segment ureteral strictures may not be suitable for reconstruction using robotic ureteroplasty with BMG and/or appendiceal grafts.For BMG ureteroplasty, the technique requires a healthy ureteral plate to suture the BMG, as the BMG should not be tubularized.While augmenting anastomotic BMG ureteroplasty for obstructive defects is possible, this technique still necessitates an anastomosis to the ureteral plate, which greatly limits the length of stricture that can be repaired using this technique.2Regarding appendiceal ureteroplasty, although the appendix may be inserted into the obstructed ureteral defect, this technique relies on a patent and sufficiently long appendix, which may not be available.1For long segment ureteral strictures that cannot be reconstructed using BMG and/or appendiceal ureteroplasty (Figure 1), IUR remains an important tool for reconstructive urologists.
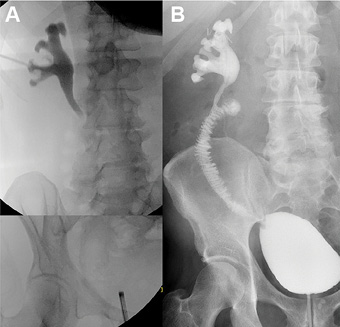
Figure 1.Long segment ureteral stricture disease unsuitable for buccal mucosa graft and/or appendiceal ureteroplasty before (A) and after (B) robotic ileal ureter replacement.
IUR was first described by Shoemaker in 1906, 3and later popularized by Goodwin et al. in the 1950s.4This technique is traditionally performed through a midline incision, involving the insertion of a segment of ileum at the site of the ureteral stricture to allow unobstructed urine flow from the kidney to the bladder.IUR is technically challenging as it often requires a large surgical field (operating on both the upper and lower urinary tracts), ureteral identification, and assessment of tissue viability (often in the context of prior surgeries, urological tumors, and/or radiation), as well as harvesting a segment of bowel.Despite large series demonstrating excellent success rates of 69% to 96% for open IUR,5,6it is also associated with a postoperative complication rate of 29.8% to 42.9% within 30 days.5,7The majority of reported postoperative complications are infectious (i.e., pyelonephritis and intra-abdominal abscesses), wound-related (i.e., dehiscence and hernias), and bowel-related (i.e., obstruction, internal hernias, and bowel obstruction).While there are concerns regarding the risk of metabolic acidosis due to urine reabsorption, this complication has been reported to occur at a relatively low incidence (2.9%-12%).5,7Moreover, most cases of metabolic acidosis can be managed with oral medications, and reoperation is rarely required.
To reduce the morbidity associated with open IUR and improve outcomes, several reports have evaluated the safety and efficacy of robotic IUR.The robotic approach is particularly well-suited for complex surgeries like IUR, as it retains the benefits of minimally invasive surgery, such as improved aesthetics, reduced wound complications, and decreased postoperative pain, while allowing surgeons to visualize and operate in a magnified 3D view. Limited anatomical space, precise suturing.Given that open IUR typically requires large incisions, the robotic approach can reduce wound-related complications and discomfort (Figure 2).Additionally, since many patients requiring IUR suffer from iatrogenic ureteral transection and/or radiation injury,identifying the ureteral anatomy and residual ureter may be challenging.Intravenous indocyanine green injection followed by near-infrared fluorescence visualization may assist in identifying viable proximal ureter/kidney pelvis (Figure 3).Furthermore, the complexity of the surgery emphasizes the importance of utilizing well-perfused tissue for reconstruction.Injecting indocyanine green and subsequently visualizing under near-infrared fluorescence may help assess ureteral perfusion after ureterolysis and bowel perfusion after harvest.We find that assessing the perfusion of harvested bowel for reconstructive urology can provide additional assurance,especially when the ileum is difficult to anastomose with the proximal ureter/kidney pelvis and requires more extensive mesenteric mobilization.Despite the potential advantages of robotic IUR, the procedure remains technically demanding.The large surgical field (Figure 4) may require multiple patient and/or port placement configurations to optimize robotic access to the upper and lower urinary tracts.Moreover, working with bowel in the robotic setting has a significant