In the world of oncology, HER2 (human epidermal growth factor receptor 2) used to represent a simple boundary—positive meant eligibility for treatment; negative meant no access to targeted therapy..
However, with the advent of antibody-drug conjugates (ADCs), this boundary has begun to blur.
This article published in Gynecologic Oncology illustrates that:HER2 is no longer a matter of “present” or “absent,” but rather a question of “a little more,” “a little less,” or “is it sensitive enough?”
Traditionally, HER2 positive meant IHC 3+ or FISH gene amplification, allowing patients with breast cancer to use drugs like trastuzumab and pertuzumab.
However, it was later discovered that even patients with non-strongly positive HER2 could benefit from ADCs.
Thus, the concept of “HER2-low” was born—HER2-low means the receptor is still present, just in limited quantities.
ADC drugs (such as T-DXd) utilize antibodies for “precise delivery” of toxins, allowing them to be effective even with limited receptor numbers.
This has fundamentally changed the fate of HER2.
So the question arises: In endometrial cancer, how prevalent is HER2-low? In which types is it commonly found?
This is precisely what the SPECTRUM study aims to answer.This research from Leiden University in the Netherlands collected 193 cases of molecularly classified endometrial cancer—ranging from low-grade endometrioid carcinoma to high-grade serous carcinoma, comprehensively testing HER2 expression and comparing three international scoring systems (breast cancer, gastric cancer, endometrial cancer).
The results are quite interesting:
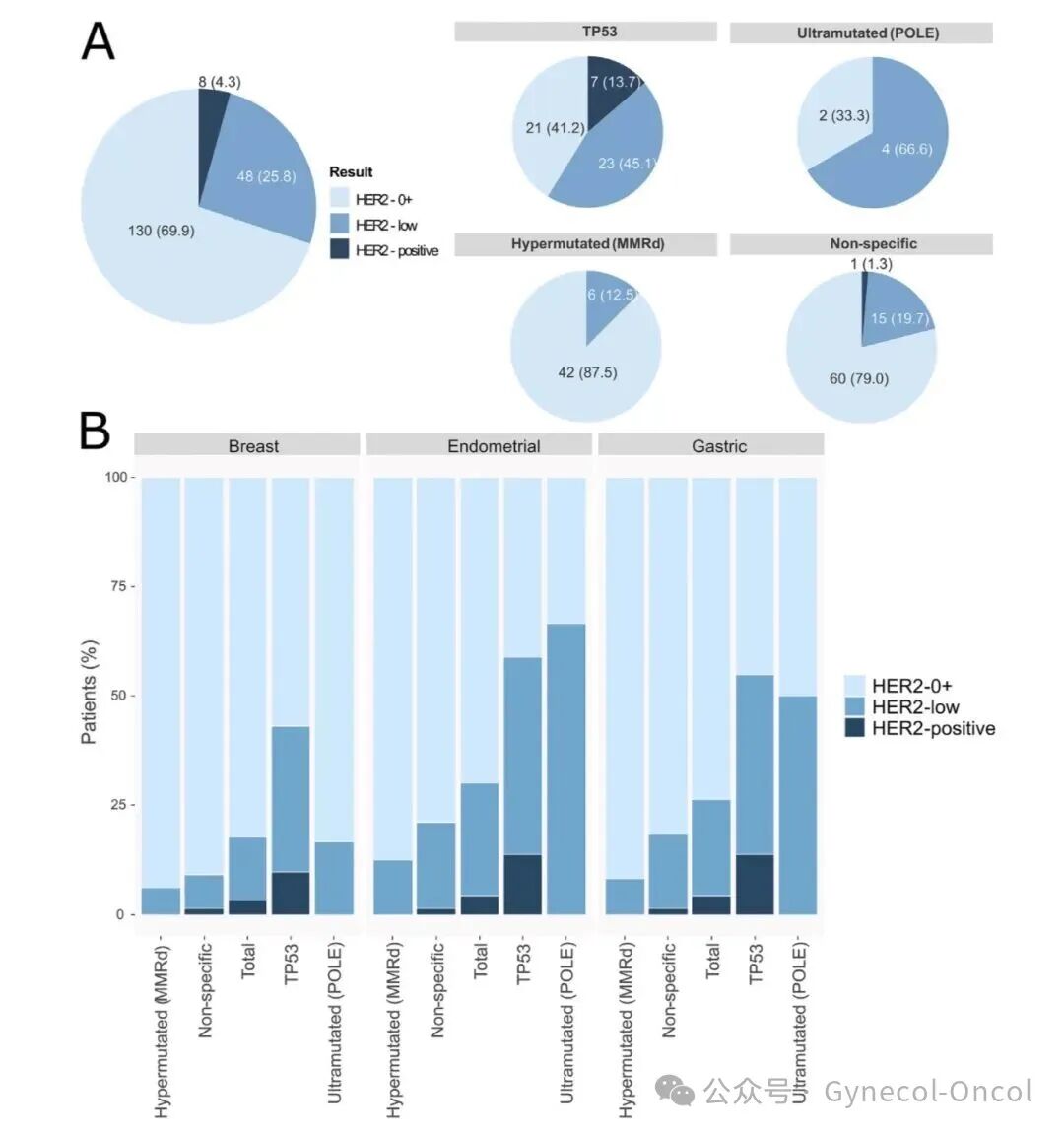
In all cases, HER2 0 level accounted for about 70%, HER2-low about 26%, and HER2 positive only 4%.
HER2-low is not only found in serous carcinoma:
About 52% of serous carcinoma is HER2-low;
About 70% of clear cell carcinoma;
About 48% of high-grade endometrioid carcinoma;
Only about 8% of low-grade endometrioid carcinoma.
If we look at molecular classification (TCGA four types):
In the POLE mutation type, the proportion of HER2-low is as high as 67%;
In the p53 abnormal type, it is also 45%;
MMRd and NSMP types are relatively lower.
In other words:
HER2-low is quite common in endometrial cancer, especially concentrated in patients with p53 abnormal and POLE mutation types.
This suggests that the future population eligible for HER2 ADC drugs may far exceed our current imagination of “serous carcinoma.”
SPECTRUM study also found significant differences between different interpretation standards:
If breast cancer standards are used, the detection rate of HER2-low will be underestimated;
Whereas the endometrial cancer-specific standard (Endometrial HER2 Scoring) not only has the best consistency but can also detect more low-expression cases.
Researchers suggest that future HER2 reports should clearly state which standard is used and define “0 score” as “completely no staining” to avoid misjudgment.
ADC: Opening the Door for HER2-low
The core of ADC drugs lies in “bridging”:
Antibodies recognize HER2 and deliver chemotherapy toxins, which release “bombs” once inside the cell, also having a bystander effect on adjacent cells.
This means that even with low HER2 expression, it may be sufficient to “receive the bomb” and achieve cell killing.
The DESTINY-PanTumor02 study has already shown that patients with various solid tumors (including endometrial cancer) who are HER2-low may benefit from T-DXd.
The significance of SPECTRUM lies in that it provides a “map” for these future clinical trials—telling researchers where to find HER2-low patients.
Conclusion
-
Testing should be comprehensive: Not only serous carcinoma but also clear cell carcinoma and high-grade endometrioid carcinoma should be tested for HER2.
-
Reports should be standardized: Use endometrial cancer-specific interpretation standards, indicating “0 score definition” and FISH status.
-
Re-testing upon recurrence: A small number of patients may change HER2 status upon recurrence, and re-testing can help with precise medication.
-
Future ADC pathways: Future ADC research should prioritize HER2-low patients with p53 abnormal and POLE mutation types.