learning curve.While there are no specific data on the learning curve for robotic IUR, literature regarding robotic radical cystectomy with intracorporeal urinary diversion suggests a learning curve of approximately 140 cases.The procedure remains technically demanding.The large surgical field (Figure 4) may require multiple patient and/or port placement configurations to optimize robotic access to the upper and lower urinary tracts.Moreover, working with bowel in the robotic setting has a significant learning curve.While there are no specific data on the learning curve for robotic IUR, literature regarding robotic radical cystectomy with intracorporeal urinary diversion suggests a learning curve of approximately 140 cases.8
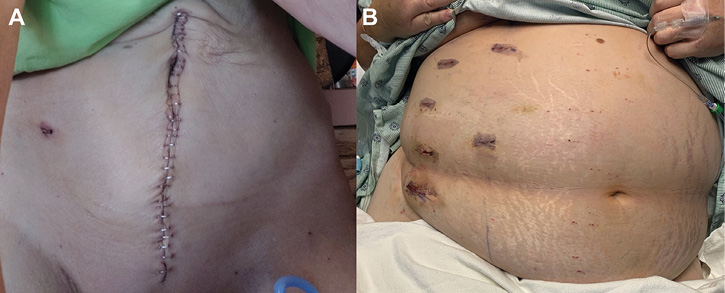
Figure 2.Incisions used for performing open (A) and robotic (B) right ileal ureter replacement. |
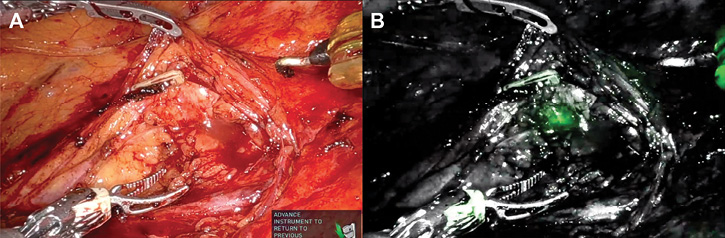
Figure 3.ADue to severe periureteral fibrosis, the ureter is difficult to identify under white light.B, after indocyanine green injection into the ureter, visualization under near-infrared fluorescence allows identification of the proximal ureter through severe periureteral scarring. |
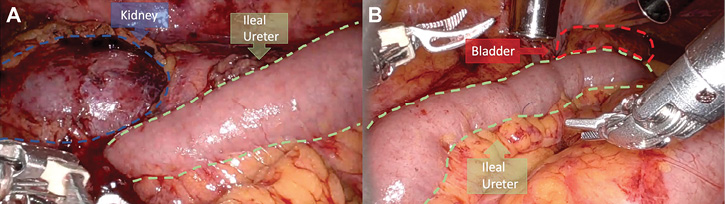
Figure 4.Complete ileal ureter shows a large surgical field.A, anastomosis of the ileal segment to the kidney pelvis.B, anastomosis of the ileal segment to the bladder. |
Currently, the literature on robotic IUR is limited to small single-center case series.In the largest series to date, Yang et al. reported on 15 patients who underwent intracorporeal robotic IUR.9At a median follow-up of 14 months, they reported a subjective success rate (defined as no urinary hardware and symptoms, and no radiographic evidence of obstruction) of 100.0%.The authors reported no major (Clavien >2) complications.While single-institution reports on robotic IUR do provide some insights into the safety and efficacy of the procedure, further studies on larger patient populations are necessary.However, generating large robotic IUR series is challenging due to the rarity of patients with long segment ureteral strictures who are unsuitable for BMG and/or appendiceal ureteroplasty.To this end, we have established a multi-institutional collaboration with New York University and the University of Colorado.Our unpublished cohort currently consists of 39 patients who underwent intracorporeal robotic IUR.The median follow-up time is 14 months, with a success rate of 90.9%.The rate of major (Clavien >2) complications is 20.5%, similar to that reported in the open IUR literature.Through our multi-institutional collaboration, we hope to recruit more surgical members to expand the study population, assess long-term success rates and complications, and prospectively address clinically significant questions.
-
Jun MS, Stair S, Xu A, et al. A multi-institutional experience with robotic appendiceal ureteroplasty. Urology. 2020;145:287-291.
-
Lee Z, Lee M, Koster H, et al. A multi-institutional experience with robotic ureteroplasty with buccal mucosa graft: an updated analysis of intermediate-term outcomes. Urology. 2021;147:306-310.
-
Shoemaker J. Discussie op voordracht van J. M. van damn over interabdominale plastiken. Ned Tijdschr Geneesk. 1911;836.
-
Goodwin WE, Winter CC, Turner RD. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter. J Urol. 1959;81(3):406-418.
-
Armatys SA, Mellon MJ, Beck SD, et al. Use of ileum as ureteral replacement in urological reconstruction. J Urol. 2009;181(1):177-181.
-
Zhong W, Hong P, Ding G, et al. Technical considerations and outcomes for ileal ureter replacement: a retrospective study in China. BMC Surg. 2019;19(1):9.
-
Monn MF, Roth JD, Bihrle R, Mellon MJ. Long term outcomes in the use of ileal ureter for radiation-induced ureteral strictures. Int Urol Nephrol. 2018;50(8):1375-1380.
-
Wijburg CJ, Hannink G, Michels CT, et al. Learning curve analysis for intracorporeal robot-assisted radical cystectomy: results from the EAU Robotic Urology Section Scientific Working Group. Eur Urol Open Sci. 2022;39:55-61.
-
Yang K, Wang X, Xu C, et al. Totally intracorporeal robot-assisted unilateral or bilateral ileal ureter replacement for the treatment of ureteral strictures: technique and outcomes from a single center. Eur Urol. 2023;84(6):561-570.